Article Text

Abstract
Unfavourable effects on the respiratory and the cardiovascular systems from short-term and long-term inhalation of air pollution are well documented. Exposure to freshly generated mixed combustion emissions such as those observed in proximity to roadways with high volumes of traffic and those from ice-resurfacing equipment are of particular concern. This is because there is a greater toxicity from freshly generated whole exhaust than from its component parts. The particles released from emissions are considered to cause oxidative damage and inflammation in the airways and the vascular system, and may be related to decreased exercise performance. However, few studies have examined this aspect. Several papers describe deleterious effects on health from chronic and acute air pollution exposure. However, there has been no research into the effects of long-term exposure to air pollution on athletic performance and a paucity of studies that describe the effects of acute exposure on exercise performance. The current knowledge of exercising in the high-pollution environment and the consequences that it may have on athlete performance are reviewed.
Statistics from Altmetric.com
Evidence supports unfavourable effects from short-term and long-term inhalation of air pollution to the respiratory and the cardiovascular systems.1,–,10 Combustion-related pollutants such as nitrogen and sulphur oxides, the ammonium ion, organic aerosols, particulate matter (PM) and ozone are of concern. Inhaled PM can be causal to oxidative stress-related airway and vascular injury. Although there is ample evidence of short-term and long-term exposure affecting the respiratory and the cardiovascular systems, little data are available demonstrating the effects of air pollution inhalation on athlete performance.10,–,12 During athlete training and competition, lung deposition of emission-related pollutants is high because of the increased ventilation during exercise,13 14 and inhalation of emission pollutants has been shown to cause the release of inflammatory mediators from airway cells.15 16 Furthermore, the asthmatic response is worsened by high emission pollution.17 This study describes combustion-related pollutants that are of concern to the athlete, examines adverse health effects of inhaling airborne pollution during exercise and presents current evidence that suggests that athletic performance is compromised by inhalation of emission-related aerosols during exercise.
Categories of particulate matter
Exposure to freshly generated mixed combustion emissions such as those observed in proximity to high volumes of traffic is of particular concern since evidence supports a greater toxicity from the freshly generated whole exhaust than from its component parts.15 Further, PM toxicity has been shown to be related to particle surface area, number count and particle charge.18
Airborne PM is categorised by aerodynamic diameter and includes the primary categories of coarse, fine and ultrafine particles. Particles larger than 10 µm are not considered harmful to airways since they are primarily filtered at the nasopharyngeal region. Coarse particles (PM10) include those between 2.5 and 10 µm in diameter, fine particles (PM2.5) are particles smaller than 2.5 µm in diameter and ultrafine particles include those less than 0.1 µm diameter.19 The establishment of a separate category for particles less than 2.5 µm is based on research demonstrating that these smaller particles are more toxic because of their deeper penetration within the airways of the lung. PM less than 1 µm in diameter (PM1) are recorded in many studies, primarily because of portable equipment limitations. This size range typically includes particles in the 0.05 to 1 µm in diameter and is a suitable representation of freshly generated particles. Although ultrafine PM (PM0.1), are not yet recognised by the US Environmental Protection Agency (EPA), they are considered to be the most harmful.4 13 14 18 20 Ultrafine particle concentrations are high in freshly generated exhaust and can penetrate deep within the lung, but rapidly decrease in number count over time by agglomeration and dispersion (figure 1).21

Sixty-two days of particle counts on an athletic field within 50 m of a high-traffic road. The x-axis is particle counts of particles <1 µm in diameter, those emitted from auto and truck emissions. Note that a rather rapid decay in number count is related to the distance from the source. Redrawn.21
PM from freshly generated exhaust emissions are likely to be the most toxic because they are highest in number count and surface area and are in the particle size range of 50 to 100 nm (or about 1/1000 the diameter of a human hair) (figure 2). Fractional deposition of these 50 to 100 nm particles occurs in the alveolar region where exchange with the circulation may occur. Although coarse and fine particles are monitored by the EPA, most toxicology research has investigated ultrafine particles (PM0.1) and field research has primarily measured PM1. An increased deposition fraction (fraction of inhaled particles remaining in the lungs after inhalation) of PM during exercise has been identified, with the largest deposition fraction noted for ultrafine particles. For example, the fractional deposition13 of PM0.1 is increased 4.5-fold during mild (38 l/min) exercise (figure 3).14 For PM2.5, it has been estimated that 9% is deposited in the lungs with 6% reaching the alveolar region.22 Exercise appears to increase the deleterious effects of PM inhalation by deposition, while damaged airway epithelium from mechanical stress of high ventilation may enhance particle infiltration to the circulatory system.

Size distribution in number count of freshly generated emission particles. Note the largest number count is in the 50–60-nm size range.

PM toxicology
The precise toxicological mechanism(s) of inhaled PM has not been established; however, oxidative stress from exposure is likely involved. It is thought that inhalation of emission pollutants causes a release of inflammatory mediators from airway cells that then enter the circulatory system, causing increased systemic oxidative stress. A decrease in lung antioxidants from in vitro carbon black exposure has been identified and suggests that the epithelial lining fluid-PM interface may represent an important initial PM detoxifying step.23 This could be critical to the exercising athlete as it is known that there is transient loss of airway surface liquid from high ventilation of dry air, making airway cells more vulnerable to effects of air pollutants. An acute twofold increase in lung antioxidants of rats exposed to diesel exhaust PM has been identified,24 suggesting a protective role against PM-induced oxidative stress for lung antioxidants. As a consequence to exercise in high emission pollutants, a 44% decrease in total nitrate and a 40% increase in malondialdehyde in exhaled breath condensate were found, supporting formation of the powerful oxidant, peroxynitrite9 from the reaction of nitric oxide (NO) and superoxide. Alternatively, NO reacts with glutathione in the lung to form a potent airway bronchodilator, S-nitrosoglutathione (GSNO).25,–,27
Studies have shown that reduced GSNO in the asthmatic airways could support increased leukotriene (LT) production, while high levels could inhibit LT production.28 Since a predominantly LT-mediated bronchoconstriction after exercise in high PM has been shown,29 and marked glutathione depletion (to ∼20% of pre-exposure levels)24 occurs in lung epithelial lining fluid after particle exposure, GSNO depletion may be, in part, responsible for PM-induced LT production.
If present in training and competition environments, freshly generated particles are of specific concern to athletes, and are likely to be related to the high prevalence of airway disease among certain athletic populations. The prevalence of exercise-induced bronchoconstriction (EIB), asthma and low resting lung function is high for athletes who train and compete in a high PM-emission environments – far exceeding that of the non-athlete and the low-pollutant-exposed athlete. Pollutants from auto and truck emissions, high emissions from fossil-fuel-powered ice-rink resurfacers and ski-waxing fumes all negatively affect the pulmonary and cardiovascular systems.
Potential consequences of inhaling pollutants during exercise include decreased lung function, increased exacerbations of asthma/EIB, decreased diffusion capacity, pulmonary hypertension, cardiovascular effects and decreased performance. McCreanor et al17 demonstrated the effect of a 2-h walk while breathing high-PM/high-ozone air compared with low-PM/low-ozone air on asthmatic airways. There was a concurrent significant decrease in forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) from the high-PM/high-ozone exposure exercise, while lung function remained unchanged from walking in low-PM/low-ozone air (figure 4). An almost sixfold increase in sputum myeloperoxidase after the high-PM walk was also observed, suggesting neutrophilic inflammation.

Lung function of asthmatic subjects during and after a 2-hour walk in either low or high freshly generated diesel emissions. Redrawn.17
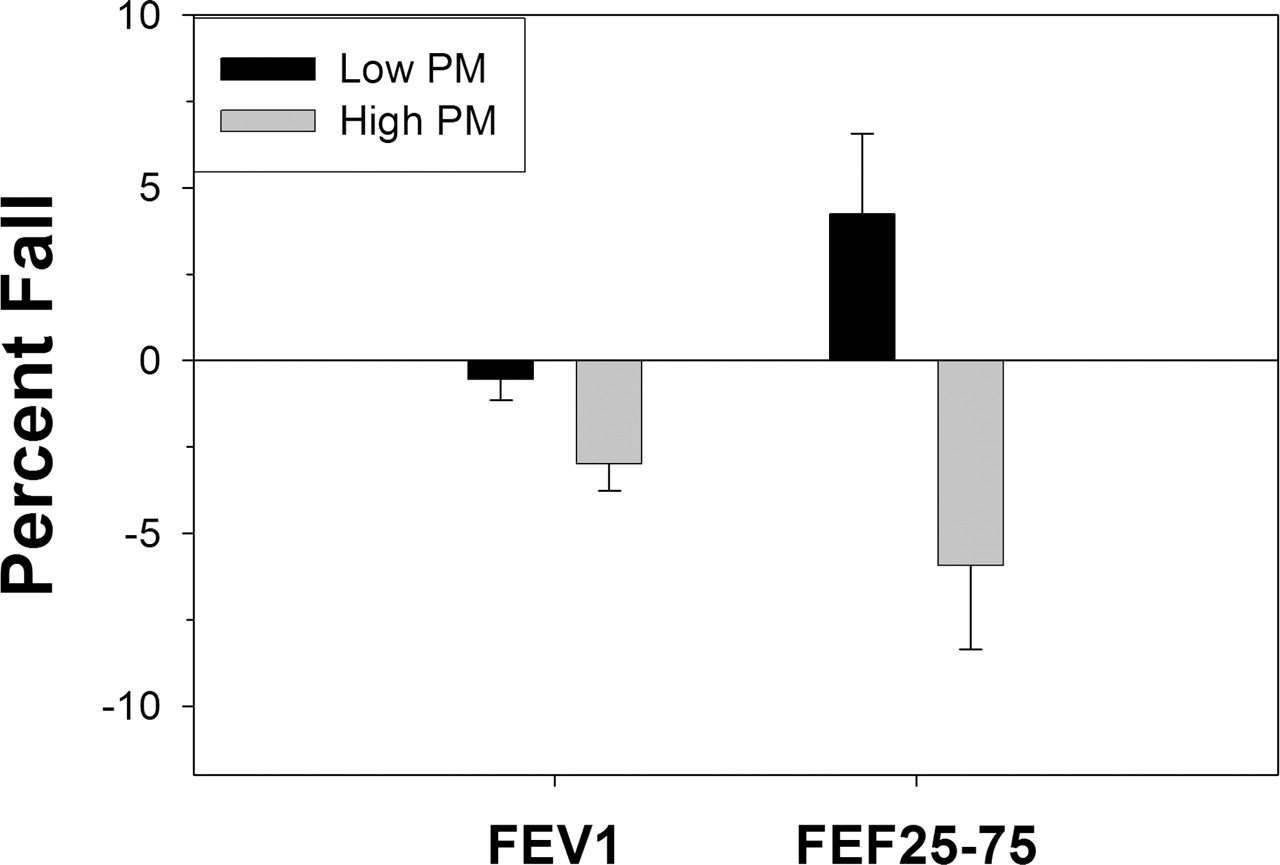
The high levels of PM1 observed at athletic fields and playgrounds in close proximity to major highways (figure 1) can affect pulmonary and vascular systems of healthy athletes. Only 30 min exposure to high-PM (>60 000 particles/cm3)/high-ozone (106 to 300 ppb) ambient air during exercise causes a small but significant decrease in lung function in non-asthmatics (figure 5).9
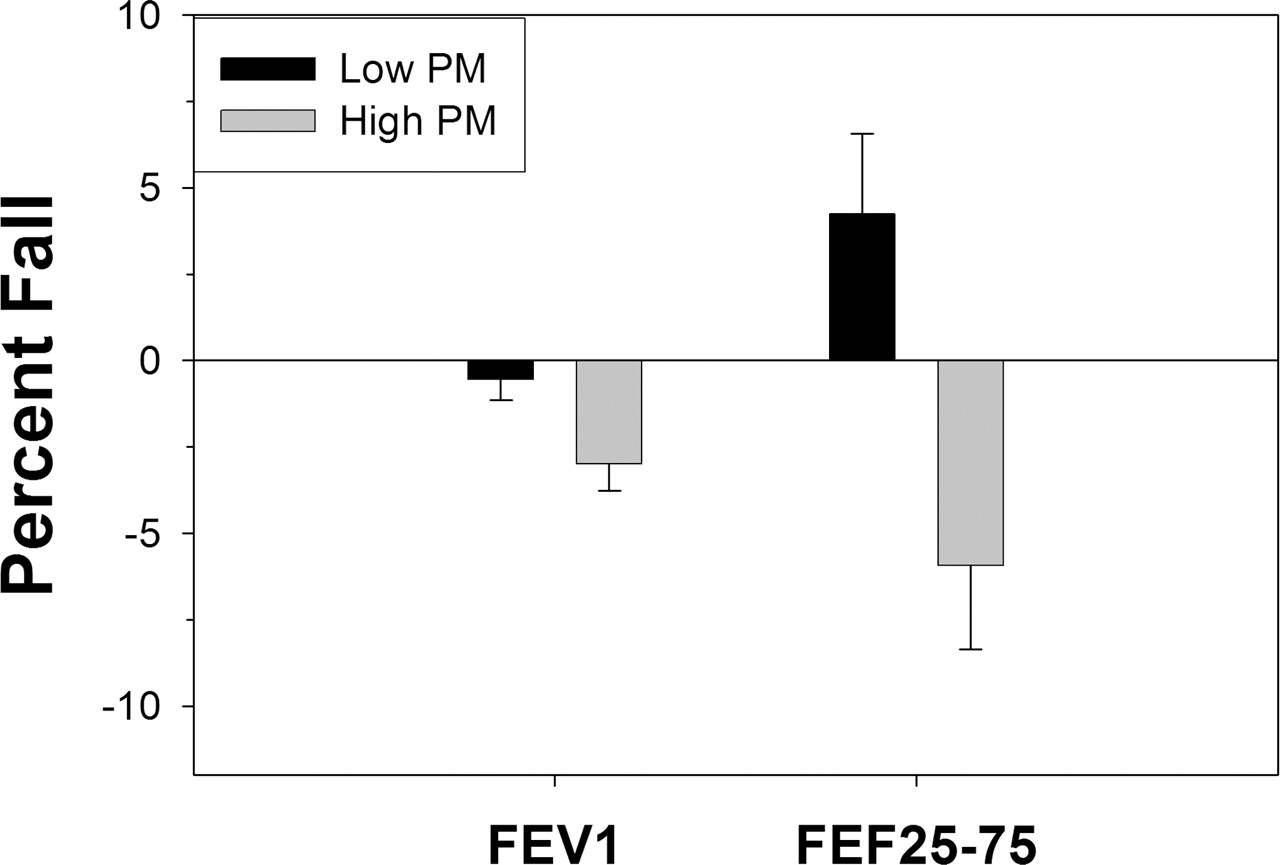
Significant change in lung function (forced expiratory volume in 1 s (FEV1) and FEF25–75) of non-asthmatic subjects after 30-min of high-particulate matter (PM1) exercise was identified. No change in lung function was noted from low-PM1 exposure exercise (p=0.0005 for FEV1 and p=0.002 for FEF25–75). Redrawn.9
Inhalation of air pollution also has negative effects on the vascular system. Thirty minutes of exercise in high-PM air resulted in a basal vasoconstriction of the brachial artery, disrupted normal vascular endothelial function, decreased flow-mediated dilatation response and a 55% decrease in reoxygenation of the muscle microcirculation.8 Arteriole dilatation was reported to be impaired after pulmonary exposure to particles and myeloperoxidase was found on adhering neutrophils on the vascular endothelial wall.30 It was proposed that this may affect the influence of NO on vascular tone and that the decreased tissue perfusion of the microvasculature from particle inhalation may compromise muscle function. Cutrufello et al10 noted an increase in pulmonary artery pressure as well as disrupted flow-mediated dilatation after 20-min of exercise in freshly generated four-cycle exhaust (PM0.1>300 000 particles • cm−3, CO<5 ppm).
Athlete PM exposure
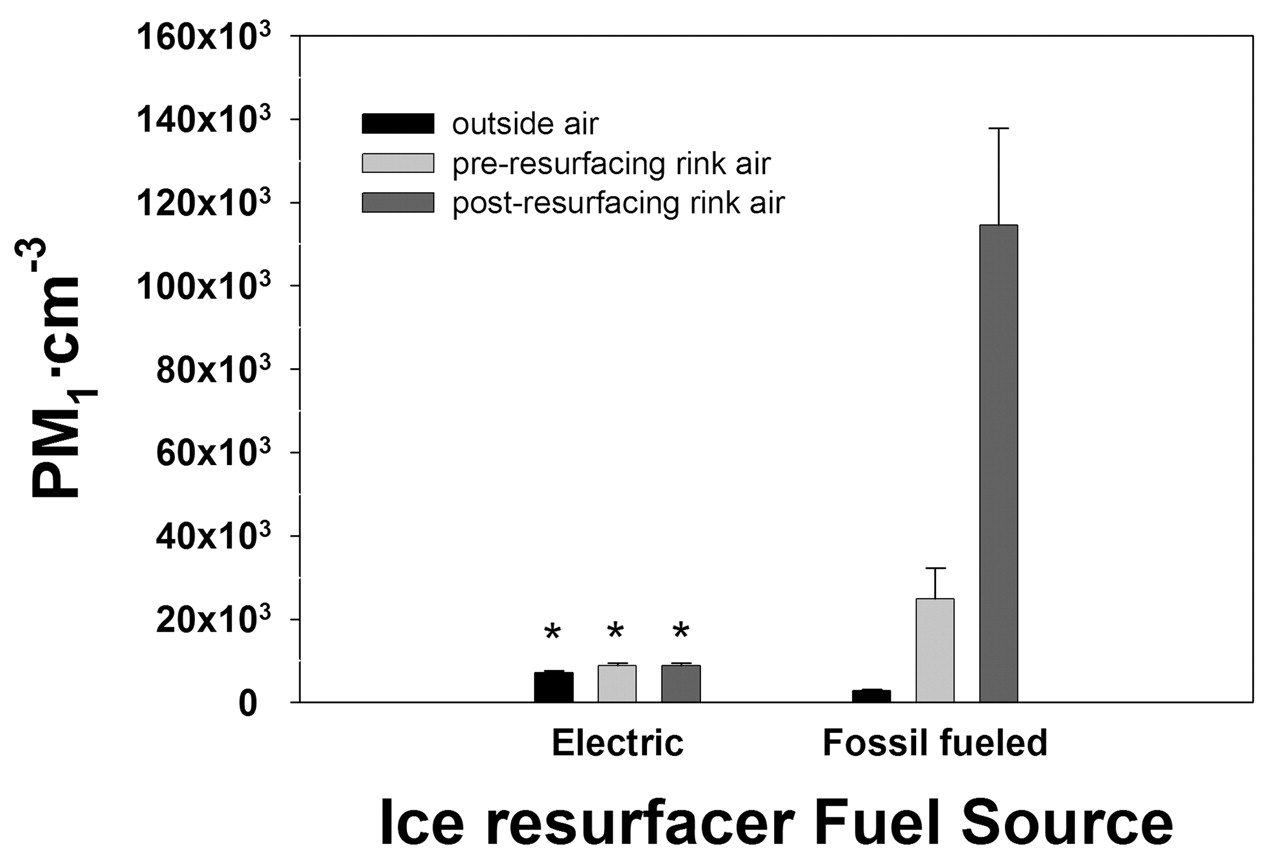
Ice-rink air is notoriously high in emission pollutants generated from combustion-powered ice resurfacers.31 There have been numerous cases of NO2 and CO poisoning in ice rinks from ice-resurfacer exhaust emissions. Along with high NO2 and CO, high particle counts from fossil-fuelled ice resurfacers have been found.31 In one study, particle counts from rinks resurfaced with electric-powered resurfacers and those resurfaced with fossil-fuel-powered machines were compared.31 The particle counts in rinks using electric-powered resurfacers were not different to the particle counts of the proximal ambient air. Those rinks that were resurfaced by fossil-fuelled machines, however, had particle counts ∼30 times greater than proximal ambient air (figure 6). As a result of this study, the Vancouver 2010 Olympic Games used electric-powered ice resurfacers to ensure acceptable air quality at all 2010 Olympic ice rinks.

Measurements of PM1 at 10 ice rinks demonstrate significant increases in particulate matter (PM1) after rinks were resurfaced by fossil-fuelled machines. Rinks using electric-powered machines showed no increase in PM1. Redrawn.6
Recent papers examining ice-rink air quality31 and the relationship to EIB have associated the high prevalence of airway dysfunction in skating athletes to inhalation of PM1.6 7 The 20% to 43% prevalence of EIB reported in figure skaters, hockey players and short-track-speed skaters32,–,34 is much higher than the estimated 10% asthma prevalence in the US and the reported prevalence for summer Olympic Games, athletes.35 Repeated ventilation of cold/dry air during sport training and competition, combined with high levels of PM1, may enhance the expression of or directly cause EIB and airway damage. Long-term exposure can have significant effects on resting airway function.6 7 Significant decrease in FVC, FEV1 and FEF25–75 over a 3-year period of daily training in an ice rink with high PM1 from fossil-fuelled resurfacers in female hockey players has been identified.6 The decline in FVC and FEV1, with little change in the FEV1/FVC ratio, is characteristic of early asthma development.
For the Nordic and alpine skier, ski-waxing fumes from daily hot waxing provide a major contribution to exposure. Many of today's ski waxes are fluorinated and have been shown to have a negative effect on lung function.36 When applied to skis, a hot iron is used; termed ‘hot waxing’. Hot waxing results in ultrafine fluorine particles being released into the air in concentrations 25-fold higher than prewaxing. Animal studies have shown that these fluorine particles are quite toxic.37 Although exposure does not occur during exercise, it does occur on a daily basis beginning early in the skiers career, when lungs are susceptible to damage. This repeated exposure in combination with airway damage from high ventilation of cold dry air during competition and training may contribute to the airway dysfunction observed in Nordic skiers. Of course, the elite skier spends little time in the wax room, but young developing skiers do, since they wax their own skis until reaching the elite level. Consequently, there are many years of exposure to the developing lung on the path to becoming an elite-level skier.
Athlete performance and PM
Inhalation of high levels of combustion-derived PM during exercise has been shown to result in reduced exercise performance during short-term maximal-intensity cycle ergometry.10 12 A single 6-min exercise bout in high PM failed to reduce exercise performance; however, a second 6-min of exercise in high PM 3 days after the first resulted in decreased exercise performance. This observation supports a delayed inflammatory effect from the initial exercise.12 In a separate study, decreased work accumulation was observed in a high-intensity 6-min cycle ergometer ride that immediately followed a 20-min high-PM exposure ride at 60% of estimated maximal heart rate,10 suggesting that a rapid response can occur within a single 20-min exposure. In this study, low-PM (L) and high-PM groups (H) were randomised, but L and H pairs were exercised 1 day apart, to evaluate 24-h effect of exposure. Unlike the previous study,12 these results showed decreases in performance in both high-PM rides. This was thought to occur because the 20-min prework accumulation ride allowed time for a systemic inflammatory response to occur, whereas the earlier study12 did not incorporate that pretime trial 20-min ride. The performance decreases from exercise in high emission-generated PM air observed in those studies were about 5%12 and 3%, respectively (figure 7).10 The implications of these studies to the athlete competing in a high-air-pollution environment suggest that even a 20-min warm-up in high air pollution will have an impact on subsequent performance. Further, only one 6-min bout of exercise in high pollution may have a carryover effect that will decrease the performance in exercise 3 days later.

Blunted flow-mediated dilatation from exercise in freshly generated four-cycle emission aerosols has been observed (figure 8A).10 12 Significant increases in pulmonary artery pressure after high-pollution exercise were also noted (figure 8B).10 Vascular function was correlated with exercise performance and accounted for as much as 24.4% of the decline in exercise performance. The <5% performance decrements are quite significant to the competing athlete. For example, all but the last place finisher in the 3000-m steeplechase at the 2008 Olympics were separated by less than 5%. These studies provide evidence that high-PM conditions are likely to affect athletic competition. In a recent study which examined the times of the top three finishers in seven US marathons over the course of 8 to 28 years, performance decrements were associated with acute PM10 exposure among women but not men.11 These findings may suggest an even greater vulnerability among females and should be considered when making exercise recommendations to this population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A, B) Pre-exercise and postexercise flow-mediated dilatation (FMD) of the brachial artery for four trials of 30-min cycle ergometry in low-particulate matter (PM) and high-PM-emission air. FMD was significantly less for high-PM versus low-PM trials (p<0.05). Pre-exercise and postexercise pulmonary artery pressure was significantly greater in high PM versus low PM (p<0.005). Redrawn.10
The response to PM0.1 inhalation 24 h after exposure in healthy humans demonstrated significant increase in diastolic blood pressure, reduced heart rate variability and significant impaired vasodilatation of the brachial artery.8 Likewise, near infrared spectroscopy demonstrated a decrease in the reoxygenation slope after cuff ischaemia, suggesting a constrictive response in the microcirculation that supports a physiologically significant decrease in blood flow that could affect exercise performance.8
The vascular dysfunction associated with PM inhalation suggests reasonable means by which PM inhalation may result in a cardiovascular incident due to the increased load on the heart. However, this added stress on the heart is not likely to result in a cardiovascular incident in the healthy population, but may affect cardiac output and thus performance. Interestingly, just as LT receptor antagonists have been useful in the treatment of asthma, montelukast has been found to attenuate the vascular dysfunction associated with the brachial artery after PM inhalation.38 This protection against the vascular dysfunction associated with PM inhalation could potentially improve exercise performance in high-PM conditions.
Conclusion
Acute exposure to mixed exhaust aerosols during exercise can cause decreases in lung and vascular function in healthy and asthmatic subjects. Chronic exposure to mixed exhaust aerosols during exercise may result in decreased lung function and may promote vascular dysfunction, which appear to be related to increased airway and systemic oxidative stress. The physiological effects of high-intensity exercise in high levels of mixed exhaust aerosols support the observed compromised performance.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed