





Abstract
Plethysmographic specific airway resistance (sRaw) is a useful research method for discriminating lung disease in young children. Its use in clinical management has, however, been limited by lack of consensus regarding equipment, methodology and reference data.
The aim of our study was to collate reference data from healthy children (3–10 yrs), document methodological differences, explore the impact of these differences and construct reference equations from the collated dataset.
Centres were approached to contribute sRaw data as part of the Asthma UK initiative. A random selection of pressure–flow plots were assessed for quality and site visits elucidated data collection and analysis protocols.
Five centres contributed 2,872 measurements. Marked variation in methodology and analysis excluded two centres. sRaw over-read sheets were developed for quality control. Reference equations and recommendations for recording and reporting both specific effective and total airway resistance (sReff and sRtot, respectively) were developed for White European children from 1,908 measurements made under similar conditions.
Reference sRaw data collected from a single centre may be misleading, as methodological differences exist between centres. These preliminary reference equations can only be applied under similar measurement conditions. Given the potential clinical usefulness of sRaw, particularly with respect to sReff, methodological guidelines need to be established and used in prospective data collection.
Lung function techniques that can be applied during tidal breathing are particularly pertinent in young children where active cooperation and understanding may be limited 1. Plethysmographic specific airways resistance (sRaw) can be measured during tidal breathing from the relationship between simultaneous measurements of airflow and change of plethysmographic pressure without need for any special breathing manoeuvres against an airway occlusion 2 and is therefore ideally suited for young children 3–6. sRaw is the product of functional residual capacity (FRC) and airways resistance. Since airways resistance has a strong inverse relationship to lung volume 2, theoretically sRaw should provide a relatively stable index with which to distinguish effects of disease from those of growth and development. There is, however, some evidence to suggest age and/or sex differences in young children 7, 8. This technique has proved to be a feasible and useful outcome measure in clinical research studies of preschool children with cystic fibrosis and wheezing disorders 9–15.
Despite these advantages, the use of sRaw as a valid outcome measure in clinical management has been limited by the lack of consensus with regards to equipment, measurement conditions, data collection, analytical strategies and reference data. Many users have therefore developed their own in-house techniques for data collection, analysis and quality control. Consequently, reported values of sRaw have been collected under a variety of differing measurement conditions involving the following: including modified masks 15 or mouthpieces 16; using bacterial filters or not; and different breathing patterns and frequencies.
Results are further influenced by: 1) the extent to which operator quality control is used, either to exclude pressure–flow (P/F) loops due to poor phasing/irregular breathing patterns, or to manually adjust the automatically generated tangents for such loops; 2) the number of breaths per epoch or trial and the number of trials used to summarise data; 3) whether results are expressed as the median of all data 11 or the weighted mean of data selected after extensive quality control 12; and 4) which outcomes are used, i.e. effective resistance (sReff), total resistance (sRtot), peak resistance (sRpeak), or that calculated over a fixed range of flow (e.g. 0–0.5 L·s−1, i.e. sR0.5).
In children, the most common reported outcomes are sReff and sRtot; sR0.5 has been discouraged in children due to potential age-related effects 17. sRtot is a simple outcome measured between points of maximum plethysmographic (box) pressure, whereas sReff is calculated from multiple points throughout the breathing cycle (the integration method, see online supplementary material for details) and may thus be a better reflection of airway mechanics 7, 18.
Interpretation of sRaw is further complicated because commercially available plethysmographs now apply a digital (electronic) thermal correction factor during calculation of sRaw 19, whereas default reference equations are commonly based on data collected using the re-breathing or panting technique to achieve body temperature, pressure and water vapour-saturated (BTPS) conditions 20. Since the latter are known to be systematically lower than those collected under electronic conditions 5, even healthy subjects will appear to have abnormally elevated sRaw if results are interpreted using BTPS-derived reference data.
The Asthma UK Collaborative Initiative was established to collate available reference data from healthy young children to produce reference centiles for spirometry 21, respiratory resistance from the interrupter technique and plethysmographic sRaw 22. This study aimed to: 1) collate available reference data for sRaw and document any differences between the collaborating centres; 2) explore the impact of these differences; and 3) construct reference equations from the collated dataset.
MATERIALS AND METHODS
Study subjects
The collaborative group was initially comprised of members of the American Thoracic Society/European Respiratory Society paediatric pulmonary function test task force. Subsequently, collaborators were identified by systematically searching PubMed, advertising at international conferences, through membership bulletins, word of mouth and by hand searching relevant respiratory periodicals.
Study design
sRaw data were collected in healthy children aged 2–11 yrs, together with details regarding population characteristics, equipment, measurement protocols and quality control. All data were collected using the same plethysmographic body box (Jaeger GmbH, Wurzburg, Germany) though different software versions were used. Where possible, visits were made to collaborating centres to conduct inter-laboratory comparisons and obtain random samples of original P/F curves. All data were anonymised prior to contribution and came from research studies where full local ethics approval and informed parental consent had been obtained. We determined differences in sRaw of 0.2 kPa·s−1 between-centres or 0.1 kPa·s−1 within-subject as being clinically or physiologically significant, such differences approximating one standard deviation for between- and within-subject variability, respectively 3.
Methods
Where differences in methodology between-centres were observed, subanalyses were conducted to establish the impact of these differences (details of these subanalyses and results can be found in the online supplementary material).
Quality control
A random sample of 10–20 P/F curves from children studied at each centre was requested to enable a central quality control (QC) over-read; P/F curves were graded out of 6, with one point given for each of the following criteria achieved: 1) respiratory rate 30–45 breaths·min−1; 2) breaths superimposable (i.e. parallel tangents); 3) breaths similar in size and shape; 4) breaths reasonably closed at zero flow; 5) no obvious distortions (e.g. glottic closure, cough, talking); and 6) availability of at least two acceptable trials
The over-read sheet and instructions can be found on the online supplementary material and at 22.
sRaw outcomes
The potential impact of reporting different outcome measures for sRaw was investigated by reanalysing a subset of data and making within-subject comparisons between sRtot and sReff.
Reporting results
Data with three sets of 10 breaths (or five sets of five breaths, depending on software version) were examined and results from each reported as: 1) the weighted mean, i.e. the sum of all acceptable sRtot values, after rigorous QC, divided by the total number of acceptable values 12; exclusion of technically unacceptable data was based on the QC criteria 1–5 as detailed above; 2) the mean of the median sRtot from three trials, prior to any exclusions; or 3) the median, as represented by the median value of sRtot from the most representative (i.e. median) trial.
Analysis
Statistical analyses were performed using SPSS version 16 (SPSS, Inc., Chicago, IL, USA) and GraphPad Prism 5 software (GraphPad, San Diego, CA, USA). One-way ANOVA and independent t-tests were applied to assess between-centre differences. Paired t-tests and Bland and Altman plots were used to assess within-subject agreement between different outcomes (sReff and sRtot, and within the same subject over time). Where appropriate, linear regression analyses were used to assess the relationship between different sRaw outcome measures to determine correction factors. Reference equations were developed using the LMS method 23, details of which can be found in the online supplementary material.
RESULTS
Five centres contributed 2,872 sets of sRaw data from 2,347 children measured between 1995 and 2008. All centres had used a Jaeger plethysmograph, but five different software versions were used ranging from 4.01 to 5.01 (table 1). Individual sRaw values ranged 0.21–2.82 kPa·s−1, with the mean±sd sRaw from these centres ranging from 0.55±0.18 to 1.29±0.30 kPa·s−1. Significant differences were observed between centres (one-way ANOVA: p<0.0001) (fig. 1).

Specific airways resistance (sRaw) results by centre. The difference between the highest reported sRaw (centre 2) and the lowest sRaw (centre 1) was 0.74 kPa·s−1. Centre 1: n = 38; 2: n = 40; 3: n = 828; 4: n = 472; and 5: n = 1,000.
White subjects of European descent contributed 2,531 (88%) of the data points; 93 data points (3%) were recorded as non-white, whereas ethnicity was not recorded in 248 (9%) subjects. The limited data in non-white subjects precluded analysis according to ethnic origin, hence these subjects were excluded from the reference equations. Further details regarding population characteristics, equipment and methodology are summarised in table 1.
Equipment
Three centres used a mouthpiece and nose clip for data collection while the remaining two used a modified facemask.
Quality control
All centres supplied details regarding methodology and analysis, and a random sample of original P/F curves for over-reading; however, the print-outs from one centre were too small to over-read and another centre only provided a single screen-shot of recent data. Examination of the protocols revealed two centres (1 and 3) had performed “manual adjustment of the tangent” whereas the others accepted the computer generated slopes. sRaw was significantly lower when manual adjustment was used (fig. 1) and results from these centres (n = 866) were excluded from further analysis. The three remaining centres scored five out of six, three out of six and five out of six on over-read (see online supplementary material for details). All subsequent results are based on the three remaining centres.
sRaw outcomes
In the two centres that reported both sReff and sRtot, the outcomes were highly correlated (fig. 2a), but sReff was systematically lower (fig. 2b). We used the data from centre 4 to generate a correction factor which was validated with data from centre one (data not shown), we then applied this correction factor to calculate sReff and sRtot in all centres to allow direct comparisons (table 2). Values of sReff and sRtot were similar between the centres, as was the between-subject variability.

Based on 228 paired measurements, total airways resistance (sRtot) and effective airways resistance (sReff) were found to be highly correlated (r2 = 0.98; a); however, sRtot was significantly and systematically higher than sReff (mean difference (95% CI): 0.16 (0.15–0.17) kPa·s−1; b). sRaw: specific airways resistance.
Mean versus median
Within-subject comparisons revealed no statistical differences between weighted-mean versus mean-of-median sRtot (mean difference: 0.003 (95% CI -0.001–0.006) kPa·s−1; n = 297) or between mean-of-median and median-median sRtot data sets (mean difference: -0.02 (95% CI -1.90–0.15) kPa·s−1; n = 101).
Repeated measurements
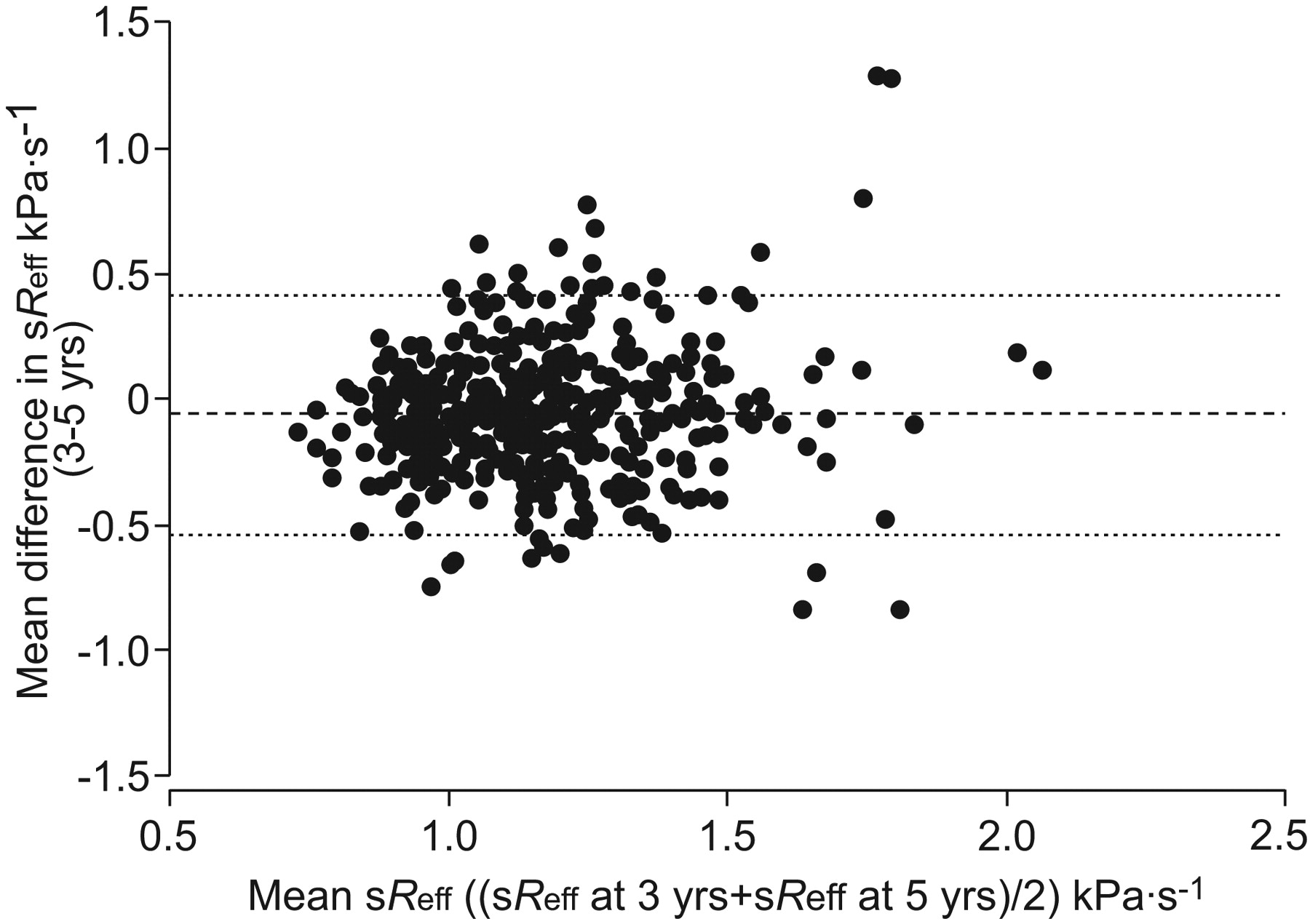
525 repeated measurements at 3 and 5 yrs of age were available from one centre. A very small, albeit statistically significant within-subject reduction in sReff occurred over this period: mean difference (95% CI) in sReff: -0.06 (-0.08– -0.04) kPa·s−1 (p<0.0001), suggesting minimal age-related changes (fig. 3).

Paired measurements of effective airways resistance (sReff) at 3 and 5 yrs of age. Mean difference (-----) (95% CI): -0.06 (-0.08–0.04) kPa·s−1; 95% limits of agreement (······): -0.54–0.41.
Age effects
After adjustment for centre, sex and age were independently associated with sRaw; sReff decreased with age (β: -0.044, p<0.0001), and was slightly lower in females (β: -0.030, p<0.0001). Centre explained the most variability (partial r2 = 11%), compared with 6% for sex and 4% for age. After adjustment for centre, sex and age, sReff was independent of height (β: 0.002, p = 0.94)
Within-centre differences
In centre 4, healthy subjects were measured as part of five different projects, one of which was carried out across three different sites. Despite the use of identical protocols and equipment during all projects, there were statistically significant differences in mean sRaw between projects; these differences being of potential clinical/physiological relevance in two projects (1b and 4)(table 3).
Reference equations
LMS reference equations were developed from the 1,908 included measurements (fig. 4). The reference equations were limited to children aged 3–10 yrs to avoid edge effects. Z-scores can be obtained by substituting the values for M, S and L from table 4 into the following equation: z-score =((measurement/M)L-1)/(L×S).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted values of specific airways resistance with upper and lower limits of normal for a) effective airways resistance (sReff) and b) total airways resistance (sRtot) for children aged 3–10 yrs. ––––––: equations for males; ------ equations for females.
It is important to note that these equations can currently only be applied to White children of European descent aged 3–10 yrs, and only when measurements are made under the following conditions. Equipment should include a Jaeger plethysmograph (≥version 4.01) with a specialised mask or mouthpiece with noseclip, and a filter in situ. No adjustments to the computer generated slope should be made and a breathing frequency of 30–45 breaths·min−1 should be adhered to. More details of recommendations for future data collection, including the use of sReff as the primary outcome measure since this computes pressure and flow signals throughout the breathing cycle, can be found in box 1 of the online supplemetary material.
DISCUSSION
This study comprises the largest collation of paediatric sRaw data from healthy controls to date, enabling a comprehensive review of the different methodologies. Significant differences in methodology between collaborating centres necessitated exclusions of some sRaw data, but enabled the development of a quality-control over-read sheet and preliminary sex-specific reference equations that also adjust for the minimal age-related changes in sReff and sRtot. In addition, we present recommendations to facilitate more standardised data collection and analysis in the future.
Clinical implications
The observed methodological differences have important implications in both clinical management and research studies, and suggest that reference ranges obtained in one laboratory could lead to significant under or over-estimation of lung disease if transferred to another, unless measurements are performed under identical conditions. Thus the reference equations presented are an interim solution to the problem, and can only be applied to populations that have been measured using the same methodology. Nevertheless, these preliminary equations are far more appropriate than those currently available in Jaeger equipment. The “Jaeger-kids” for children aged 4–18 yrs, and “Jaeger” for those aged >18 yrs are based on data collected under BTPS conditions more than 30 yrs ago 20 and have identical predicted values for sReff and sRtot, whereas we found sReff to be significantly lower than sRtot (fig. 2). Furthermore the Jaeger-kids predicted values of both sReff and sRtot of 0.51 kPa·s−1 for females and 0.53 kPa·s−1 for males aged <18 yrs significantly underestimate the actual values observed in healthy children in this study, which were collected using electronic compensation. This would result in serious over-estimation of the degree of airway obstruction in children with lung disease. In addition, whereas we observed a very gradual decline in the predicted values with age (fig. 3), the Jaeger equations suggest that there is a sudden (and physiologically implausible) increase in predicted values to 0.96 kPa·s−1 for females and 1.18 kPa·s−1 for males from 18 yrs of age onwards. Finally, in contrast to the current Jaeger reference equations, and more recent single-centre reference data 3, limits of normality for both males and females in sReff and sRtot with which to identify abnormality more reliably in individual children, are now provided.
Strengths and limitations
The Asthma UK dataset is the largest collection of sRaw data in children; however, all collaborating centres used the Jaeger equipment and we cannot generalise our findings to other equipment. Furthermore the impact of software version could not be examined as several centres had updated software since the time of data collection. Quality control is an essential aspect of any lung function test, and our in-depth examination of each centre-specific protocol enabled us to develop a QC over-read sheet.
We demonstrated that sRaw can be affected by use of a filter in adults if not calibrated and adjusted for in the internal settings (see online supplementary data). While the measured effect was within the expected 0.1 kPa·L−1·s−1 increase in resistance as reported by manufacturers (Air Safety Ltd, Morecambe, UK), this could introduce an important bias to sRaw if an operator neglects to calibrate with a filter in situ, and/or neglects to select the filter check box in the internal settings. These differences may be greater in children because of the relative increase in dead space. Ethically we were unable to evaluate the influence of filter use in children, but since filters should be used to comply with most infection control policies, reference data should be based on measurement conditions that reflect clinical practice. However, when a filter is used it is essential that the plethysmograph is calibrated with a filter in situ, and the internal settings are corrected for the additional resistance imposed by the filter.
It has previously been shown that breathing frequency can have a marked impact on measured values of sRaw 5. In this study 5, collaborating centres adhered to the recommendations of 30–45 breaths·min−1, and we were unable to systematically evaluate the influence of breathing frequency. The true impact of breathing pattern may relate more to flows attained, which can vary markedly while maintaining identical breathing frequency, than to respiratory rate per se. This warrants further investigation into flows attained and breathing frequency in future studies. In the meantime, we would recommend that the child is encouraged to breathe as quietly and naturally as possibly while maintaining breathing frequencies between 30–45 breaths·min−1.
We present reference equations for both sReff and sRtot; however, sReff is likely to be the better outcome as it takes into account resistive changes throughout the breathing cycle rather than simply the tangent between points of maximum pressure (the equation for calculating sReff is included in the online supplementary material) 18. While the difference between sReff and sRtot was relatively small in health (and assumed to be similar across all centres), differences in outcomes may be more marked in the presence of airway disease and it is therefore essential to use a consistent approach and not to attempt to predict one outcome from another in children with lung disease. Whilst, the preliminary reference equations presented within are an improvement on current equations, they must be used with caution since they were created with a correction factor on the assumption that the relationship between sReff and sReff in health across the centres was consistent. They will, however, enable future research and clinical studies to examine which of these outcomes is more appropriate for detecting changes in lung function in young children with respiratory symptoms and disease.
Repeated measurements within the same children are rare but crucial for understanding growth and development of airway function within individuals. The longitudinal data included as part of our current study suggested minimal age-related changes in young children. Nevertheless, the 95% limits of agreement indicated that even in healthy children sRaw may vary by up to 0.5 kPa·s−1 over a 2-yr period, which must be taken into account when interpreting serial results from those with lung disease. It should also be noted that while most studies have concluded that sRaw is relatively consistent in preschool children, we only noted minor age-related changes between 3 and 10 yrs in our study. There are developmental reasons why this may not be the case during infancy 8, 24.
Finally, we observed differences within centres with no apparent explanation. It has recently been suggested that even when using apparently identical equipment and protocols, inter-centre differences in sRaw can result from hidden differences in internal settings within the equipment 25 which are only accessible to equipment engineers. This could have potentially contributed to the within-centre differences observed in the current study. Such differences require thorough investigation by the manufacturers with standardisation of internal settings prior to distribution.
Recommendations
Based on the data collated from five European centres we have agreed upon recommendations (below) that will facilitate further improvements to the sRaw technique, such that future data collection can be combined to develop more robust reference equations. Detailed recommendations are available in box 1 of the online supplementary material.
1) Reporting the median breath from the median trial appears to be the most robust approach as it is not influenced by outliers, and avoids the subjective and time-consuming nature of excluding inadequate loops.
2) While we were unable to directly compare results obtained with a modified mask and mouthpiece, previous studies have found no difference between these methods 4. In order to standardise methodology, we recommended an appropriately sized mouthpiece and noseclip be used since these are now used routinely for many preschool lung function tests 1, as well as in older children and may be more readily available.
3) As software and equipment change, we recommend that laboratories always validate any major software releases by within-subject comparisons in biological controls. Results of such biological validation should be collated by manufacturers and placed in the public domain. Validation studies should be performed under identical conditions as that in clinical practice, i.e. breathing quietly at 30–45 breaths·min−1 with a filter in place.
4) In future studies, we recommend sReff to be the primary outcome measure since this calculates sRaw from multiple points throughout the breathing cycle. sReff can be calculated as follows: where Pamb is the ambient pressure, integral δVdV is equivalent to the area enclosed by the specific work of breathing loop, and integral V'dV is equivalent to the area of the flow/volume loop.
where Pamb is the ambient pressure, integral δVdV is equivalent to the area enclosed by the specific work of breathing loop, and integral V'dV is equivalent to the area of the flow/volume loop.
Conclusions
Significant methodological differences between centres that perform sRaw measurements have important implications for clinical interpretation of results. Given the potential clinical usefulness of sRaw, there is an urgent need to apply standardised methodology, and to prospectively collect data in healthy children of all ages and ethnicities in order to develop more robust reference equations for children.
Acknowledgments
The authors would like to thank the children and families who participated in the original studies, and the investigators involved in the original data collection: London, UK: C. Saunders, A. Laverty, C. Oliver, K. Lindsay and C. Guinard; Leicester, UK: T. Clarke, H. Clarkson and A. Leary; Manchester, UK: L. Lowe; and Glasgow, UK: C. King.
Footnotes
This article has supplementary material accessible from www.erj.ersjournals.com
Support Statement
This study was funded by Asthma UK, the UK Medical Research Council and the Wellcome Trust.
Statement of Interest
None declared.
- Received August 27, 2009.
- Accepted January 25, 2010.
- ©2010 ERS
REFERENCES










