Article Text

Abstract
Background: The role of nasal continuous positive airways pressure (nCPAP) in the management of respiratory distress syndrome in preterm infants is not completely defined.
Objective: To evaluate the benefits and risks of prophylactic nCPAP in infants of 28–31 weeks gestation.
Design: Multicentre randomised controlled clinical trial.
Setting: Seventeen Italian neonatal intensive care units.
Patients: A total of 230 newborns of 28–31 weeks gestation, not intubated in the delivery room and without major malformations, were randomly assigned to prophylactic or rescue nCPAP.
Interventions: Prophylactic nCPAP was started within 30 minutes of birth, irrespective of oxygen requirement and clinical status. Rescue nCPAP was started when Fio2 requirement was > 0.4, for more than 30 minutes, to maintain transcutaneous oxygen saturation between 93% and 96%. Exogenous surfactant was given when Fio2 requirement was > 0.4 in nCPAP in the presence of radiological signs of respiratory distress syndrome.
Main outcome measures: Primary end point: need for exogenous surfactant. Secondary end points: need for mechanical ventilation and incidence of air leaks.
Results: Surfactant was needed by 22.6% in the prophylaxis group and 21.7% in the rescue group. Mechanical ventilation was required by 12.2% in both the prophylaxis and rescue group. The incidence of air leaks was 2.6% in both groups. More than 80% of both groups had received prenatal steroids.
Conclusions: In newborns of 28–31 weeks gestation, there is no greater benefit in giving prophylactic nCPAP than in starting nCPAP when the oxygen requirement increases to a Fio2 > 0.4.
- CPAP, continuous positive airways pressure
- Fio2, fraction of inspired oxygen
- MV, mechanical ventilation
- nCPAP, nasal continuous positive airways pressure
- RDS, respiratory distress syndrome
- Spo2, transcutaneous oxygen saturation
- nasal continuous positive airways pressure
- prophylaxis
- surfactant
- respiratory distress syndrome
- preterm newborn
Statistics from Altmetric.com
- CPAP, continuous positive airways pressure
- Fio2, fraction of inspired oxygen
- MV, mechanical ventilation
- nCPAP, nasal continuous positive airways pressure
- RDS, respiratory distress syndrome
- Spo2, transcutaneous oxygen saturation
- nasal continuous positive airways pressure
- prophylaxis
- surfactant
- respiratory distress syndrome
- preterm newborn
Continuous positive airways pressure (CPAP) has been used to treat neonatal respiratory distress syndrome (RDS) since 1971, initially through an endotracheal tube1 and subsequently through different kinds of nasal prongs.2,3 Many studies have contributed to establishing the role of nasal CPAP (nCPAP) in different groups of infants.4–7 In addition, several devices and modes of delivering CPAP have been compared.8–10 Recent evidence suggests that variable flow nCPAP may be the optimal technique in preterm infants.11,12
Most evidence for the beneficial effects of nCPAP was collected before the introduction of surfactant treatment, and little is known about the interaction between prophylactic or therapeutic nCPAP and prophylactic or therapeutic exogenous surfactant administration. Notwithstanding the extensive experience acquired in the use of nCPAP in the newborn, a systematic review conducted in 1998 concluded that information on the possible advantages of prophylactic nCPAP in preterm infants is insufficient to make definite recommendations for clinical practice.13
The aim of this study was to compare prophylactic with rescue nCPAP in preterm infants of 28–31 weeks gestation to evaluate whether nCPAP applied before clinical evidence of respiratory distress reduces the need for surfactant by improving lung volume and conserving surfactant on the alveolar surface.14
PATIENTS AND METHODS
Trial design
A randomised controlled clinical trial was conducted in 17 Italian neonatal intensive care units from November 1999 to December 2000. The primary end point was the need for exogenous surfactant; the secondary end points were the need for mechanical ventilation (MV) within seven days of birth and the incidence of air leaks. The study was approved by the hospital ethics committees, and parental consent was obtained before randomisation. Infants were eligible if they were inborn and their postmenstrual gestational age was 28–31 weeks (more than 27 weeks and 6 days and not more than 31 weeks and 6 days). The gestational age estimated by fetal ultrasonography during the first trimester of pregnancy was used when there was a discrepancy of more than two weeks with respect to the postmenstrual age. Exclusion criteria were the need for intubation in the delivery room and the presence of major malformations. In the case of twins, only the first twin was randomised for the study. Newborns were intubated in the delivery room according to the criteria of the International Liaison Committee on Resuscitation.15
Randomisation was conducted through the central randomisation unit of the Institute of Neonatology of Bologna, by means of a telephone call. The group assignment was based on a list of casual numbers generated by a computer. Stratification for each week of gestational age was used. Randomised blocks of six were used to ensure treatment balance between the two arms. Eligible patients were entered in the trial based on a 1:1 treatment allocation to prophylactic (prophylaxis group) or rescue (rescue group) nCPAP.
Treatment
The prophylaxis group received nCPAP as soon as possible after birth (within 30 minutes) irrespective of clinical status and oxygen requirement. The rescue group received nCPAP when the fraction of inspired oxygen (Fio2) in the hood was > 0.4, for more than 30 minutes, to maintain transcutaneous oxygen saturation (Spo2) at the right hand between 93% and 96%. nCPAP was given through nasal prongs using the Infant Flow Driver system (EME Ltd, Brighton, Sussex, UK) at a level of 4–6 cm H2O. Newborns receiving nCPAP at a pressure of 6 cm H2O, requiring a Fio2 > 0.4 for more than 30 minutes to maintain Spo2 in the range 93–96%, and showing radiological signs of RDS16 were endotracheally intubated after a bolus of fentanyl (0.5–2 μg/kg over five minutes),17 treated with surfactant (Curosurf–Chiesi Farmaceutici, Parma, Italy; 200 mg/kg), and manually ventilated for two to five minutes. The infants were then extubated and placed in nCPAP if they had a good respiratory drive and a satisfactory Spo2 value. An arterial blood sample for blood gases was taken before surfactant treatment in all cases. Criteria for MV were the following: persistence of a Fio2 requirement > 0.4 on nCPAP to maintain a Spo2 of 93–96% after surfactant administration; at every point of the study, severe apnoea (defined as more than four episodes of apnoea/hour or more than two episodes of apnoea/hour if ventilation with bag and mask was required); Paco2 > 70 mmHg and pH < 7.2; Fio2 rapidly increasing above 0.8 even before 30 minutes. Peripheral perfusion and blood pressure were monitored non-invasively in all infants, and inotropic amines and/or volume expansion were given if indicated.
Echocardiography was performed in all infants at 24–72 hours of life, and intravenous treatment with ibuprofen (10 mg/kg followed by two doses of 5 mg/kg, 24 hours apart)18 was initiated if a patent ductus arteriosus with a left to right shunt was found. All infants not mechanically ventilated were treated with caffeine (loading dose 10 mg/kg, followed after 24 hours by a maintenance dose of 2.5 mg/kg/24 hours, intravenously). Cerebral echography was performed within the first 48 hours of life, repeated at 7 days, and then every two weeks until discharge. Intracranial haemorrhages were classified as described by Volpe,19 and periventricular leucomalacia as described by De Vries et al.20
Chronic lung disease was defined as oxygen dependency at 36 weeks postmenstrual age.
Statistical analysis
To estimate the possible number of eligible infants per year in all the participating neonatal intensive care units and the requirement for surfactant replacement therapy and MV, a questionnaire was sent to all neonatal intensive care units. During the year before the trial, the requirement for surfactant therapy and MV in newborns of 28–31 weeks gestation was 47% (range 25–79%) and 42% (range18–66%) respectively. To detect a 40% difference in the requirement for surfactant treatment (from 47% to 28%), with a power of 80% and an α error of 5% (two tailed test), 111 infants were required for each arm. The number of eligible newborns per year in all the 17 centres was about double that. Therefore, taking into consideration denials of consent by the parents, the duration of the study was established as one year.
χ2 statistics were used to test differences between the two study groups. Logistic regression analysis (backward elimination, likelihood ratio test) was performed to account for confounding factors and to identify the impact of individual factors, such as gestational age, prenatal steroid treatment, sex, premature prolonged rupture of membranes together with study group allocation, on the need for surfactant and MV.
Data forms were sent to the coordinating centre, reviewed for completeness, and entered into a database. Data were analysed using the SPSS version 5.0 software (SPSS Inc, Chicago, Illinois, USA).
The total number of newborns of 28–31 weeks gestation, as well as the number of newborns eligible but not randomised, and the relative outcomes were reported by each participating centre.
RESULTS
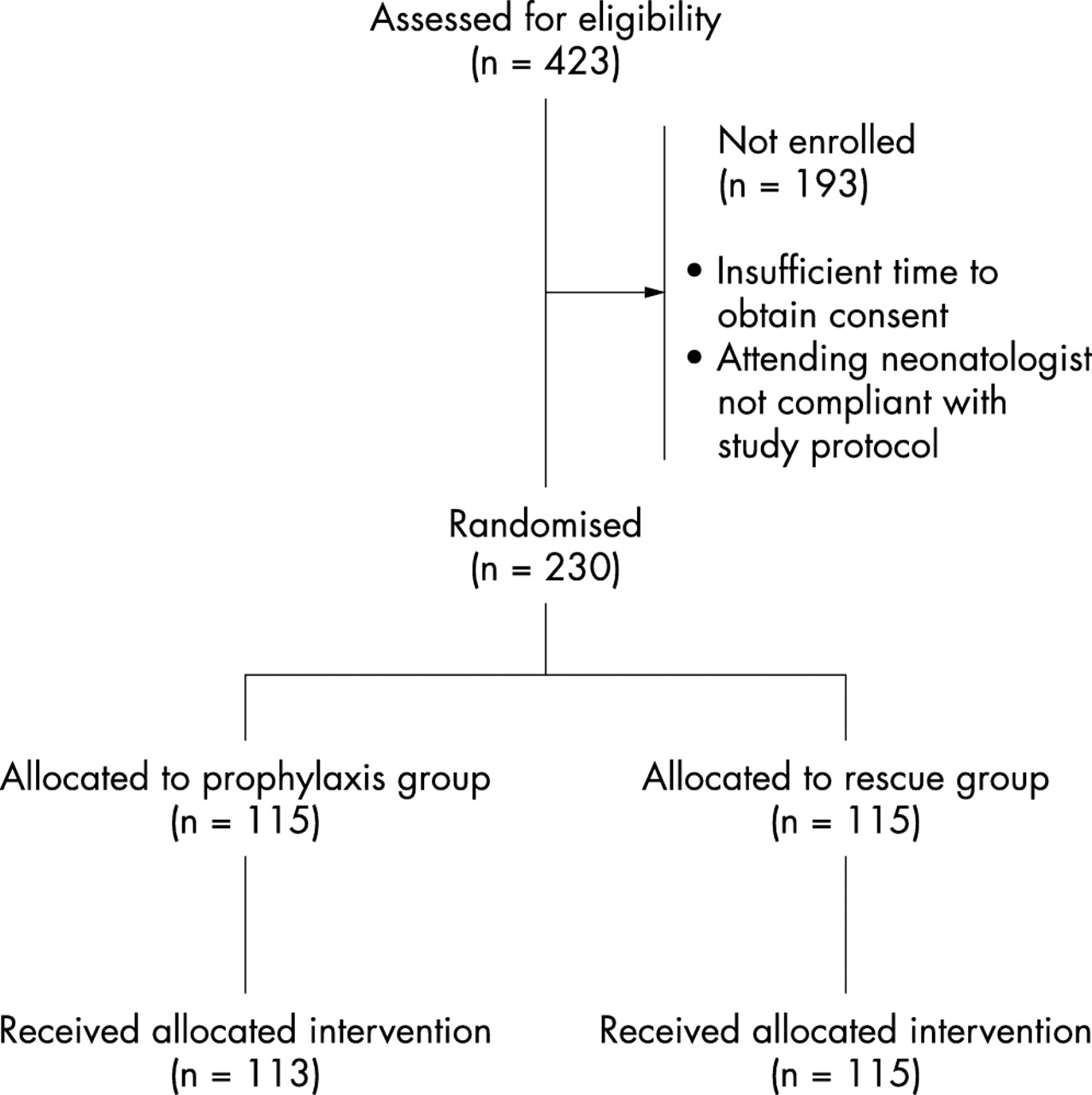
The total number of infants of 28–31 weeks gestation admitted to the participating units during the study period was 527. Of these, 104 were not eligible: 62 were intubated in the delivery room, and 42 were second twins or had major malformations. Of the remaining 423 infants, 193 were not randomised because of insufficient time to obtain parental consent or because the attending neonatologist was not compliant with the study protocol. The mean (SD) gestational age and birth weight of this group of newborns were 30.0 (0.9) weeks and 1375 (380) g respectively and were not significantly different from the randomised infants.
The incidence of surfactant treatment and MV in the group of eligible but not randomised infants was 26% and 28% respectively. No adverse outcome occurred in 84%; 2% were affected by intraventricular haemorrhage more severe than grade 2, 5% by periventricular leucomalacia, and 2% died within 28 days of age.
Statistical analysis was performed on the data collected in 230 infants admitted to the participating neonatal intensive care units by the end of December 2000 (115 in the prophylaxis group and 115 in the rescue group). Only two patients did not follow the protocol; they were included in the originally assigned group, and an intention to treat analysis was performed (fig 1).

{kind=link}
Flow diagram of eligible newborns. The number of infants not randomised and the reasons for non-enrolment are provided. Two infants in the prophylaxis group did not receive the allocated treatment (both infants requiring surfactant were firstly mechanically ventilated and then given surfactant). Statistical analysis was by “intention to treat”.
The two groups were comparable for gestational age, birth weight, sex ratio, clinical risk index for babies (CRIB) score21,22, and administration of prenatal steroids (table 1).
Fetal and neonatal data of the two groups of newborns randomised to receive either prophylactic or rescue nasal continuous positive airway pressure (nCPAP), and of the group of eligible, but non-randomised infants
The need for surfactant was 22.6% (26/115) in the prophylaxis group and 21.7% (25/115) in the rescue group (p > 0.05); the need for MV was 12.2% (14/115) in the prophylaxis group and 12.2% (14/115) in the rescue group (p > 0.05). The severity of RDS, graded radiologically, was similar in the two groups. The mean (SD) arterial to alveolar oxygen tension ratio (a/A) calculated before the instillation of surfactant was 0.20 (0.07) in the prophylaxis group and 0.19 (0.08) in the rescue group. The incidence of air leaks was 2.6% in both groups.
Table 2 gives the incidence of adverse outcomes; there were no significant differences between the two groups.
Incidence of adverse outcomes in the two groups of newborns receiving prophylactic or rescue nasal continuous positive airway pressure
Logistic regression analysis showed that the need for surfactant and MV in the whole group of infants was positively associated with the male sex. In fact, the need for surfactant was 34/118 in male infants and 17/112 in female infants (relative risk 1.9; 95% confidence interval 1.13 to 3.20). The incidence of MV was 21/118 in male infants and 7/112 in female infants (relative risk 2.85, 95% confidence interval 1.26 to 6.44). Moreover, logistic regression analysis showed that there was a trend towards a greater need for surfactant in infants who had not received prenatal steroids (p = 0.0606).
Sixty six newborns required nCPAP in the rescue group (57.4%); in all cases nCPAP was begun more than 30 minutes after birth, at a median age of 108.5 minutes (range 40–3600). The logistic regression analysis showed that, in a model considering the effects of gestational age, sex, and prenatal steroid treatment on the need for nCPAP in the rescue group, only the prenatal steroid treatment reached significance (p = 0.02).
DISCUSSION
In the last decade, efforts have been made to improve survival and long term outcome of preterm newborns. Prenatal steroid administration has reduced the incidence and severity of RDS.23 Early identification and treatment of patent ductus arteriosus has reduced lung deterioration from haemodynamic factors.18 Studies on surfactant therapy have helped to establish the best type of surfactant and the optimum timing of its administration.5,24–28 The result is a large population of less severely affected preterm infants who can be treated without MV, thus reducing iatrogenic risks and costs. Several studies6,7,29 have suggested that using nCPAP as the first intervention in the management of the less severe cases of RDS and restricting MV to the more severe cases may be beneficial in reducing the need for MV and the incidence of chronic lung disease. Recently, a multicentre randomised controlled trial showed that early versus late treatment with surfactant may reduce even more the necessity for MV in infants of gestational age < 30 weeks treated by nCPAP.30 Unfortunately, there are no randomised trials indicating the best time for beginning nCPAP. The study of Han et al,31 which showed no differences in the incidence of RDS in preterm infants of < 33 weeks gestation receiving early or rescue nCPAP, was conducted before the introduction of surfactant treatment and antenatal steroids. Moreover, the authors did not report the exact time that nCPAP was started in the two groups.
Our study shows that, in preterm infants of 28–31 weeks gestation, prophylactic nCPAP does not reduce the need for later surfactant administration or for MV in the first week of life, when compared with nCPAP given at a Fio2 > 0.4. The relative stiffness of the rib cage probably enables these not extremely immature infants to reach and maintain functional residual capacity. This prevents alveolar collapse and surfactant consumption even without the application of positive pressure.
The criteria for treatment in this study were based on Spo2 values. Pulse oximetry has been shown to be reliable in detecting hyperoxic and hypoxic episodes in neonates, although to achieve good sensitivity, a low specificity must be accepted.32,33 When pulse oximeters are used, attention must be paid to placing the probe correctly and to having a pulse pressure of more than 20 mm Hg.32 These limitations in the correct interpretation of the Spo2 values have been overcome by experience and by the careful detection and treatment of hypotension and poor peripheral perfusion. In our study, the widespread use of pulse oximetry in clinical practice has resulted in high compliance with the study protocol by the participating centres. Furthermore, the results of the study are easily reproducible and applicable in the clinical setting.
The results of this study appear to be in contrast with those from other studies7,29 suggesting a beneficial role for prophylactic nCPAP. There are three possible explanations for this difference. Firstly, the use of historical controls in the other studies creates several problems in interpretation. Changes in practice over time in the obstetric and neonatology fields may account for many differences in outcome, antenatal steroid administration and the different criteria for intubation and MV being the main confounding factors. Secondly, the other studies reported data on newborns weighing less than 1500 g, and thus included all the premature infants. We chose not to include newborns of < 28 weeks gestation because in many centres they are electively treated with early prophylactic surfactant shortly after birth. Thirdly, “prophylactic” nCPAP was not defined exactly in the previous studies; this term encompasses a wide range of intervals after birth and it is impossible to distinguish between really prophylactic and early rescue nCPAP. We chose to define as prophylactic nCPAP applied within 30 minutes of birth. This enabled all the centres to comply with the study protocol and begin nCPAP at a mean age of 19 minutes.
The standardisation of intervention produced by the trial protocol reduced the need for surfactant and MV in infants of 28–31 weeks gestation, compared with the pre-trial survey. Also in the group of eligible but non-randomised infants, the need for exogenous surfactant and MV was higher than in the study groups. In fact, in all but two centres, management of RDS before participation in the study was quite inhomogeneous and dissimilar from the study protocol: nCPAP was not necessarily tried before MV in the treatment of RDS; exogenous surfactant was given at a more advanced stage of RDS and was invariably followed by MV. Two studies30,34 have suggested that many preterm infants, if not apnoeic, can be extubated in nCPAP soon after the instillation of surfactant, thus avoiding MV and the associated risks. This strategy was also applied in our trial. In fact, in our study nearly 50% of the babies treated with surfactant did not need MV at all. Furthermore, by starting nCPAP when the Fio2 requirement was greater than 0.4, we could avoid any ventilatory support in 43% of infants assigned to the rescue group.
Our data suggest a higher need for respiratory assistance in male infants. The evidence of a worse prognosis in boys has been widely reported in the literature; the physiopathological basis of this difference remains to be clarified35 and is not the topic of the present study.
In conclusion, our trial shows that nCPAP prophylaxis is no better than nCPAP rescue treatment in newborns of 28–31 weeks gestation. Therefore unnecessary intervention can be avoided in a group of preterm infants who make up a large proportion of those admitted to neonatal intensive care units. Moreover, the evidence of a lower requirement for surfactant and MV in randomised compared with non-randomised infants suggests that starting nCPAP when the Fio2 requirement is over 0.4 and giving exogenous surfactant when the Fio2 is over 0.4 in nCPAP in the presence of RDS may be a sound approach in treating RDS in infants of 28–31 weeks gestation, permitting prompt extubation in many cases.
The results of this trial may not be universally applicable to all infants of this gestational age, as nearly 80% of our study population had received a complete course of prenatal steroids and all of them were inborn. This may not be the case in other contexts.
APPENDIX
The multicentre study group included the following investigators who collected data and provided care for study patients:
Elena Brasca, Department of Neonatology, Clinica Mangiagalli, ICP, Milano, Italy;
Tiziana Fedeli, Division of Neonatology, San Gerardo Hospital, Monza, Italy;
Michele Pelti, Rossella Germani, Claudia Costato, Division of Neonatology, G Salvini Hospital, Rho, Italy;
Gianfranco Maffei, Giuseppe Rinaldi, Division of Neonatology, Ospedali Riuniti, Foggia, Italy;
Maria Pia Morgando, Palma Cambursano, Division of Neonatology, Bianchi Melacrino Morelli Hospital, Reggio Calabria, Italy;
Fabio Strano, Giorgio Rondini, Division of Neonatology, Policlinico S Matteo, Pavia, Italy;
Pierantonio Santuz, Paolo Biban, Neonatal and Pediatric ICU, Civile Maggiore, Borgo Trento Hospital, Verona, Italy;
Eloisa Gitto, Stefania Paola Cordaro, Ignazio Barberi, Division of Neonatology, University of Messina, Messina, Italy;
Giancarlo Gargano, Maria Federica Roversi, Fabrizio Ferrari, Department of Neonatal Medicine, University of Modena, Modena, Italy;
Gilberto Compagnoni, Gianluca Lista, Francesca Castoldi, Department of Neonatology, V Buzzi Hospital, ICP, Milano, Italy;
Lucio Giordano, Francesco Messina, Marcello Napolitano, Neonatal Intensive Care Unit, Villa Betania Hospital, Napoli, Italy;
Antonio Marra, Maria Pia Morgando, Division of Neonatology, S Croce Hospital, Moncalieri, Italy;
Carlo Dani, Firmino F Rubaltelli, Division of Neonatology,Careggi University Hospital, Firenze, Italy;
Wanda Bonacci, Giovanni Serra, Neonatal Intensive Care Unit, G Gaslini Institute, Genova, Italy;
Giancarlo Piccinini, Gianfranco Santini, Division of Neonatology, S Maria delle Croci Hospital, Ravenna, Italy;
Claudio Martano, Claudio Fabris, Institute of Neonatology, University of Torino, Torino, Italy.