





Figures
- Figure 1
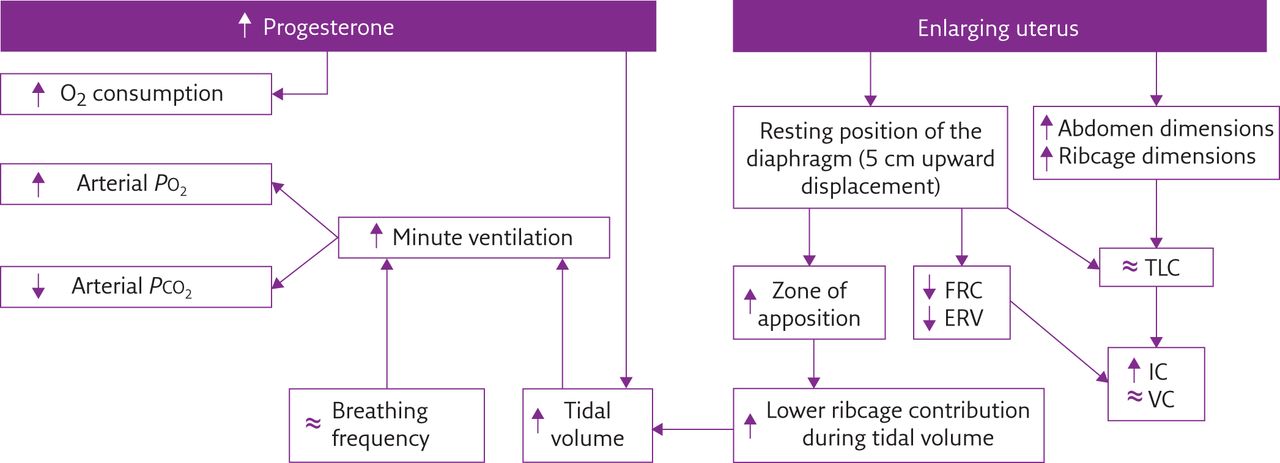
Flow diagram summarising the most important effects of biochemical (left) and mechanical (right) pregnancy-induced factors on pulmonary function, ventilatory pattern and gas exchange. PO2: oxygen tension; PCO2: carbon dioxide tension; FRC: functional residual capacity; ERV: expiratory reserve volume; TLC: total lung capacity; IC: inspiratory capacity; VC: vital capacity; ↑: increased; ↓: decreased; ≈: no change.
{kind=link}
Tables
- Table 1
Principal features to consider when treating unhealthy pregnant women
Disease Features and/or indications Asthma [15] Recommended use of corticosteroids to prevent critical illness Oral corticosteroids associated with a two-fold increase in pre-eclampsia and with a minimal incidence (0.4%) +of oral clefts (if taken in the first trimester) Pulmonary oedema [15] Cardiogenic basis secondary to haemodynamic factors occurring during pregnancy: ↑ cardiac output ↑ heart rate ↓ systemic vascular resistance ↓ colloid osmotic pressure A consequence of tocolytic therapy and of pre-eclampsia If no improvement within 24 h after diuresis, invasive haemodynamic monitoring and/or rapid antihypertensive therapy are required Severe restrictive lung disease [10] Risk of hypoxic and hypercapnic respiratory failure because the ability to increase ventilation is limited Severely reduced vital capacity but pregnancy can be well tolerated Minimal complication: preterm delivery with newborn needing high-dependency support Lung function and oxygen saturation should be monitored Supplemental oxygen and noninvasive ventilation may be required Pre-eclampsia [16] The most common obstetric disorder, with multisystem ramifications ↑ minute ventilation because of ↑ concentration of blood leptin (a ventilation-stimulating hormone) ↓ vital capacity secondary to lower transverse section area of the upper airways, pharyngeal oedema and excessive weight gain with higher adipose deposition around the neck ↓ exercise tolerance Respiratory muscle function is not affected Heart and lung transplantation [17] Better to avoid conception within the first 1–2 years after transplantation Potential pregnancy-related complications: prematurity, low weight at birth and postpartum graft loss Maintenance of immunosuppression with close monitoring of cyclosporine blood levels during gestation Accurately diagnose signs of pre-eclampsia, as it is a multi-organ disease Hereditary neuromuscular disorders [18] Identify the highest risk group according to the diaphragmatic and/or bulbar involvement of the disease ↑ respiratory muscle load by higher airway resistance and impaired bulbar load, leading to overwhelmed respiratory muscle capacity Hypoventilation Monitor the respiratory and cough function Maximise airway clearance High aspiration risk in the third trimester because of ↑ abdominal pressure and ↓ gastro-oesophageal sphincter tone ARDS [19] Non-obstetric causes: sepsis, pneumonia, intracerebral haemorrhage, blood transfusion and trauma Obstetric causes: amniotic fluid embolism, pre-eclampsia, septic abortion, retained products of conception and complication from tocolytic therapy Management includes: prompt antibiotic therapy, conservative fluid strategy, use of mechanical ventilation and extracorporeal life support in case of refractory ARDS Mechanical ventilation [20] Similar indications to those for non-pregnant patients, with some exceptions: Oxygen therapy may also help fetal distress Consider that PCO2 in pregnancy is about 30 mmHg when interpreting arterial blood gases Airways are narrow (consequence of mucosal surface hyperaemia), so it is preferable to perform endotracheal intubation via oral route using a smaller tube ↓ oxygen reserve of the mother, so use pre-oxygenation with 100% oxygen during intubation to avoid arterial desaturation after a short period of apnoea Better to avoid respiratory alkalosis as it leads to problems in uterine blood flow and fetal oxygenation Treat respiratory acidosis with bicarbonate ARDS: acute respiratory distress syndrome; ↑: increased; ↓: decreased.
Vol 11 Issue 4
Table of Contents

Respiratory physiology of pregnancy









