Article Text

Abstract
In spite of the consistency of the primary discharge coordinator in our practice and attempts to streamline the process, the obstacles to discharge highlighted five years ago remain frustratingly similar. The children in this survey spent an average of 9.6 months extra time in hospital awaiting discharge at considerable cost to the local commissioning teams, quite apart from the emotional cost to the child and stress for the whole family. We hope in future years this review will enable health practitioners and local health providers to anticipate the hurdles, address the problems early, and expedite the process of discharging home children who are dependent on long term ventilation via tracheostomy.
- discharge
- home ventilation
- tracheostomy
- BPD, bronchopulmonary dysplasia
- CCHVS, congenital central hypoventilation syndrome
- CLD, chronic lung disease
- DGH, district general hospital
- ECMO, extracorporeal membrane oxygenation
- GOSH, Great Ormond Street Hospital
- HOCM, hypertrophic obstructive cardiomyopathy
- ICU, intensive care unit
- LTV, long term ventilation
- PCT, Primary Care Trust
- TCU, transitional care unit
Statistics from Altmetric.com
- BPD, bronchopulmonary dysplasia
- CCHVS, congenital central hypoventilation syndrome
- CLD, chronic lung disease
- DGH, district general hospital
- ECMO, extracorporeal membrane oxygenation
- GOSH, Great Ormond Street Hospital
- HOCM, hypertrophic obstructive cardiomyopathy
- ICU, intensive care unit
- LTV, long term ventilation
- PCT, Primary Care Trust
- TCU, transitional care unit
Advances in neonatal and paediatric intensive care have reduced mortality, but have introduced a new morbidity: a growing number of children who are medically stable but require 24 hour ventilatory support.1,2 However, life in hospital is an unsuitable environment for the developing child and an inappropriate use of resources.3 In 1998 guidelines produced by the UK Working Party on Paediatric Long Term Ventilation (LTV)4 suggested that with appropriate support and careful planning, long term ventilation for children in the home was feasible. Due to the nature of the work involved, the responsibility for transitioning a ventilated child from hospital to home not uncommonly falls into the hands of neonatologists, paediatric intensivists, and respiratory paediatricians in tertiary centres. However once home, the responsibility rests with general paediatricians, nurses, and allied health professionals attached to district general hospitals (DGH).
In 1999, a cross sectional survey on 141 children from paediatric respiratory consultants and intensivists from around the United Kingdom,2 reported that 24% were ventilated via a tracheostomy, and 68% were cared for at home. The report predicted that only 4% would remain institutionalised. The survey highlighted specific obstacles to discharge; failure to recruit qualified nursing staff or trained carers; delay in obtaining funding; and unsuitable housing. We know of no reports in the United Kingdom on the long term outcomes for this group of children.
We describe our experience over the past seven years of coordinating the discharge home of 39 children from Great Ormond Street Hospital (GOSH) on tracheostomy dependent ventilation. We examine outcomes for this specific group of children, and discuss issues relevant to the wide variety of health professionals who are involved in the complexities of discharging a child home on tracheostomy dependent ventilation.
METHODS
Since 1994, the GOSH sleep service has identified 146 children requiring long term ventilatory support. The majority of these children were ventilated by non-invasive mask interface. These children require simple care packages and have been reviewed recently.5 For this article we reviewed the details of 39 children who, at the time discharge planning was initiated, were the most technology dependent: children dependent on ventilation via tracheostomy who cannot survive for more than 24 hours without ventilatory support. Following multidisciplinary assessment (including ethical considerations and parental views), all were considered suitable for home ventilation, and all but four were discharged from GOSH between January 1995 and November 2002. The key discharge coordinator was a social worker (MO). The funding responsibilities for the 39 children were under the jurisdiction of 23 health authorities or more recently Primary Care Trusts (PCT). No more than four children were supported by any one funding agency, and the majority of the Trusts (12/23) were only responsible for funding one child.
At the time of the survey, six of the 39 children were in hospital. The details of these six children are included in keeping with the inherently fluid nature of the discharge process: one child has remained in hospital for over four years, and is included to illustrate that not all children get home; another child, successfully discharged home, was readmitted following a change in medical and home circumstances.
RESULTS
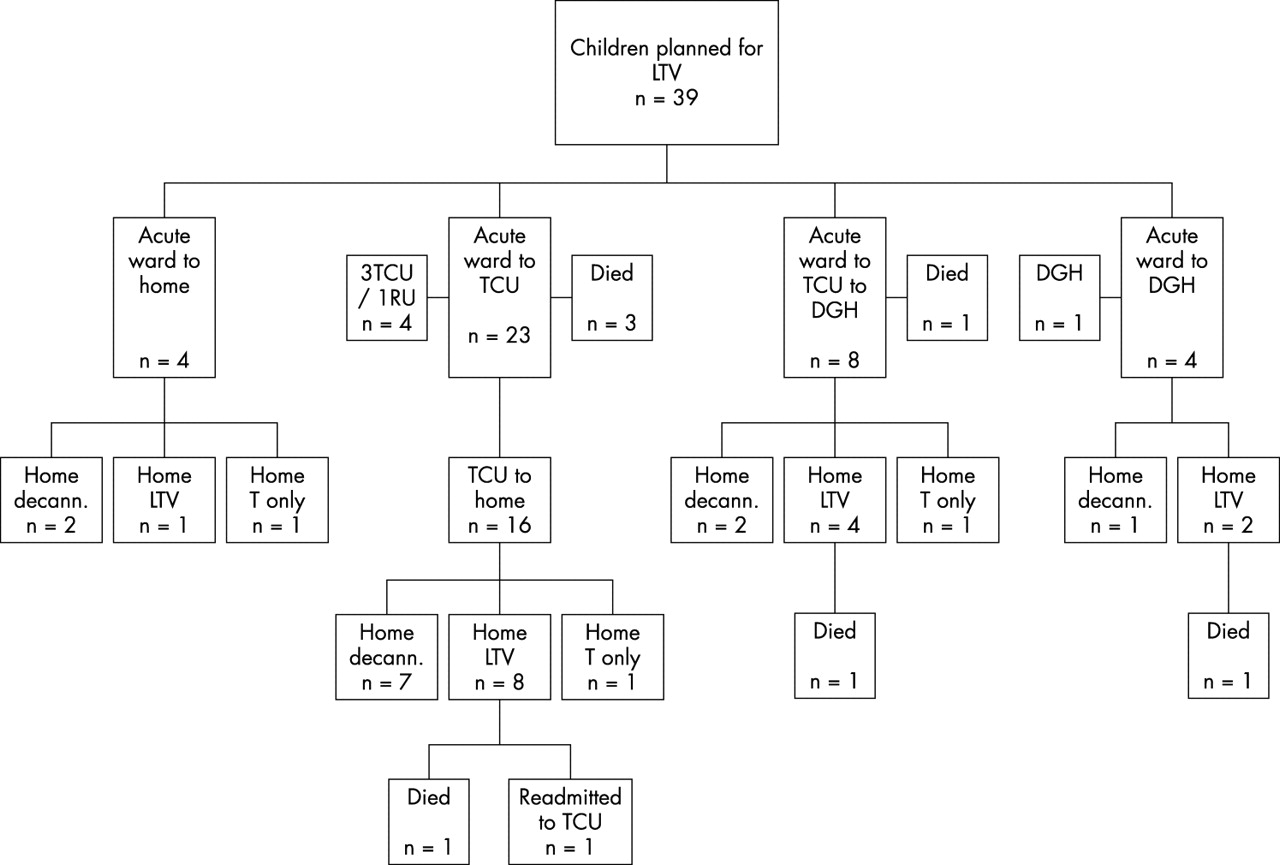
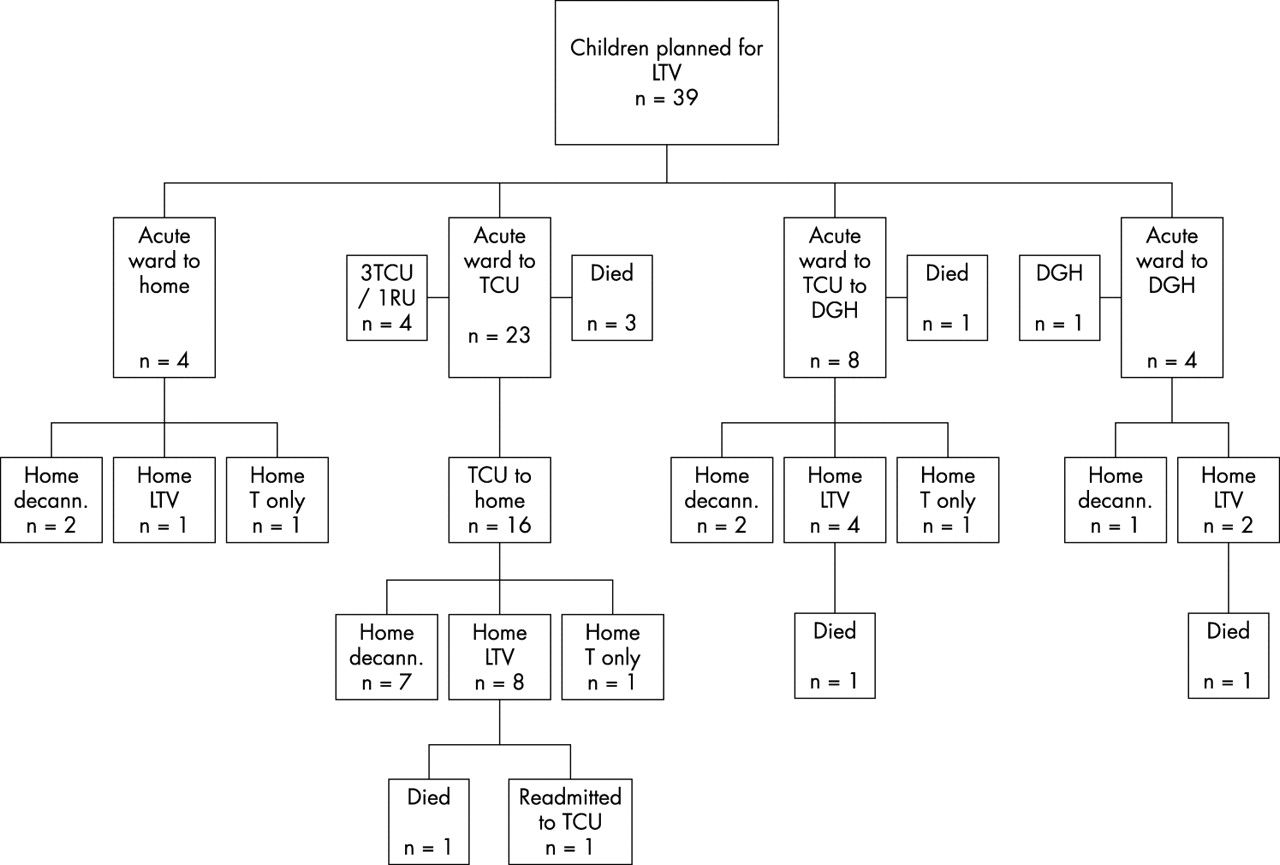
Table 1 summarises details of the 39 children including the age when planning for LTV was initiated, time spent in hospital before discharge, the age now (November 2002), the principal diagnosis resulting in the need for LTV, the respiratory outcome to date, and the number of years that ventilatory support has been provided at home. Twenty nine (74%) of the children required ventilation for 24 hours of the day, and the remaining 10 required either nocturnal ventilation or ventilation when they were asleep, day or night. The median age at the time discharge planning was started was 10.8 months (range 3.6 months to 14 years). The commonest reason for needing LTV was an abnormality of the airway (tracheobronchomalacia or tracheal stenosis), combined with underlying chronic lung disease of prematurity or secondary to a variety of respiratory pathologies (21/39, 54%) (for example, meconium aspiration, congenital diaphragmatic hernia, pulmonary hypoplasia). Three children out of the cohort had required tracheal stenting. Seven children (18%) had neuromuscular disease (for example, myopathy (three cases), myasthenia gravis, muscular dystrophy, HSMN type II, polyneuropathy). One child had congenital central hypoventilation syndrome (CCHVS). Three children required LTV following trauma or acute illness: two cases of spinal cord injury, and one case of severe head injury. Six cases had underlying medical syndromes (trisomy 21 (two cases), Noonan’s syndrome (two cases), 3C syndrome (one case), Shprintzen’s syndrome (one case)). Five cases had complex cardiac disease that included two cases of hypertrophic obstructive cardiomyopathy (HOCM), and cardiac conditions associated with the medical syndromes. Nine children had significant gastro-oesophageal reflux disease requiring gastrostomy feeding and Nissen’s fundoplication. Although all the children in the series had required prolonged conventional ventilation before stability was achieved, only one child had been supported with extracorporeal membrane oxygenation (ECMO). Figure 1 tracks the children’s journey after they left the original acute in-patient location at GOSH.
Case histories of 39 children requiring ventilation via tracheostomy
{kind=link}
Flow diagram of the journey from the acute inpatient location. LTV, long term ventilation; TCU, transitional care unit; DGH, district general hospital; T, tracheostomy; RU, respiratory unit; decann., decannulated; acute ward, intensive care or high dependency unit.
OUTCOMES
Twenty seven children were successfully discharged home (median age 4.8 years, range 1.5–22.6 years), having spent a median of 9.6 months (range 3.6 months to 3.5 years) awaiting discharge. Seven children died, but none as a result of failure of ventilatory support at home. Fifteen of the discharged children successfully came off all ventilation. Twelve had a combination of CLD and an upper airway abnormality. The median age of the children now off ventilation is 4.7 years (range 2.2–7.5 years). Eleven children (median age 5 years, range 1.5–22.6) remain at home ventilated (median time ventilated at home 3.4 years, range 0.2–5.1 years), seven have neurological or muscular disease. One child (case 22) has been readmitted to the TCU but had been home for 1.8 years before readmission, and is expected to return home. Excluding the children in hospital, of the 11 children ventilated at home, five children remain on 24 hour ventilation and six have ventilatory support when they are asleep. There was only one child (child 35) who is unlikely to be discharged home, and has the longest hospital stay of the group (4.4 years). Table 2 summarises the ventilatory outcomes.
Summary of ventilatory outcomes
The level of mobility and schooling of the 32 surviving children were noted as crude measures of neurological function. Eleven were normally ambulant, seven wheelchair dependent, and 10 were ambulant but still used a wheelchair outside the home. The remaining four children were below 18 months of age. Six children attended mainstream school, five attended a special school, 15 were preschool, and two other children’s schooling was unknown.
In summary, whereas all of the group were dependent on ventilation when discharge planning was initiated, at the time the survey was completed only 43% were dependent, 38% had successfully come off ventilatory support, and 18% had unfortunately died. Of the surviving children 34% had normal mobility, 22% were wheelchair dependent, and 17% were ambulant but used a wheelchair outside the home. Nearly half were of preschool age; however, 19% attended mainstream school, and 16% attended special schools.
COMPARATIVE EXPERIENCES
There have been a number of surveys outlining paediatric programmes and guidelines for children who require long term ventilation from many centres around the world including the United Kingdom,2,4,6 Canada,7 America,8 France,9 Switzerland,10 and Japan.11 Despite this there is limited information specifically on children at home on ventilation via a tracheostomy and their long term outcomes. The largest prospective study from France reported on outcomes of a heterogeneous group of children, and only 16 of the 158 on mechanical ventilation were supported via tracheostomy. A 15 year review from Italy described their experience of long term ventilated children.12 Forty six children were followed, six died in the ICU, and one child remained in the ICU. Two children could not be discharged due to insufficient parental skill and a poor domestic environment. Of the 37 who were alive at home, four were decannulated (two had bronchopulmonary dysplasia (BPD) and two had tracheomalacia). Like our survey all had tracheostomies in situ, and 61% (28/46) had gastrostomy tubes. The median time of ventilation at home was 4.6 years (range 2 months to 15 years). Twelve children had abnormalities of the upper airway, 13 had neuromuscular disorders, three had BPD, three had tracheomalacia, and two had central hypoventilation syndrome. Thirty five per cent required temporary readmissions to hospital for various acute medical and elective surgical procedures.
COMMON DELAYS TO THE DISCHARGE PROCESS
Fraser and colleagues’ review in 1998 of 40 chronically ventilated children highlighted that nearly three quarters of the hospital stay was spent awaiting discharge.1 Sixty five per cent required a tracheostomy, 25% required ongoing mechanical ventilation, and only one was at home. Previously the UK guidelines4 and other reports13,14 suggested that the major discharge obstacles for chronically ventilated children were failure to recruit qualified nursing staff or trained carers, delay in obtaining funding, and unsuitable housing. Our cross-sectional survey found that the most common obstacles to discharge were funding for staffing and equipment, and local organisational delays (defined as delays in decision making at a local level), which both occurred in 41% of the cases. In 33% of cases the families’ housing was unsuitable or needed major alterations. Significant family or social reasons were obstacles to discharge in 15% of cases, and in two cases the children were fostered. In 15% of cases the child’s medical condition changed and affected the level of support required at home. Our experience suggests that although the number of children who fail to be discharged home is still very small, considerable obstacles remain which make hospital care more protracted. Four key causes of delay are discussed further.
Staff recruitment
It is accepted that children requiring ventilation via a tracheostomy need constant supervision, and that at home parents will need a minimum of seven nights care a week. The amount of help provided by day however will depend on the child’s condition, the degree of dependence on ventilation, and family factors. Three children in our survey went home without any carer support, one because the family got frustrated waiting, took the child home themselves, and gave up work. Two children had come off ventilation and only had a tracheostomy in situ when they were eventually discharged home.
Recruitment of trained paediatric nurses is a national problem and is one cause of delayed discharge for this group of children. However, it is possible for one lead nurse to train and support suitable applicants (such as trained nursery nurses) to be health care assistants for ventilated children. In addition our experience is that using an agency specialising in this area can speed up the discharge process. One child had been referred for palliative care and after a delay while attempts were made to recruit suitable staff, finally went home with agency care and died one week later. The parents bitterly regret the months spent in hospital rather than at home.
Although local providers may reduce management costs by trying to employ their own teams, this creates delays. In two cases the local team found they were unable to recruit a lead nurse and after 9 and 7 months respectively used an agency. In the case of another child the local providers took 10 months to establish the local team by which time the child, who had spent the intervening months in hospital, no longer needed the amount of care provided.
One solution is to use agency care while a local service is being established. The creation of larger teams covering more than one PCT area, could result in more flexibility. The Lifetime organisation is an example of using this approach successfully (The Lifetime Service, Child Health Department, Newbridge Hill, Bath BA1 3QE, UK; phone 0122 57731624).
Funding
Funding delays affected 41% of the children in our survey. Before PCTs were established many health authorities divided their budgeting system between hospital and community care, and keeping a child in hospital did not provide the impetus for making quick decisions about funding a community package. Alteration of budgeting systems in the PCTs may hasten agreement for funding.
In our experience, no-one has been refused funding. However, we note refusal to fund an adequate home ventilation package for a child in Northern Ireland was referred for judicial review at the request of parents quoting Articles 2, 3, and 8 of the European Convention on Human Rights. The case did not receive a hearing as the Department of Health agreed to fund after the judge granted leave.
Housing
Thirty three per cent of families were in unsuitable housing. If families lived in local authority provided housing, transfer applications took many months to complete, during which time no discharge planning could be undertaken. Examples from our survey were one child who stayed in hospital until ventilation was no longer needed, and another who died while the family were awaiting transfer.
The very restricted stock of council housing, and the fact that newly built homes have smaller, open plan rooms, and gardens with limited space for extensions, increases the housing issues for these children. Some families are trapped by the stringent financial assessment for the Disabled Facility Grant for an extension, leaving them ineligible for a grant but unable to afford the extension either. A solution suggested by groups representing disabled children is to change the regulations so that the child’s income is assessed rather than the parents’. Few families are fortunate enough to have the support of local fund raising groups, as in the case of one child, who had an extension built following a television appeal.
Family issues
The care of a child with complex needs requires more than normal parenting skills. In spite of this only two of the children in our survey were placed in alternative care. The mother of one child was young and single, and the child was placed in foster care but retains contact with the birth family. In the case of another child home circumstances changed and the family decided to release the child for adoption. Only one child has remained in hospital in the long term. The mother cares for her in hospital on a daily basis, but because of the child’s needs and family circumstances she has not been transferred home.
IS IT ALL WORTH IT?
Fraser found that children who were ventilated due to pulmonary failure had the best prognosis, and children ventilated with central nervous system failure had the worst overall prognosis.1 Based on our experience and on the available literature, children ventilated because of respiratory failure secondary to CLD of prematurity or with an upper airway abnormality have the best outlook in terms of coming off ventilation in the short to long term. Economic factors have not been discussed here or previously published elsewhere, but in our opinion LTV at home can only be seen as a cost reduction in terms of ICU and hospital beds, as a price gain cannot be applied to the improved quality of life for the child. Noyes has written extensively on the parents’ and young people’s perspectives of the discharge planning process itself, and how the children and their carers view their lives when they are long term ventilated.13–15 Noyes found that once medically stable, the children and young people did not want to stay in hospital. They experienced a variety of problems including accessing services, and their needs for attachment, security, communication, friendship, and belonging were not met when hospitalised. There is little information regarding parents’ experiences. Noyes references several newspaper articles in which parents have demonstrated their growing frustration at the inability of professionals to discharge their children from hospital.13 Our experience and feedback from the families involved in this survey suggests that overcoming the hurdles to discharge and expediting the journey towards life at home is justified and worthwhile.
Key points
-
Almost 40% of children discharged home on tracheostomy dependent ventilation can be successfully weaned and decannulated
-
Children on ventilation due to CLD and/or an upper airway abnormality have the best outlook
-
The obstacles to hospital discharge of ventilator dependent children have not changed in half a decade
-
Using trained health care assistants from agencies, and the use of larger teams covering more than one PCT may help overcome some of the obstacles to discharge
One would expect that ethical considerations would be central in any decision regarding the introduction of long term ventilation. The use of valuable resources and the rights of the individual all deserve debate. However, when reviewing our cohort of children, it was interesting to note that there was rarely an ethical dilemma. In only 12 children was there discussion about the appropriateness of continued support. Of this group, only two eventually had a poor outcome. The decision to treat and begin ventilation (often an acute intervention initially) is often made well before any consideration of long term ventilatory needs. Instead, paediatricians face a task of a child already dependent on complex and expensive care. Focus is on rehabilitation and the child’s needs rather than questioning: “How did we get here and should we have started?”
Returning the child to the home environment does not signal the end to paediatric care and responsibility. Regular review and adjustment is required to adapt to a highly fluid status, incorporating the changing needs of the growing child, changes to family structure and dynamics, and the protean nature of the underlying medical condition. A named coordinator in the community has a responsibility to ensure that these changing needs are anticipated and addressed.
