Article Text

Abstract
Rationale Advanced fibrosing interstitial lung disease (ILD) is often progressive and associated with a high burden of symptoms and poor prognosis. Little is known about the symptom prevalence and access to palliative care services at end of life (EOL).
Objectives Compare prevalence of symptoms and palliative treatments between patients dying with oxygen-dependent ILD and patients dying of lung cancer.
Methods Nationwide registry-based cohort study of patients with oxygen-dependent ILD and patients with lung cancer who died between 1 January 2011 and 14 October 2013. Prevalence of symptoms and treatments during the last seven days of life were compared using data in Swedish Registry of Palliative Care.
Measurements and main results 285 patients with ILD and 10 822 with lung cancer were included. In ILD, death was more likely to be ‘unexpected’ (15% vs 4%), less likely to occur in a palliative care setting (17% vs 40%) and EOL discussions with the patients (41% vs 59%) were less common than in lung cancer. Patients with ILD suffered more from breathlessness (75% vs 42%) while patients with lung cancer had more pain (51% vs 73%) (p<0.005 for all comparisons). Patients with ILD had more unrelieved breathlessness, pain and anxiety. The survival time from initiation of oxygen therapy in ILD was a median 8.4 months (IQR 3.4–19.2 months).
Conclusions Patients with ILD receive poorer access to specialist EOL care services and experience more breathlessness than patients with lung cancer. This study highlights the need of better EOL care in oxygen-dependent ILD.
- Interstitial Fibrosis
- Palliative Care
- Long Term Oxygen Therapy (LTOT)
- Idiopathic pulmonary fibrosis
- Lung Cancer
Statistics from Altmetric.com
- Interstitial Fibrosis
- Palliative Care
- Long Term Oxygen Therapy (LTOT)
- Idiopathic pulmonary fibrosis
- Lung Cancer
Key messages
What is the key question?
What is the quality of end-of-life care for patients dying with oxygen-dependent interstitial lung disease?
What is the bottom line?
Patients dying with interstitial lung disease frequently suffer from breathlessness and receive suboptimal end-of-life care across multiple domains.
Why read on?
The end-of-life needs for patients with interstitial lung disease have not been systematically described.
Introduction
Advanced fibrosing interstitial lung disease (ILD) is a group of often progressive and incurable conditions.1 ,2 The most common form of ILD, idiopathic pulmonary fibrosis (IPF), is associated with poor survival, and high symptom burden and poor quality of life as the disease progresses.2–5 ILD represents an increasing proportion of patients with chronic hypoxemic respiratory failure.6 There are no prevalence figures of IPF available in Sweden, but the rate probably approximates that of our neighbouring country, Finland, with 14–16/100 000 inhabitants.7
Despite this poor prognosis, palliative care remains underused in patients with ILD.8 This may be due to under-recognition of the palliative care needs and symptom burden, or unfamiliarity and discomfort with palliative therapies.9 Though oncology has largely embraced earlier integration of palliative care, which has translated into improvements in end-of-life (EOL) care for patients with lung cancer,10 palliative and EOL care for non-malignant diseases are now gaining increased attention. In pulmonary disease, this research has mainly focused on COPD and demonstrated a significant burden of unmet palliative care needs and lower quality of EOL care compared with patients with cancer.11–13 Similar attention is only beginning to be paid to ILD,8 ,14–16 but symptom burden and quality of EOL care in patients with ILD have yet to be quantified.
The aim of this study was to determine the period prevalence of symptoms during the last week of life and characterise their management at EOL in patients with oxygen-dependent ILD compared with terminal lung cancer. In making this comparison, we hope to highlight ways to improve the EOL care for patients with oxygen-dependent ILD.
Materials and methods
This was a nationwide registry-based cohort study including all patients starting long-term oxygen therapy (LTOT) for physician-diagnosed ILD in the Swedevox registry who died between 1 January 2011 and 14 October 2013. A previous analysis indicates that most patients suffered from IPF,17 so we have chosen to use the more inclusive and more accurate term fibrotic ILD. Analyses were carried out using the Swedish Registry of Palliative Care (SRPC) and including patients with ILD from Swedevox. The physiological data of patients with ILD at time of initiation of LTOT from Swedevox data were cross-linked with SRPC data on the last seven days of life using each patient's unique Swedish identification number.
Data on patients with oxygen-dependent ILD were compared with data from patients on the SRPC who died from lung cancer in the same time period. Lung cancer was identified using the tenth revision of the International Classification of Disease (ICD-10) by cross-linking SRPC data on cancer patients with Causes of Death Registry. ICD-10 code C34 for lung cancer as either underlying cause or the first five contributing causes of death was identified and included in the comparator group.
Swedevox
The Swedevox registry prospectively includes patients starting LTOT in Sweden with a population-based coverage of about 85%.18–20 It contains patients’ diagnosis requiring LTOT and physiological data including arterial blood gas tensions when breathing air and oxygen, body mass index (BMI) and FEV1 registered at the start of LTOT. Accuracy of ILD diagnosis in this registry has been previously validated.17 Details of the registry are described elsewhere.21
The SRPC
The SRPC is a national quality register of the care of patients during their last week of life regardless of place of care or diagnosis.22 ,23 During 2013, 87% of all deaths from cancer nationwide were included in the registry.24 SRPC contains data on the presence of breathlessness, pain, death rattle, nausea, anxiety and confusion during the last seven days of life and prevalence of provided treatment of ‘as needed’ medications for pain, nausea, anxiety and death rattle at least one day before death.22
The SRPC collects data through an EOL questionnaire completed retrospectively by the responsible nurse and/or physician within a week of the patient's death; all deaths are expected to be registered, irrespective of place of death, diagnosis, age or involvement of formalised palliative care. The report is based on the patient record and recall of the care that may not have been documented, preferably after a team discussion so as to include the experience of all team members.22 The version of the questionnaire that was used to collect data was launched in January 2011 (see online supplementary material for an English version of the questionnaire). The questionnaire is completed online and all questions must be answered before submission. A previous study supported the validity of the questionnaire.25
Assessments
The period prevalence was estimated for each symptom from responses to the question, “Were any of the following symptoms prevalent at some time during the last week of life?” (yes or no). For any reported symptom, symptom relief was graded as relieved, partially relieved or unrelieved.
Prevalence of ‘as needed’ medication prescriptions was analysed among symptomatic patients for each identified symptom in response to the question, “Was medication prescribed for use as needed in the form of injections before death for pain, death rattle, nausea and anxiety?” (yes or no). This reflects prescription of medication, not necessarily administered doses.
Statistical analyses
Baseline characteristics were summarised using standard descriptive statistics. The differences among the groups were tested with t test for continuous and χ2 test for categorical variables. Multivariate logistic regression was carried out adjusting for age at death and gender. Statistical significance was defined as a double-sided p<0.05. Statistical analyses were conducted using the software packages Stata, V.12 (StataCorp; College Station, Texas, USA).
Results
Of an initial 490 patients with ILD in Swedevox who died between 1 January 2011 and 14 October 2013, 285 (58%) were registered in SRPC and included in the study (figure 1). Characteristics were similar between patients with LTOT who were and were not included in terms of age, sex, lung function, BMI and arterial blood gas levels (see online supplementary material table E1).

Flow chart of study population selection. ILD, interstitial lung disease; LTOT, long-term oxygen therapy; SRPC, Swedish Registry of Palliative Care.
In the SRPC, 10 822 patients died from lung cancer during the same time period and were included in the analysis as the comparator group. Characteristics of the patients with ILD and lung cancer are shown in table 1. Compared with patients with lung cancer, patients with ILD were slightly older (78±8 vs 73±10 years) and a smaller percentage were women (39% vs 48%). The survival time from initiation of LTOT was a median 8.4 months (IQR 3.4–19.2 months) (figure 2).
Baseline patient characteristics in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer

Kaplan–Meier survival curve in 285 patients with oxygen-dependent interstitial lung disease. LTOT, long-term oxygen therapy.
EOL care for patients with oxygen-dependent ILD had less palliative care input on nearly every measure (table 2). In ILD, death was more likely to be unexpected (15% vs 4%), less likely to occur in a palliative care setting (17% vs 40%) and there were fewer EOL discussions with the patients (41% vs 59%) and families (52% vs 73%). Validated symptom scales were used less frequently in patients with ILD for pain (13% vs 28%, p<0.001) and for other symptoms (8% vs 14%, p=0.004). Patients with ILD also had significantly greater period prevalence of breathlessness (75% vs 42%) than patients with lung cancer (table 3). In contrast, pain, death rattle and confusion were more common among patients with lung cancer. Nausea, and especially anxiety, was common, but similar between groups. Figure 3 illustrates symptom prevalence in both groups. Notably, there was a high rate of responding ‘don't know’ to the presence of many symptoms, higher in the ILD group for all symptoms (see online supplementary material table E2). For example, 21% of patients dying with ILD did not have the presence of breathlessness ascertained compared with 9% for lung cancer.
End-of-life (EOL) care in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer
Prevalence of symptoms at end-of-life (EOL) in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer

Prevalence (%) of symptoms in interstitial lung disease (ILD) (n=285) compared with lung cancer (n=10 822) at end of life in Sweden.
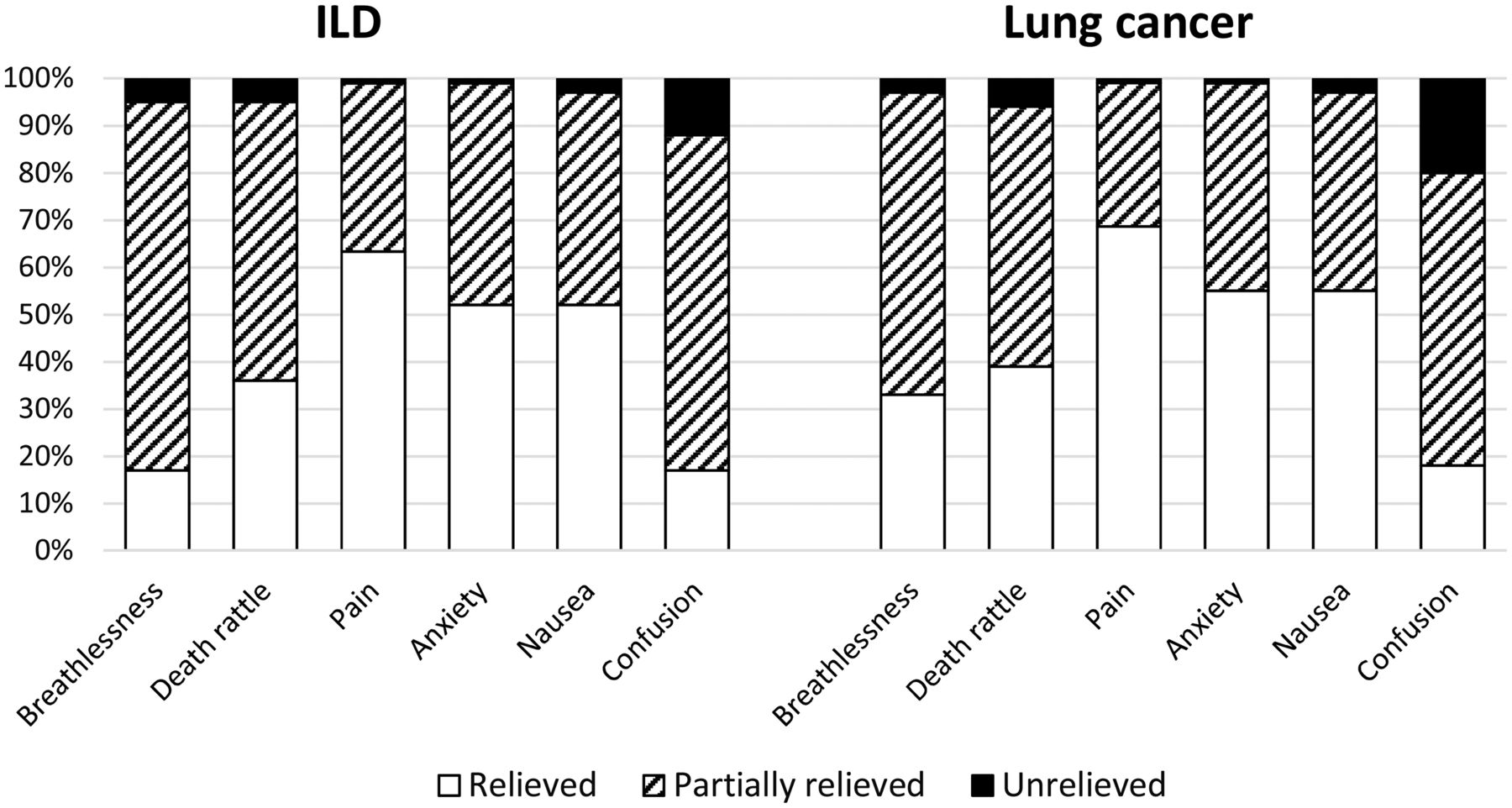
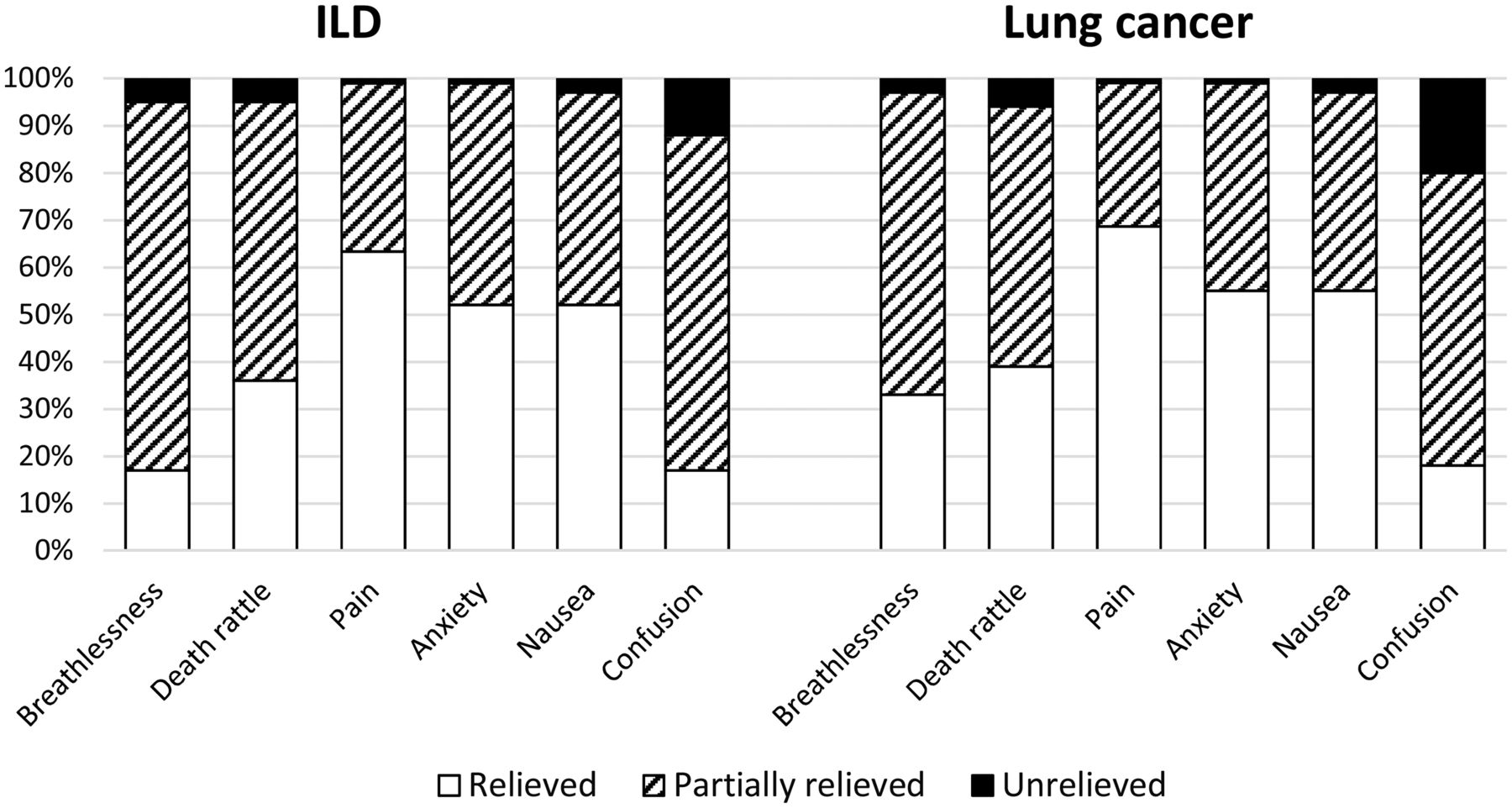
The prevalence of relieved and unrelieved symptoms is shown in table 4. Patients with ILD had lower rates of complete relief from breathlessness (17% vs 33%, p<0.001). Complete relief of pain (62% vs 70%, p=0.169) and anxiety (52% vs 55%, p=0.480) was similar (figure 4). Patients with ILD were less frequently prescribed as needed medications for death rattle (77% vs 88%), pain (83% vs 96), anxiety (79% vs 91%) and nausea (51% vs 73%); p<0.001 for all comparisons (table 5). An alternative analysis of the prescription data limited to patients who were symptomatic shows a similar result (see online supplementary material table E3). For example, 92% of patients with symptomatic ILD were prescribed as-needed medications for pain compared with 98% of patients with lung cancer (p<0.001). Treatment for breathlessness was not separately recorded.
Prevalence of symptom relief at end-of-life (EOL) in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer
Prevalence of ‘as needed’ medication prescriptions at end-of-life (EOL) in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Symptom management with prevalence (%) of relieved, partially relieved and unrelieved symptoms in interstitial lung disease (ILD) (n=285) compared with lung cancer (n=10 822) at end of life in Sweden.
The OR for breathlessness was more than three times higher for ILD compared with lung cancer (OR 3.49; CI 2.57 to 4.73), and the symptom ORs were similar adjusting for age and gender (table 6).
Odds of symptoms at end-of-life (EOL) in patients with oxygen-dependent interstitial lung disease (ILD) versus lung cancer
Discussion
Key findings
The present study suggests that patients dying with oxygen-dependent ILD receive lower quality EOL care and experience more breathlessness compared with patients dying of lung cancer.
To our knowledge, this is the first population-based study documenting symptom prevalence at the EOL using quantitative methods in people with ILD. Our findings are made more representative and robust due to its population-based and multicentre design. The other similar study of this size was single centre and could not include symptom prevalence.8 Furthermore, they included patients seen over many years in order to amass such numbers, and so their results may be less descriptive of current practices.
Our findings are consistent with other studies reporting underutilisation of specialised palliative care services in ILD.8 ,9 ,16 Underuse of specialised palliative care may lead to under-recognition of symptom burden and palliative care needs. Our data support this hypothesis in demonstrating a lower use of structured symptom assessments at EOL among patients with ILD.
While patients with lung cancer also suffer a high burden of symptoms at the EOL—particularly pain, death rattle and confusion—the frequency of complete relief of all symptoms met or exceeded that in ILD. This is likely explained in part by a greater rate of use of as-needed medications directed at all symptoms. Also, more frequent use of validated instruments for symptom assessment in cancer, and hence greater attention to distressing symptoms, could in part explain these differences. While not every symptom can or (depending on patient goals) should be completely relieved, these disparities suggest a quality issue in the provision of EOL care for ILD.
One explanation for our findings may be that pulmonologists are uncertain when and how to involve palliative care in advanced ILD. Though all recognise that ILD is progressive, the terminal decline often seems sudden or unpredictable, resulting in late referral to palliative care.8 Our data demonstrate a fairly rapid decline towards death in oxygen-depending ILD patients with a median survival time of 8.4 months after starting LTOT. This supports that referral to specialised palliative care should be offered when starting LTOT, if not earlier, and that palliative care services should be made available on an outpatient basis. A more proactive palliative approach may allow patients to avoid hospital admission at the EOL if that is consistent with the patients’ wishes.
Along these lines, some of the observed differences between these groups may be related to these disease-specific factors. For instance, perhaps the terminal decline in ILD is more sudden than in lung cancer and more difficult to predict. This may necessitate a higher frequency of hospital admission at the EOL, perhaps for acute symptom management. Still, even hospitalised patients with ILD had lower access of palliative care services.
Another potential explanation for the higher symptom burden in ILD may be that pulmonologists are unfamiliar or uncomfortable with palliative therapies in chronic respiratory failure. Breathlessness is the most prevalent symptom at EOL by far, yet studies have shown systematic under-recognition of breathlessness26 ,27 and unfamiliarity and discomfort with palliative care therapies for breathlessness.28 ,29 Some have described a therapeutic nihilism in treating breathlessness.30 Along similar lines, our data suggest that pain and anxiety are nearly as prevalent as breathlessness for patients with ILD at the EOL, arguing for a comprehensive assessment of palliative care needs.
Interestingly, the symptom burden and the poor quality of EOL care in ILD appears to be similar to COPD.31 Point estimates of nearly all measures for ILD are similar to a prior study of COPD using the same data sources.32 EOL care and symptom burden at EOL among non-malignant lung diseases are currently similar and inferior to the care provided to patients dying of cancer. Models for integration of respiratory and palliative care are emerging for COPD,33 and it is likely that patients with ILD will benefit from similar care models.
Strengths and limitations
Strengths of the present study include its national, population-based design and inclusion of the largest cohort to date of patients with ILD on LTOT and lung cancer. No previous studies have included the very last days of life among patients with ILD or used quantitative measures to report symptom prevalence. These features enhance the generalisability and interpretation of our findings.
Possible limitations of our study include that data on palliative care in SRPC were, by design, collected retrospectively. The questionnaire was answered by staff, which could be influenced by recall bias and social desirability bias, but it is unknown whether these biases would apply differentially to patients with ILD or cancer. Staff proxy assessments of symptoms in patients with advanced disease have been shown to be a valid alternative to patient self-report, especially for the detection of breathlessness. This was shown in patients with mostly cancer, and the validity of proxy reports in ILD has not yet been established.34
Another limitation is that the aetiology of ILD could be heterogeneous because our data did not allow further characterisation. It is, however, often difficult to obtain a specific diagnosis in patients with advanced ILD in the clinic. A previous study using the same data set supported the validity of the ILD diagnoses by having respiratory physicians using medical records, including available radiographic and histological data, and they found that most had IPF (according to the guidelines at that time).17 IPF is the most common fibrotic ILD, and it is associated with a high risk of progression to hypoxemic respiratory failure and death. Thus, the prevalence of IPF is most likely to be high in our sample of oxygen-dependent ILD. Furthermore, we expect the prognosis, symptom burden and care requirements between the various ILDs are likely to be more similar than different once these patients reach an oxygen-dependent stage.
Our data were also limited by some degree of missingness. Though all survey items were required before submission, the symptom assessments allowed a response of ‘don't know’, which was significantly higher in the ILD group for all symptoms. In light of this, the symptom prevalence data should be interpreted with caution as missingness of survey data is often non-random and the pattern may be informative. We are unable to determine whether a response of ‘don't know’ is more likely to be associated with symptom presence, or absence, and so may bias the prevalence estimates in uncertain ways. The reason for this differential missingness, though, may be explained by our main observation; that patients dying with ILD receive less palliative care, and this item may reflect less attention to symptom assessment and management.
Implications for practice
Though our analysis is limited to the EOL phase of care and suggests improvements in EOL care, the outcomes we describe have implications for care leading up to EOL as well. Our findings highlight the need to improve management of patients with oxygen-dependent ILD at an early phase, perhaps when starting LTOT, by better integrating respiratory and palliative care and improving access to specialised palliative care. Our data suggest poor advance care planning with nearly half of patients with ILD dying in the hospital, a rate that is nearly double that in cancer.
We believe better recognition of symptom burden for patients with oxygen-dependent ILD, perhaps through use of structured symptom assessments earlier in the disease course, could discover under-recognised palliative care needs. This could then lead to improved treatment of symptoms, advance care planning and proactive referral to specialised palliative care.
Improved palliative care for patients with ILD would likely improve symptom burden, but also the other equally important domains of palliative care including psychosocial and spiritual support for patient and carers.35 While we uncovered disparities in symptom burden, patients with ILD experienced lower quality of EOL care in multiple domains. As others have advocated, this patient population would benefit from comprehensive palliative care needs tools similar to those employed in cancer.36 ,37
Conclusion
Patients with ILD have less access to palliative care services and experience more breathlessness at the EOL than patients with terminal lung cancer. Further research is needed to elucidate the care structures, processes and evidence-based therapies that optimise palliative and EOL care for ILD and other advanced, non-malignant pulmonary diseases.
Acknowledgments
The analysis was carried out at the Department of Respiratory Medicine, Blekinge Hospital Karlskrona and Lund University, Sweden. The authors thank all the physicians and nurses who collected the data and cared for the patients.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement 1
- Data supplement 2 - Online supplement 2
Footnotes
Contributors ME had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Conception and design: NGW, ME and ZA; data acquisition: ME, SL and ZA; data analysis: ME and ZA; interpretation of data: CJ, DCC, ME, NGW, SL and ZA; drafting the article: NGW, ME and ZA; revision for important intellectual content: CJ, DCC, ME, NGW, SL and ZA; approval of the version to be published: CJ, DCC, ME, NGW, SL and ZA.
Funding This study was funded by The Swedish Society of Medicine, the Swedish Respiratory Society, the Swedish Heart-Lung Foundation, the Scientific Committee of Blekinge County Council and the Wera and Emil Cornell Foundation.
Competing interests None declared.
Ethics approval Ethics committee at the Department of Medical Ethics at Lund University, Lund, Sweden (reference number LundDNr: 2013/379).
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves