Article Text

Abstract
Background: Gastro-oesophageal reflux (GOR) is increased in cystic fibrosis (CF), but its prevalence, characteristics, association with gastric aspiration and respiratory impact are not well characterised. We investigated acid and weakly acidic reflux, aspiration and respiratory symptoms/function in adult CF patients.
Methods: Thirty-three CF patients [19 men; 29 (18–55) years, [10 post-lung transplant (LTx)] underwent impedance–pH monitoring for detection of acid (pH<4) and weakly acid GOR (pH 4–7). In 16 patients cough was objectively recorded with oesophageal manometry, and the symptom association probability (SAP) was calculated. Saliva and bronchoalveolar lavage fluid (BALF) were tested for bile acids.
Results: Twenty-eight patients had increased GOR (21 acid, 5 weakly acidic and 2 acid+weakly acidic) and 10 had a positive SAP for reflux cough. GOR parameters were similar in non-LTx and post-LTx CF patients. The sequence reflux cough was significantly more common than cough reflux. Sixteen of 38 patients had bile acids in saliva and 6/10 in BALF and this was almost exclusively observed in patients with genotype DF508/DF508. Only 12/28 with increased GOR and 9/22 with bile acids in saliva/BALF had typical reflux symptoms. There was a positive correlation (r = 0.53, p = 0.03) between oesophageal acid exposure and cough. SAP-positive patients with for reflux cough had a lower lung function than SAP-negative patients.
Conclusion: Increased GOR is prevalent in CF and not secondary to cough. Acid GOR is common, but weakly acidic GOR may also occur. CF patients have a high risk of aspiration and reflux seems to be associated with more cough and poorer lung function. Outcome studies with intense anti-reflux therapy are needed to confirm the deleterious role of reflux in CF progression.
Statistics from Altmetric.com
Increased acid gastro-oesophageal reflux (GOR) was first reported in patients with cystic fibrosis (CF) in 1975. The prevalence of increased acid GOR in CF is currently estimated to be between 35 and 81%.1–4 Several primary mechanisms for increased GOR in CF have been proposed including a reduced pressure of the lower oesophageal sphincter (LOS),2 increased number of transient LOS relaxations5 and delayed gastric emptying.6 However, it is frequently suggested that increased GOR in CF might be a secondary phenomenon resulting from increased abdominal–thoracic pressure gradient during cough and/or physiotherapy.2
So far, gastro-oesophageal reflux in patients with CF has been assessed with 24 h oesophageal pH monitoring. This technique only allows detection of acid GOR. The acidity of gastro-oesophageal reflux depends on the acidity, volume and distribution of gastric contents. It has been suggested that in the early postprandial period and during the night, gastro-oesophageal reflux might have a less acidic pH (between 7 and 4).7 In CF patients, the volume of gastric contents, acidity and concentration of bilio-pancreatic components might be modified and this might affect the characteristics of GOR. Combined impedance–pH monitoring is a more sensitive technique that allows detection of all types of gastro-oesophageal reflux events (acid and weakly acidic).8 The prevalence of weakly acidic reflux in patients with CF is unknown.
Previous studies have shown that chronic cough might be associated with acid and weakly acidic reflux9–11 and this could also be the case in CF patients. The precise temporal relationship between reflux and cough in patients with CF is unknown. It is frequently proposed that reflux might be a secondary phenomenon in CF. If this were the case, most reflux events should occur together with or after coughing. The simultaneous measurement of reflux with impedance–pH metry and objective detection of cough with gastro-oesophageal ambulatory manometry allows a precise assessment of the reflux–cough relationship.9
Increased GOR in CF might induce typical GORD symptoms like heartburn and regurgitation or even oesophagitis. The most important concern about GOR in CF is the possibility of reflux-induced lung aspiration of gastric contents with deterioration of lung function. This concern has been supported by the observation that CF patients with increased acid GOR have poorer lung function than those without abnormal GOR.12 However, coexistence of GOR and poor lung function does not imply a causal relationship and, so far, there is no objective data showing abnormal presence of gastric contents in bronchial secretion of CF patients. Recent studies have shown the presence of markers of gastric contents in bronchoalveolar lavage (BAL) obtained during bronchoscopy in patients after lung transplant (LTx) including transplanted CF patients. It is unknown, however, whether CF patients have higher levels of lung aspiration than other LTx patients. Collection of BAL during bronchoscopy is not routinely performed in pre-transplant CF patients. Detection of gastric markers in saliva has been proposed as a surrogate for high proximal extent of GOR13 and might provide a non-invasive alternative to identify those CF patients with increased GOR and risk for lung aspiration.
The aims of our study were to (1) assess the prevalence of acid and weakly acidic reflux in adult patients with CF; (2) define the temporal relationship between reflux and cough and determine whether GOR is a primary or a secondary to cough phenomenon; (3) confirm the occurrence and assess the severity of lung aspiration of gastric contents in LTx patients with CF; and (4) assess the potential risk of aspiration in CF by measuring gastric markers in saliva.
METHODS
Subjects
Studies were performed in 71 adult CF patients (fig 1). Gastro-oesophageal reflux monitoring was performed in 23 non-transplanted and 10 lung transplanted (LTx) adult CF patients, proton pump inhibitor (PPI) treatment was discontinued for at least 7 days before the study. Enzymatic pancreatic supplements were continued during the study day. Patient characteristics are displayed in table 1. Lung function was assessed on the reflux monitoring study day. Thirty-one patients were studied at the adult CF centre of the University Hospital Gasthuisberg, K.U.Leuven, two non-transplanted CF patients were studied in the Vrije Universiteit Brussels. In the 10 CF patients after LTx, the presence of chronic rejection, defined as an irreversible decline in forced expiratory volume in one second (FEV1), was graded according to ISHLT criteria.14 Informed consent was obtained from all subjects.

In a separate group of 38 CF patients attending the outpatient clinic of the adult CF centre of the University Hospital Gasthuisberg, K.U.Leuven, saliva samples were collected for the determination of bile acids. Eleven of these patients were studied “on” empirical PPI treatment (omeprazole 20 mg).
MONITORING OF GASTRO-OESOPHAGEAL REFLUX AND COUGH
Reflux detection (impedance–pH recording)
Gastro-oesophageal reflux was monitored using ambulatory impedance–pH metry (Sleuth, Sandhill Scientific, Highlands Ranch, CO, USA). Oesophageal impedance–pH was recorded with a 2.1 mm diameter catheter that comprised six electrode pairs to measure intraluminal impedance and two antimony pH sensors. The proximal pH sensor was positioned 5 cm above the LOS, the distal pH sensor in the stomach and the impedance channels were positioned 3, 5, 7, 9, 15 and 17 cm above the LOS.
The impedance–pH recording was analysed using criteria described in a recent consensus report on detection and definitions of acid, non-acid and gas reflux.8 Reflux was defined as acid if the pH fell below 4 for at least 4 s or, if the pH was already below 4, as a decrease of at least 1 pH unit sustained for more than 4 s. Weakly acidic reflux was defined as a pH decrease of at least 1 pH unit sustained for more than 4 s with the basal pH remaining between 7 and 4.
For each patient, the total number of reflux events (acid, weakly acidic), the proximal extent of reflux (number of episodes reaching 15 cm above the LOS) and the exposure of the oesophageal body to acid and volume were calculated. Total 24 h acid exposure was calculated as the percentage of time that the oesophageal pH was below 4. Total volume exposure per 24 h was obtained from the impedance tracing by addition of the volume exposures during reflux measured at 5 cm above LOS. The number of reflux events and the volume exposure were regarded as increased if these values were above the 95th percentile of normal data obtained in healthy subjects.15
Cough detection (manometry)
In non-transplanted CF patients, the exact time relationship between reflux and cough was assessed by adding to the ambulatory reflux monitoring a simultaneous gastro-oesophageal manometric recording. A separate thin (2.7 mm external diameter) manometric catheter with two solid-state pressure sensors (15 cm apart) (Unisensor, Attikon, Switzerland) was positioned so that one pressure channel was located in the oesophageal body (5 cm above LOS) and the other in the stomach. The impedance–pH and manometric catheters were connected to a single ambulatory device containing the respective amplifiers (Sleuth, Sandhill Scientific). All signals (impedance, pH and manometry) were digitised at 50 Hz and stored in the data logger. Simultaneous impedance–pH–manometric recordings were obtained in 16/23 non-transplanted patients. The double intubation procedure was not tolerated by seven patients.
The manometric tracing was independently analysed for cough episodes. A “cough burst” was defined as two or more rapid simultaneous pressure peaks within 3 s, which occurred in both manometric channels with the same configuration (fig 2).16

As in our previous studies on GOR related cough9 only “cough bursts” were considered in the reflux–cough association analysis.
Cough-inducing reflux
A reflux event was considered “induced by” cough if the cough occurred in the 30 s preceding reflux (fig 2). The total oesophageal acid and volume exposures due to cough were calculated by adding the acid and volume exposures (in seconds) at 5 cm above the LOS from the individual reflux events “induced by” cough, divided by the total recording time.
Reflux-inducing cough
A 2 min time interval following the start of a reflux episode was used to delimitate the time window for reflux–cough association. A 2 min period was chosen based on previous analysis of acid reflux–chest pain association.17 Thus, if a cough episode occurred in the 2 min time period after the start of a reflux event, cough was considered “induced by reflux” (fig 2). The statistical significance of the association between reflux and cough was assessed using the symptom association probability analysis (SAP). The SAP was calculated as previously described; SAP values greater than 95% were considered statistically significant.18
Monitoring of bile acids in bronchoalveolar lavage and saliva
Bile acids assay
BAL and saliva samples were analysed for the presence of total bile acids using a commercially available enzymatic assay (Bioquant, San Diego, USA). The lowest level of accurate detection for this assay was 0.2 μmol/l.
Bronchoalveolar lavage
Bile acid concentration was measured in BAL samples of 10 transplanted CF patients obtained at routine follow-up bronchoscopy. As control, bile acid was measured in BAL samples from (1) 24 patients who underwent lung transplantation for indications other than CF and (2) 14 non-transplanted non-CF patients (11 lung cancer, two chronic obstructive pulmonary disease (COPD), one non-Hodgkin lymphoma).
Saliva
Bile acids concentration was measured in saliva samples collected in fasting condition in 38 non-transplanted CF patients [20 men, age 29 (18–56) years] attending the outpatient clinic. These patients did not undergo reflux testing. Standard samples of 1–2 ml were obtained using a commercially available method (Salivette, Sarstedt, Germany). As control, bile acid was measured in saliva from 10 healthy subjects [four men, age 24 (23–56) years], nine GORD patients [four men, age 38 (29–51) years] and 10 patients with chronic unexplained cough without GORD [four men, age 42 (19–53) years].
Statistical analysis
Data are presented as median (25th to 75th percentile). Comparison between groups was done with an unpaired t-test. Fisher’s exact test was used to calculate SAP. Statistical significance was accepted when p<0.05.
RESULTS
Gastro-oesophageal reflux
Impedance–pH metry detected increased gastro-oesophageal reflux in 20/23 non-transplanted and in 8/10 transplanted patients. From all CF patients who underwent reflux testing (n = 33), 21 had increased acid reflux (18 with high oesophageal acid exposure and three with increased number of acid reflux events). Two patients had increased acid and weakly acidic reflux and five patients had only increased weakly acidic reflux (three with high volume exposure and two with an increased number of weakly acidic reflux events. Twelve patients (36%) had an increased number of reflux episodes reaching the proximal oesophagus. A significant number of patients with increased reflux (16/28) did not have typical reflux symptoms.
There was no difference in reflux parameters between non-transplanted and transplanted CF patients. The oesophageal acid exposure, volume exposure, number of reflux events and the proximal extent of reflux were similar in both groups (table 2).
Patients with the DF508 homozygote genotype had fewer acidic gastric contents (per cent of time with gastric pH<4) and lower oesophageal acid exposure compared to the other genotypes (table 3).
Gastric aspiration
Bile acids in saliva
Patients with CF had more bile acids in saliva than controls. Bile acids were present in the saliva of 16/38 patients tested. Most of these patients had the DF508 homozygote genotype. None of the healthy controls, 3/9 patients with GORD and 4/10 patients with chronic unexplained cough tested positive for bile acids in saliva. Bile acids were present in saliva of 6/11 non-transplanted CF patients treated with PPIs. The concentration of bile acids in saliva was significantly higher in patients with CF [3.3 μmol/l (2.4–6.1)] compared to GORD [1.23 μmol/l (1.2–2.3)] and chronic cough patients [0.72 μmol/l (0.2–1.2)] (p<0.05).
Bile acids in bronchoalveolar lavage
Transplanted CF patients had more bile acids in BAL than controls. Bile acids were not detected in BAL of non-transplanted patients (0/14). In contrast, bile acids were detected in 6/10 CF transplanted patients (60%) and in 10/24 non-CF transplanted patients (41%). The concentration of bile acids in BAL was higher in CF transplanted patients [0.65 μmol/l (0.4–0.7)] than in non-CF lung transplanted patients [0.50 μmol/l (0.3–1.3)].
A significant number of CF patients with bile acids in BAL or saliva (13/22) did not have typical GOR symptoms.
Gastro-oesophageal reflux, gastric aspiration and respiratory status
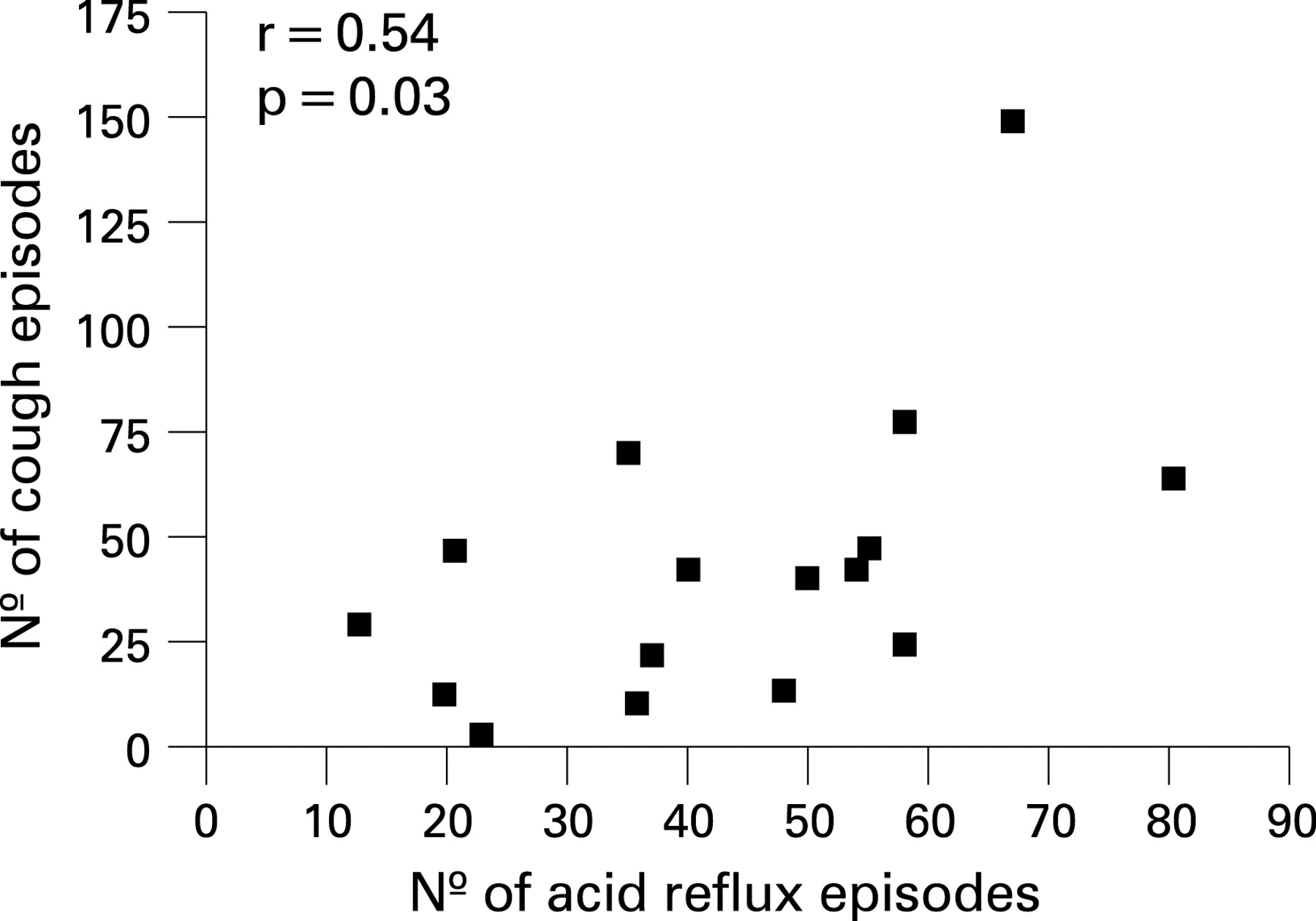
Cough was recorded simultaneously with gastro-oesophageal reflux in 16 non-transplanted patients. The median number of cough bursts events was 35 (4–149) per 24 h. There was a significant correlation between individual oesophageal acid exposure and number of coughs per 24 h (r = 0.53, p = 0.03) (fig 3).
The number of reflux–cough sequences [5 (4–10) per subject] was significantly higher than the number of cough–reflux sequences [2 (0–4) per subject], (p<0.02). A small fraction of the oesophageal acid exposure (0.4%) and volume exposure (0.106%) was secondary to cough.
Ten of the 16 patients showed a statistically significant association for the reflux–cough sequence: six had a positive SAP for acid reflux and four had a positive SAP for weakly acidic reflux. Moreover, patients with a positive SAP had a significantly lower lung function (FEV1% predicted) compared to patients with negative SAP (55 (32–74) vs 78 (55–92); p<0.05) (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The lung function (FEV1% predicted) was slightly lower in CF patients with bile acids in saliva compared to patients without [61% (38–82%) vs 71% (61–79%)]; however, this difference was not statistically significant.
The lung function was slightly lower in transplanted CF patients with and without bile acids in the BAL [FEV1%best: 73.0% (SD 32.0%) vs 92.3% (SD 4.4%); p = 0.2], respectively. Interestingly, 2/6 patients with bile acids in the BAL developed bronchiolitis obliterans syndrome (BOS), compared to none of the patients without bile acids in the BAL.
DISCUSSION
It is known that GOR is increased in patients with cystic fibrosis; however, its prevalence, characteristics, association with gastric aspiration and respiratory impact are not well characterised. In the current study we investigated acid and weakly acidic reflux, markers of gastric aspiration and respiratory symptoms and function in adult patients with cystic fibrosis (CF). The main findings of the study were (1) 80% of CF patients have increased GOR, mostly acid GOR, with a subgroup having increased weakly acidic reflux; (2) a significant group of CF patients have risk of gastric aspiration (increased bile acids in saliva) or definite gastric aspiration (bile acids in BAL); (3) half of the CF patients with increased GOR or gastric aspiration do not present oesophageal symptoms like heartburn or regurgitation; (4) the characteristics of GOR and material aspirated depends on the genotype, with bile aspiration being more important in DF508 homozygotes; and (5) the causal relationship between GOR, aspiration and respiratory symptoms is not completely elucidated. However, our results suggest that (1) gastro-oesophageal reflux in CF is a primary phenomenon and not secondary to cough; (2) there is a positive correlation between oesophageal acid exposure and the number of cough epsisodes per 24 h; and (3) a positive association between reflux and cough is associated with poorer lung function.
Gastro-oesopahgeal reflux has been associated with respiratory diseases such as chronic cough and the development of chronic rejection after lung transplantation.9 10 19 In 1975 GOR was first reported in patients with CF.20 Since then several studies described a high prevalence of acid GOR in CF patients, ranging from 35 to 81%.1–4 20–24 The majority of these studies used oesophageal pH monitoring for GOR detection. In our study we used oesophageal impedance–pH metry that allows detection of both acid and weakly acidic reflux. We found a large percentage of CF patients with increased total GOR. The increased GOR in CF patients was mainly due to increased acid GOR in 70% of the patients, confirming the results of previous studies. Additionally, we could identify a subgroup of five patients with increased weakly acidic reflux. The prevalence of weakly acidic reflux was relatively low compared to other patients with chronic unexplained cough and GORD. The reason for this is not clear. We speculate that patients with CF might have a different pattern of acid/weakly acidic reflux due to modifications of gastric volume or concentration of bile, specific to the disease. It has been previously demonstrated that patients with CF have increased gastric acidity.2 25 26
The prevalence of GOR was similarly high in CF patients, irrespective of whether they underwent LTx or not. Recent studies suggested that the lung transplant procedure, by itself, can increase GOR and the risk of gastric aspiration.27 The increased GOR after LTx was attributed to a significantly prolonged gastric emptying.28 Although we did not study the same patients before and after LTx, our cross-sectional data argue against a major impact of LTx on an already increased prevalence of GOR in CF patients.
A significant group of our CF patients showed increased risk of gastric aspiration (increased bile acids in saliva) or definite evidence of gastric aspiration (bile acids in BAL). It is generally accepted that gastric aspiration may occur in CF patients. The evidence available is scarce, however, and based on one study demonstrating tracheal acidification.29 More recent studies have demonstrated the highest levels of pepsin and bile acids in BALF in a group of CF LTx patients.19 Our study suggested that the risk and prevalence of aspiration in CF could be even higher than previously accepted.
We found bile acids in BALF in 60% of the LTx CF patients. Previous studies have demonstrated the presence of pepsin or bile acids in BALF of LTx patients.19 30–33 However, the concentration of bile acids in BALF in our CF patients was significantly higher compared to that observed in LTx patients with other end stage lung diseases.
Our results also showed that 42% of the CF patients had bile acids in the saliva compared to none of the healthy controls. As in BALF, the concentration of bile acids in saliva from CF patients was significantly higher than that observed in patients with chronic cough or GORD. Interestingly, bile acids were present in saliva from 6/11 patients treated with PPIs, suggesting that the risk of bile acid aspiration persists in spite of empirical treatment with a low dose of antacids.
The reasons why CF patients have increased bile acids in saliva and BALF remain to be elucidated. A study by Hallberg et al34 showed increased duodeno-gastric reflux in CF. In our study, bile acids were found in saliva and BAL of CF patients with the DF508 homozygote genotype. This finding suggests that this genotype is associated with abnormal intestinal motility that might favour duodeno-gastric reflux and increase the bile acids concentration in the stomach. Furthermore, increased duodeno-gastric reflux with bicarbonate may have a neutralising effect on gastric contents which might explain the decreased gastric acid exposure observed in our patients who are homozygous for DF508 mutation. Further studies on gastric secretion and distribution of gastric contents in CF are needed to test this hypothesis.
In CF patients, the causal relationship between GOR, aspiration and respiratory symptoms has never been completely clarified. Whether GOR is a primary phenomenon or secondary to cough or physiotherapy has been a matter of debate. Early studies demonstrated increased reflux in infants and children before development of significant respiratory disease, suggesting that GOR is a primary disorder.3 4 35 On the other hand, multiple medications that can impair lower oesophageal sphincter pressure, chest physiotherapy and frequent coughing have been suggested to provoke reflux as a secondary phenomenon. Our study provides evidence that GOR is a primary event in CF. Chest physiotherapy is performed on a daily basis in CF patients and has been associated with exacerbation of GOR.36 37 It has been suggested that the increase in intra-abdominal pressure with coughing may be responsible for increased reflux in CF (cough–reflux).2 Our study is the first to investigate the temporal relationship between cough and reflux using objective techniques for cough and reflux recognition.9 10 16 We observed that the cough–reflux sequence is a rare finding in patients with CF. Cough was responsible for a very small portion of the oesophageal acid (0.4%) and volume exposures (0.1%). Despite the finding that, overall, only a small fraction of cough was preceded by reflux, a per individual analysis showed a significant relationship between reflux and cough in 10 patients with a +SAP. These data favour the concept of reflux as a primary phenomenon in CF.
It has been suggested that GOR may provoke respiratory symptoms and contribute to reduced respiratory function in CF. CF patients with increased GOR may have a poorer lung function compared to CF patients without GOR and anti-reflux treatment has been associated with an improvement of the evolution of the FEV1.12 38 However, other studies failed to show a relationship between reflux and pulmonary damage.39
Impairment of lung function in CF is multifactorial. As a result a direct relationship between reflux parameters and impairment of the lungs might not be evident. However, results of our study suggest a potential role for GOR in symptom generation and possibly progression of the disease. Firstly, we found a significant correlation between the number of coughs and the oesophageal acid exposure. This correlation may be due to microaspiration but also to possible enhancement of the physiological cough reflex. A recent experimental study in cats showed that oesophageal acidification increases tracheobronchial mucus secretion.40 An oesophageal acidification-induced increase in mucus secretion might provoke increased coughing in CF patients. Secondly, patients with a significant positive association between reflux and cough (SAP+) had a significantly lower pulmonary function (% predicted FEV1) compared to SAP− patients. Thirdly, in the group of post-LTx CF, two patients with evidence of gastric aspiration developed BOS compared to none of the patients without increased GOR or gastric aspiration. These findings are in agreement with other studies showing an association between bile acid aspiration and development of chronic rejection after LTx.19 30 31 However, the observation that patients with bile acids in saliva did not have a significantly lower FEV1 argues somewhat against this hypothesis. Alternatively, we need to consider an indirect non-causal relationship between FEV1 and aspiration based on the genotype association. Patients who are homozygous for DF508 have a higher prevalence of bile acid aspiration in our study but this genotype has also been associated with an increased CFTR impairment resulting in a more progressive decline of the pulmonary function.
Although the above findings provide some indication for the relevance of GOR in patients with cystic fibrosis, further prospective intervention studies are required to confirm the impact of GOR in the progression of the disease. For this purpose, objective detection of increased GOR or risk of aspiration is mandatory. Despite the high prevalence of GOR in our patient population, only a minority of patients with increased GOR had typical reflux symptoms (heartburn or regurgitation) suggesting that typical reflux symptoms questioning is not sufficient for the diagnosis of GOR or gastric aspiration in CF.
In conclusion, gastro-oesophageal reflux is a primary and very prevalent phenomenon in adult patients with CF. Acid reflux is predominant but a subgroup of patients may only have increased weakly acidic reflux. Patients with cystic fibrosis have a high risk for gastric aspiration even in the absence of typical reflux symptoms. Although outcome studies are needed to further identify the role of GOR in CF patients, our results suggest that gastro-oesophageal reflux should be objectively measured in CF and treated accordingly to prevent gastric aspiration and its possible deleterious effects.
REFERENCES
Footnotes
Funding: This work was supported by a grant of the Fonds voor Wetenschappelijk Onderzoek (FWO) Vlaanderen, a grant of the Belgian CF Foundation (BVSM) and an educational grant of AstraZeneca Belgium. DS received a research grant from Sandhill Scientific, Denver USA. LJD is a part-time senior research fellow of the FWO Vlaanderen.
Competing interests: None.
Ethics approval: This study was approved by the Ethics Committee of the University Hospital Gasthuisberg, K.U.Leuven, in July 2000.