





Case history
A 77-year-old Caucasian female was referred to the renal team with a newly elevated plasma creatinine (288 mmol·L−1) associated with a 2-week history of malaise. Urinalysis demonstrated heavy proteinuria and renal biopsy confirmed the diagnosis of myeloma kidney. She was commenced on pulsed dexamethasone therapy (20 mg for 4 days in succession) before commencing thalidomide 50 mg daily. On day 10 of therapy, she was admitted to hospital with gradually progressive breathlessness for the previous 24 h, present at rest but made worse by exertion. She described a dry cough and ill-defined discomfort bilaterally over the thoracic cage. No haemoptysis was reported. Examination revealed reduced oxygen saturations of 85% on room air and a respiratory rate of 20 breaths·min−1. Auscultation of the chest disclosed bilateral scattered crackles. She had a trace of pitting peripheral oedema only and the jugular venous pressure was not elevated.
A plain chest radiograph was taken and is shown in figure 1.

Chest radiograph
Task 1
How would you interpret the chest radiograph?
Answer 1
There are coarse bilateral patchy infiltrates affecting all the visualised lung fields with relative sparing of the right costophrenic angle. The cardiothoracic ratio on this posterioranterior film is preserved. There is no radiological evidence of congestive cardiac failure. The appearances are in keeping with a diffuse interstitial process, with a wide differential diagnosis. Comparison to a plain chest radiograph taken a month earlier shows these to be new abnormalities.
A blood gas analysis was performed. This revealed an oxygen tension (PO2) of 6.93 kPa (52 mmHg) and carbon dioxide tension (PCO2) of 3.06 kPa (23 mmHg) on an inspired oxygen fraction of 0.21 (room air).
Task 2
What is the alveolar-arterial (A-a) gradient and arterial/alveolar (a/A) ratio? How would you interpret these figures?
Answer 2
The A-a gradient was 9.2 kPa (69 mmHg) and the a/A ratio was 0.43. The A-a gradient and a/A ratio reflect oxygenation and are unaffected by hypo- or hyperventilation, and hence demonstrate an intrapulmonary cause of hypoxaemia.
The arterial oxygen tension (PaO2)/inspiratory oxygen fraction (FiO2) ratio of 53/0.21 = 247 mmHg is supportive of a diagnosis of acute lung injury according to the 1994 American–European Consensus Conference Criteria:
-
Acute onset
-
Bilateral interstitial infiltrates
-
No evidence of elevated left atrial pressure
-
PaO2/FiO2 ratio of 201–300 mmHg
Task 3
Give a differential diagnosis.
Answer 3
Bacterial community-acquired pneumonia (including atypical organisms such as Legionella spp.), viral pneumonia, Pneumocystis jirovecii pneumonia, acute interstitial pneumonitis (Hamman–Rich syndrome), drug-induced respiratory disease (DIRD), cryptogenic organising pneumonia. Although left ventricular dysfunction and pulmonary oedema are common entities that must be excluded when evaluating acute lung injury there was no clinical supporting evidence of this. In these circumstances, opportunistic infections are common and actively need excluding.
The chest radiograph was reported as a patchy bilateral interstitial infiltrate. Given the association between thalidomide and venous thromboembolism, and the degree of hypoxaemia at presentation, a computerised tomographic pulmonary angiogram was performed with high resolution reconstructions. A representative image from this series is shown in figure 2.
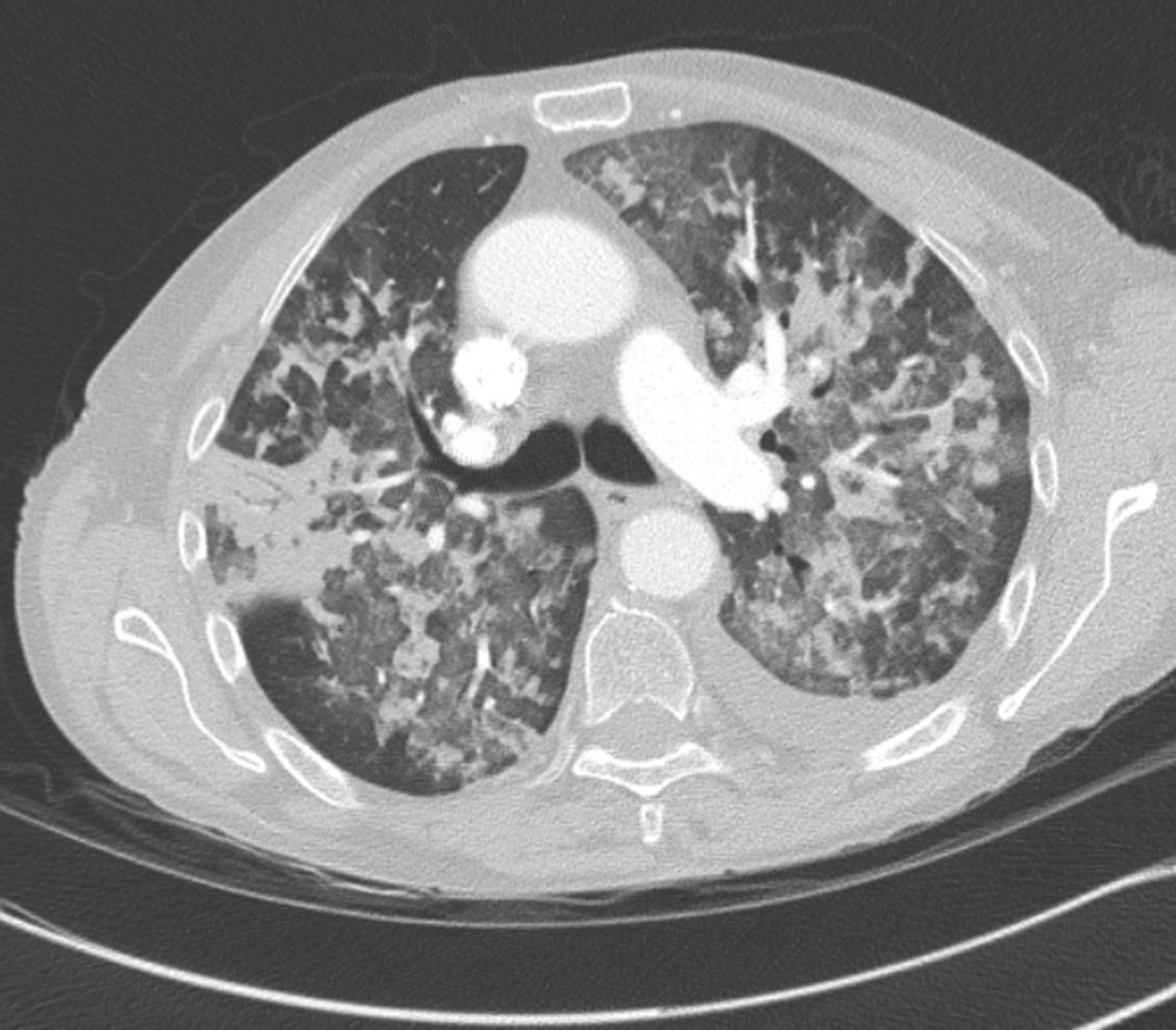
Computed tomographic pulmonary angiogram.
Task 4
Describe the abnormalities shown.
Answer 4
A bilateral, widespread, severe pulmonary parenchymal abnormality is seen. There is evidence of air trapping, together with areas of ground glass activity as well as more confluent density (consolidation) visible with air bronchograms demonstrated in the periphery of the right lung. There is a left-sided pleural effusion visible. Pulmonary embolus was not seen.
Task 5
What further investigations are needed?
Answer 5
The following further investigations are needed:
-
A pulmonary haemorrhage screen including autoantibodies and coagulation studies.
-
Infectious disease specimens to exclude infective causes.
-
Bronchoscopy with or without transbronchial lung biopsy or surgical lung biopsy depending on local expertise and presence of contraindications.
-
Full pulmonary physiology including lung volumes and diffusing capacity of the lung for CO (DLCO).
-
Echocardiography.
Phlebotomy revealed the prothrombin time, activated partial thromboplastin time, platelet and fibrinogen counts to be within the reference range. Autoimmune serology was unremarkable including negative dsDNA, anti-neutrophil cytoplasmic antibody, antinuclear antibody and Anti–glomerular base ment membrane antibodies. Cultures and antibody or immunohistochemistry testing of blood, urine, sputum, peritoneal dialysis fluid and faeces were all unremarkable. HIV antibodies were negative. Bronchoscopy was suggestive of pulmonary haemorrhage with blood seen throughout the visualised bronchial tree. No haemorrhage was seen in the nasopharynx or larynx. Bronchoalveolar lavage revealed large numbers of red cells and small numbers of polymorphs, bacterial and mycobacterial cultures showed no growth and immunofluorescence for P. jirovecii was negative. Cytological analysis of the bronchial washings revealed normal bronchial epithelial cells and haemosiderin-laden macrophages. Echocardiography showed moderately impaired systolic function and elevated right ventricular pressures. There was no evidence of valvular heart disease. Unfortunately, DLCO was not available during the acute illness.
The likely diagnosis was therefore drug induced respiratory disease (DIRD) manifesting as interstitial lung disease (DI-ILD).
Thalidomide was stopped within 24 h of admission, resulting in a subjective improvement within a further 24 h. Chest radiograph on day 3 of the admission was consistent with pneumonitis and a repeat on day 6 showed significant clearing which continued to improve until there was minimal evidence of any interstitial disease within 1 month (fig. 3). The patient was not re-challenged with thalidomide and transbronchial lung biopsy was not performed due to rapidly progressive hypoxaemia at the time of presentation and subsequent rapid improvement in condition after cessation of thalidomide. The patient was commenced on bortezomib.

{kind=link}
{kind=link}
{kind=link}
Chest radiograph on day 3 of admission
Discussion
While, for many, thalidomide remains synonymous with teratogenicity, increased understanding of its immunomodulatory, anti-cytokine and anti-angiogenic properties [1] have led to it being approved once more for use in certain well-defined situations and subject to careful surveillance. Efficacy in multiple myeloma is potentially mediated via direct inhibition of myeloma cell growth and survival, anti-angiogenesis, suppression of tumour necrosis factor α, inhibition of selected cell surface adhesion molecules that assist leukocyte migration, suppression of CD4:CD8 lymphocyte ratios and effects on interleukins and interferon-γ [2]. It is being increasingly used for both first-line and also as salvage therapy for multiple myeloma [3]. The common side effects of thalidomide are well documented. Apart from the severe teratogenicity, these include drowsiness, somnolence, sedation, peripheral neuropathy and thrombogenicity. Less commonly, thalidomide can result in nausea, dizziness and orthostatic hypotension, bradycardia and syncope, neutropenia, seizures, severe dermatological reactions, impaired wound healing and tumour lysis syndrome. To date, there have been only five reported cases of thalidomide-induced interstitial pneumonitis in multiple myeloma patients reported in the literature in English [3–7]. We present a case of thalidomide-induced pneumonitis and review the current literature. Clinicians, who may not be experienced in the use of thalidomide therapeutically, should be aware of the features of pulmonary toxicity.
Thalidomide-induced pneumonitis is a rare diagnosis, which prompted this review. A literature review using PubMed was undertaken using the search terms “thalidomide induced interstitial pneumonitis” and “thalidomide” and “myeloma” and “interstitial pneumonitis”. This revealed 49 papers, of which 10 were deemed relevant. Examining the references of these papers revealed a further 11. All but four were obtained in full. Two were unavailable in full text and two more were not written in English. The search was compared against a drug search on a website that provides updated information of drug induced respiratory disease (www.pneumotox.com) and revealed no additional papers. The diagnosis of drug-induced interstitial lung disease (DI-ILD) essentially rests on the temporal association between exposure to the drug and the development of pulmonary infiltrates, and the exclusion of other causes. The histopathological features of DI-ILD are generally consistent with, rather than suggestive of or specific to the drug aetiology. In view of the non-specific nature of pathological findings, the pursuit of tissue in DIRD often has an unfavourable risk/benefit analysis, as biopsy is not without hazard and the patients are by definition already compromised. Thus, the diagnosis of DI-ILD is mainly made by the meticulous exclusion of all other possible causes.
Three papers reviewed the indications, mechanisms and side effects of thalidomide in specific disease and interstitial pneumonitis was not quoted in any of these studies as an adverse effect of the drug [11–13]. Five studies reported cases of likely drug-induced interstitial pneumonitis while on thalidomide alone as treatment for multiple myeloma [3–7]. In these reports, the diagnosis of thalidomide-induced pneumonitis was presumed, as discussed above, alongside a corroborative history and by exclusion of other reasonable causes via a combination of computed tomography, negative cultures, normal echocardiography, bronchial biopsy (open lung biopsy not usually warranted [3]) and bronchiolar lavage (may show lymphocyte preponderance) [3]. All five patients showed improvement of symptoms and radiological signs after ceasing the drug. Two of these cases were re-challenged with thalidomide which resulted in recurrence of symptoms and signs [3, 6]. Three further papers reported cases of possible thalidomide-induced interstitial pneumonitis; however, patients were concurrently being treated with other agents (none of which was known to be associated with pneumonitis).
Interstitial-infiltrative lung disease is the most common pattern of drug-induced pulmonary injury and has been reported with over 380 drugs [10]. The mechanism for thalidomide-induced interstitial lung disease is unclear. There are a number of purported mechanisms for anti-neoplastic therapy induced lung toxicity, including oxidative effects, hyper- sensitivity and impairment of cell repair by agents blocking epidermal growth factor receptors [8]. The lymphocytic preponderance in broncholaveolar lavage (BAL) in interstitial pneumonitis supports a hypersensitivity mechanism, as does the recurrence of respiratory symptoms upon re-challenge with a smaller dose in one patient [6]. Sassaki et al. [14] suggest a genetic component by highlighting the possibility of preferential incidence of interstitial pneumonia in Japanese patients.
We report a further case of probable thalidomide-induced interstitial pneumonitis, on the basis that all other reasonable diagnoses and possible aetiologies were excluded. In addition, the rapid resolution following the cessation of thalidomide is in keeping with the aetiology. It was deemed unethical to re-challenge the patient with thalidomide as alternative therapies were available for her multiple myeloma.
Summary
Drug-induced pneumonitis is a rare complication of thalidomide therapy, however it should be considered in anyone recently commenced on thalidomide who presents with appropriate respiratory symptoms. It is a diagnosis of exclusion. Fortunately, the condition appeared to be completely reversible in this patient (both symptomatically and radiologically) upon ceasing the medication.
The Authors wish to highlight the excellent website www.pneumotox.com and its associated app for iOS. The site has collated information on DIRD since 1997 and is free to use.
Educational questions
Regarding druginduced respiratory disease (DIRD), answer the following true or false:
-
When seen in bronchoalveolar lavage of patients on amiodarone, foam cells are diagnostic for amiodarone pulmonary toxicity (APT)
-
Classical pulmonary fibrosis of a usual interstitial pneumonia pattern is seen in APT
-
Diffuse alveolar haemorrhage is characterised by a haemorrhagic return on broncholaveolar lavage
-
Idiosyncratic DIRD is uncommon, with most DIRD caused by prolonged dosing
-
Histopathological confirmation of DIRD is mandatory if a DIRD is to be reported to local pharmaceutical regulatory bodies.
Answers to educational questions
-
False. Foam cells, phospholipid laden macrophages, can be found in the BAL of patients on amiodarone without evidence of pulmonary toxicity.
-
True. APT has many radiological manifestations including UIP-pattern fibrosis, pulmonary nodules, ground glass opacities or even isolated pleural effusion. Pulmonary infiltrates often have high attenuation on HRCT and it is postulated that this relates to iodine content.
-
True. This helps distinguish from other conditions that give rise to blood in the airways (e.g. unrecognised endobronchial haemorragic tumours).
-
False. Many drug reactions are idiosyncratic and occur unpredictably regardless of dose or duration of treatment.
-
False. Whilst the precise details of pharmacovigilance programmes vary from country to country, many nations have such a scheme e.g. the Yellow Card scheme in the UK (www.yellowcard.mhra.gov.uk), the European Medicines Agency's EudraVigilance scheme (www.eudravigilance.ema.europa.eu) to which clinicians can contribute suspected Adverse Drug Reactions (ADRs). Tissue confirmation of DIRD is often not feasible (due to illness severity or comorbidity) or when available, findings may be non-specific. A healthy level of suspicion is needed, and clinicians should be aware of their duty to report potential ADRs.
Footnotes
Statement of Interest
None declared.
- ©ERS 2014
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










