





Figures
- Figure 1
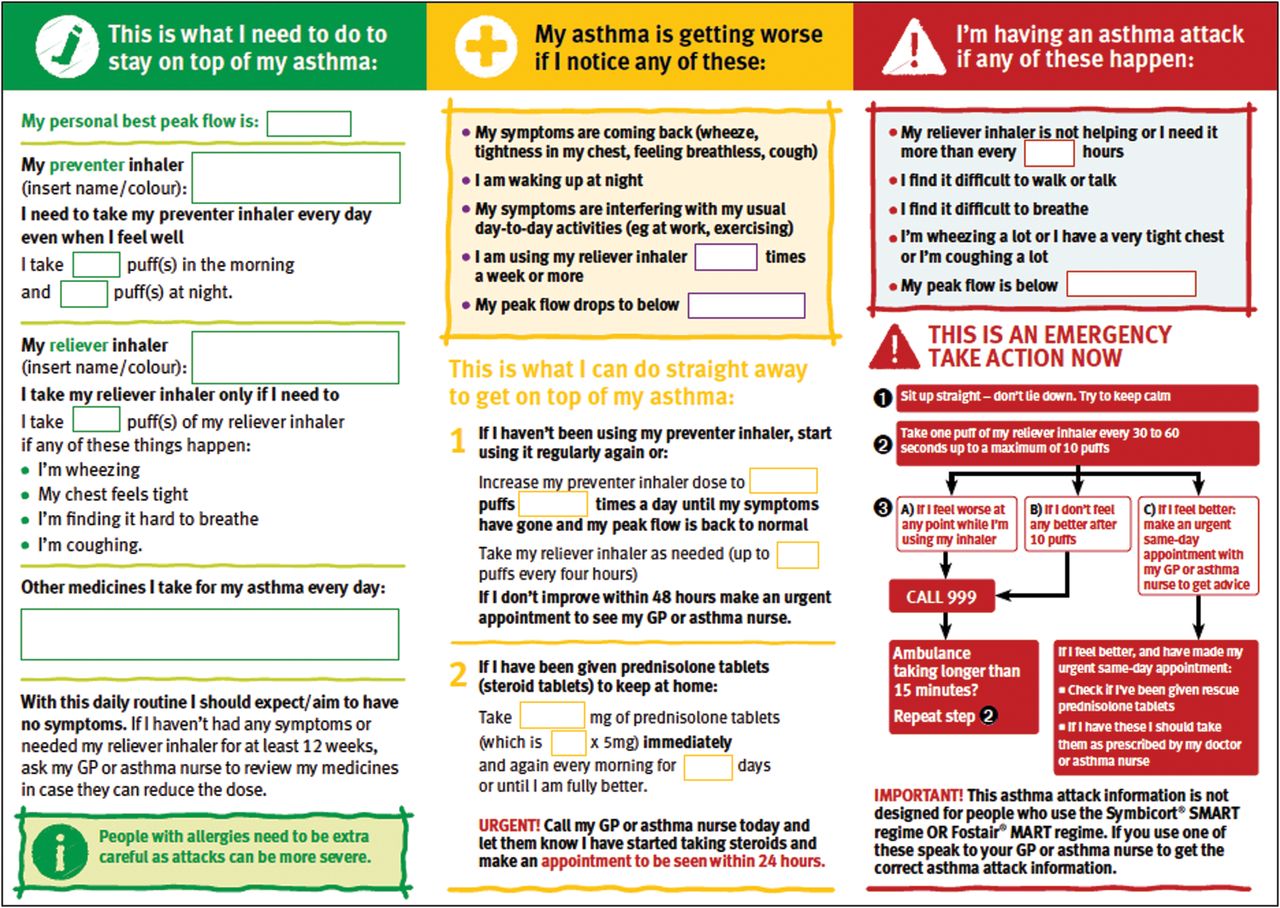
Asthma action plan. An example of a asthma self-management tool. Reproduced with permission from Asthma UK. Available from www.asthma.org.uk/advice-asthma-action-plan.
{kind=link}
Tables
- Table 1
Strategies for cultural tailoring that have been used in effective interventions
Translation of materials into community languages with ethnically appropriate pictures.
Asthma educators fluent in community languages.
Identifying culturally appropriate support agencies within the local community.
Inclusion of culturally specific beliefs and practices.
Reference to culturally appropriate role models.
Involvement of a local community health worker to support clinical teams.
Reproduced from [8] with permission from the publisher.
- Table 2
Summary of the key components of a written personalised asthma action plan
Component of an action plan Result Practical considerations Format of action points Symptom versus peak flow triggered Similar effect Asthma UK personalised asthma action plans include both symptom triggers and peak flow levels at which action should be taken. Standard written instructions Consistently beneficial Traffic light configuration Not clearly better than standard instructions Number of action points 2–3 action points Consistently beneficial Three commonly used action points are:Peak flow <80% best: increase inhaled steroidsPeak flow <60% best: commence oral steroids and seek medical advicePeak flow <40% best: seek urgent medical advice. 4 action points Not clearly better than 2–3 points Peak flow levels Based on percentage personal best peak flow Consistently beneficial Personal best should be assessed once treatment has been optimised and peak flows are stable. Best peak flow should be updated every few years in adults, and, if a peak flow meter is being used, more frequently in growing children. Based on percentage predicted peak flow Not consistently better than usual care Treatment instructions Individualised using inhaled and oral steroids Consistently beneficial Patients may safely hold an emergency supply of prednisolone tablets for use if their symptoms continue to deteriorate and/or if their peak flow falls to 60% of their best. Individualised using oral steroids only Insufficient data to evaluate Increasing inhaled steroids is ineffective if patients are already taking moderate or high doses (≥400 µg daily) and these patients should be advised to move straight to the oral steroid step. Individualised using inhaled steroids Insufficient data to evaluate Those on low doses (e.g. 200 µg) of inhaled steroids may be advised to increase the dose substantially (e.g. to 1200 µg daily) at the onset of deterioration. Patients who have stopped medication should be reminded to restart their inhaled steroids. Reproduced from [8] with permission from the publisher.
- Table 3
Opportunities to review, refine and reinforce self-management
A hospital admission represents a window of opportunity to review self-management skills. No patient should leave hospital without a written personalised asthma action plan.
An acute consultation offers the opportunity to determine what action the patient has already taken to deal with the asthma attack. Their self-management strategy may be reinforced or refined and the need for consolidation at a routine follow-up considered.
A routine consultation should include a review of whether the action plan has been used, and if the actions need refining in the light of experience.
A consultation for an upper respiratory tract infection or other known triggers is an opportunity to rehearse with the patient their self-management in the event of their asthma deteriorating.
Collection of a prescription at a pharmacy is an opportunity to reinforce understanding of the role of medications and check inhaler technique.
A request for hay fever treatment is an opportunity to ask about asthma symptoms and reinforce the action that should be taken if symptoms increase.
Reproduced from [8] with permission from the publisher.










