





Abstract
Physiology masterclass: respiratory physiology of pregnancy http://ow.ly/UvYXt
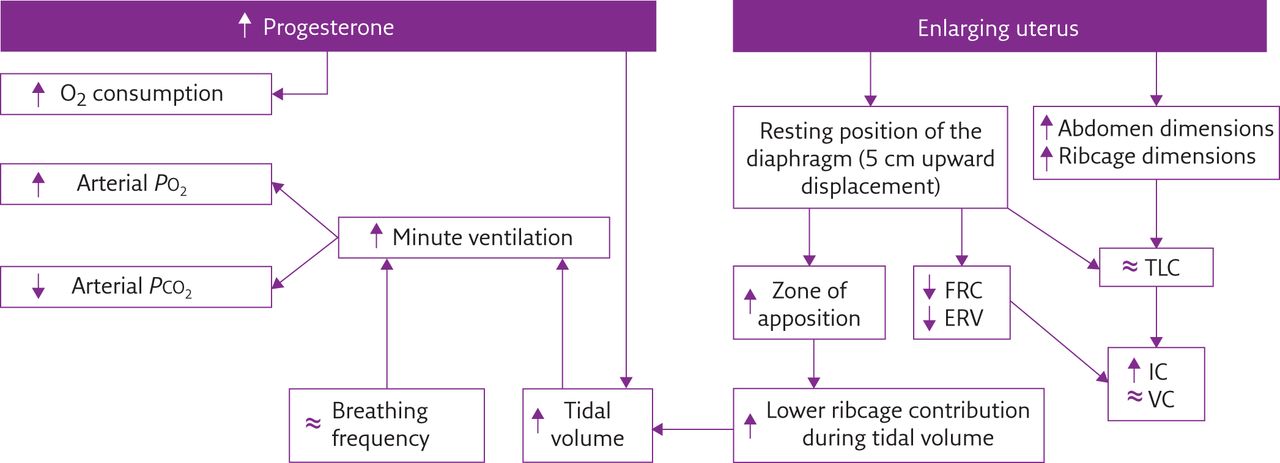
During healthy pregnancy, pulmonary function, ventilatory pattern and gas exchange are affected through both biochemical and mechanical pathways, as summarised in figure 1.
{kind=link}
Flow diagram summarising the most important effects of biochemical (left) and mechanical (right) pregnancy-induced factors on pulmonary function, ventilatory pattern and gas exchange. PO2: oxygen tension; PCO2: carbon dioxide tension; FRC: functional residual capacity; ERV: expiratory reserve volume; TLC: total lung capacity; IC: inspiratory capacity; VC: vital capacity; ↑: increased; ↓: decreased; ≈: no change.
Chemical/hormonal changes
During pregnancy, the physiological alteration of hormonal patterns is the main cause of ventilatory changes in respiratory function.
Progesterone
Progesterone gradually increases during the course of pregnancy, from 25 ng⋅mL−1 at 6 weeks’ to 150 ng⋅mL−1 at 37 weeks’ gestation [1–5]. Progesterone acts as trigger of the primary respiratory centre by increasing the sensitivity of the respiratory centre to carbon dioxide, as indicated by the steeper slope of the ventilation curve in response to alveolar carbon dioxide changes [6]. Progesterone alters the smooth muscle tone of the airways resulting in a bronchodilator effect. It also mediates hyperaemia and oedema of mucosal surfaces, causing nasal congestion.
Oestrogen
The circulating levels of oestrogen increase during pregnancy, before or in parallel to those of progesterone. Oestrogen is a mediator of progesterone receptors. It increases the number and the sensitivity of progesterone receptors within the hypothalamus and medulla, the central neuronal respiratory-related areas [1].
Prostaglandins
Prostaglandins stimulate uterine smooth muscle during labour and are present during all three trimesters of pregnancy. Prostaglandin F2α increases airway resistance by bronchial smooth muscle constriction, whereas a bronchodilator effect can be a consequence of prostaglandins E1 and E2 [1].
Mechanical effects
The progressive uterine distension is the major cause of lung volume and chest wall changes during pregnancy, which comprise elevation of the diaphragm and altered thoracic configuration [1–3]. The enlarging uterus increases the end-expiratory abdominal (gastric) pressure (Pga), thereby displacing the diaphragm upwards, with two consequences [2]. First, the negative pleural pressure (oesophageal pressure (Poes)) increases, leading to an earlier closure of the small airways with consequent reduction of functional residual capacity (FRC) and expiratory reserve volume (ERV) [1, 3, 4, 7]. Secondly, the chest height becomes shorter, but the other thoracic dimensions increase in order to maintain constant total lung capacity (TLC) [1, 2, 7].
Lung volumes, spirometry and airway function
Throughout pregnancy, spirometry remains within normal limits, with forced vital capacity (FVC) [1, 3–5, 7–9], forced expiratory volume in 1 s (FEV1) [1, 4, 5, 7, 9] and peak expiratory flow [4, 7–9] not changing or modestly increasing with unaltered FEV1/FVC index [1, 4, 5, 7, 9].
Conversely, lung volumes undergo major changes: ERV gradually decreases during the second half of pregnancy (reduction of 8–40% at term) because residual volume reduces (by 7–22%). FRC then decreases (by 9.5–25%) while inspiratory capacity increases at the same rate in order to maintain stable TLC [1, 3, 4, 7].
Respiratory resistance increases while respiratory conductance decreases during pregnancy. Total pulmonary and airways resistances tend to decrease in late pregnancy as a consequence of hormonally induced relaxation of tracheobronchial tree smooth muscles [1, 4, 8]. Pulmonary static and dynamic compliance, diffusing capacity and static lung recoil pressure do not change during pregnancy [1, 2, 4, 7]. Respiratory function does not differ between singleton and twin pregnancies [7].
Chest wall geometry and displacement
The pregnancy-induced reduction of FRC is accompanied not only by abdominal enlargement but also by ribcage dimension increases. The ribcage expands, as its transversal diameter and the lower thoracic perimeter increase in the third trimester compared with postpartum. The average subcostal angle of the ribs at the xiphoidal level increases from 68.5° at the beginning of pregnancy to 103.5° at term [1–3].
Such ribcage dimension changes could be a consequence of fatty tissue and fluid accumulation, particularly blood, since pulmonary blood volume is often increased in pregnancy. However, it seems more likely to be a compensation of the shortening of the thorax due to the upward movement of the diaphragm, in order to guarantee space to the lung and preserve TLC.
Chest wall compliance decreases in late pregnancy due to the increased abdominal content [10].
Breathing pattern at rest
Minute ventilation (V′E) starts to increase significantly (by up to 48%) during the first trimester of gestation, due to higher tidal volume (VT) with unchanged respiratory rate. This ventilatory pattern is then maintained throughout the course of pregnancy [1–3, 5, 8].
Both VT/inspiratory time ratio and mouth occlusion pressure at 100 ms increase during pregnancy, indicating respectively that the ventilatory and inspiratory drives augment [2, 8].
The increased VT in pregnancy is achieved mainly by an improved displacement of the ribcage with no consistent changes in the abdominal contribution measured with magnetometers [2, 3].
Respiratory muscles
Maximal inspiratory and expiratory pressures do not change during pregnancy or after delivery indicating that, although there is alteration of chest wall geometry, the respiratory muscle strength is preserved [2–4, 11].
With pregnancy progression, the resting position of the diaphragm moves 5 cm upward with the increasing uterus size, as shown by chest radiograph measurement [1, 2, 12]. This causes the following changes to the diaphragm: its capability to generate tension increases secondary to muscle fibre lengthening; its area of apposition to the lower ribcage increases; and its radius of curvature increases, due to the progressive enlargement of the lower ribcage to give space to the lungs. In addition, the upward movement of the diaphragm causes FRC decrease.
The inspiratory movements of the diaphragm are similar or become even broader than postpartum [1, 12], and trans-diaphragmatic pressure swings during tidal breathing do not change [2]. The diaphragmatic work may increase as a consequence to contract against higher load represented by higher end-expiratory Pga and enlarged gravid uterus. This hypothesis is supported by the tension time index of the diaphragm, which falls after delivery [2].
During pregnancy, chest wall expansion is shifted toward the ribcage because of an enhanced coupling between abdominal pressure and the lower ribcage [2, 3]. Thanks to the increased area of apposition, in fact, the abdominal pressure generated by the contraction of the diaphragm acts mainly on the lower ribs, thereby elevating and expanding the ribcage where the diaphragm is apposed.
Two possible respiratory muscle strategies can be considered during pregnancy. 1) Higher inspiratory intercostal and accessory muscle recruitment, since the increased thoracic volume displacement and pleural pressure swings could also be a consequence of their enhanced action [2, 3]. 2) Similar relative contribution between the diaphragm and the inspiratory intercostal muscles, since the slope of the Pga versus Poes curve remains constant [2, 3].
The progressive increment of the anterior abdominal dimension leads to morphological adaptation of the abdominal muscles by lengthening their fibres up to 115%, changing their line of action, altering their angle of insertion and reducing their thickness. The consequences are compromised functional ability, poor torque production and reduced ability to stabilise the pelvis against resistance. The latter may be implicated in back pain during pregnancy [13, 14].
Oxygen consumption, arterial blood gases and acid–base status
Oxygen consumption and basal metabolic rate increase (by up to 21% and 14%, respectively), but to a lesser extent than ventilatory augmentation [1, 5]. Pregnancy-induced reduction in FRC combined with a rise in oxygen consumption lowers the oxygen reserve of the mother.
As a consequence of V′E increment, alveolar and arterial carbon dioxide tension (PCO2) levels decrease to plateaux around 27 and 32 mmHg, respectively [1, 4, 5]. During labour, arterial PCO2 further decreases with each contraction, while at full dilatation it decreases even between contractions [1].
Following hyperventilation and reduced levels of PCO2, arterial oxygen tension increases, reaching 106–108 mmHg and 101–104 mmHg in the first and third trimesters, respectively [1].
Despite hyperventilation and respiratory alkalosis, blood pH remains almost constant at slightly alkalotic values (7.40–7.47), thanks to renal compensation by increasing the excretion of bicarbonate [1, 4, 5].
Dyspnoea
Dyspnoea or breathlessness is commonly reported by 70% of healthy pregnant women during their daily living activities, starting from the very first trimester of gestation. Such an early time of onset excludes the pregnancy-induced mechanical changes from playing a role in the genesis of the symptoms [1]. Possible explanations could be: 1) an increased awareness of the new sensation of the physiological hyperventilation associated with pregnancy; 2) an increased central perception of respiratory discomfort with increasing V′E; or 3) a combination of these two.
Recently, pregnancy-induced hyperventilation has been demonstrated to be the result of complex interactions between changes in chemo-reflex drives, acid–base balance, metabolic rate and cerebral blood flow [5]. It is therefore a difficult challenge for the caregiver to distinguish between physiological and pathophysiological origins of dyspnoea.
Exercise
Pregnant women preserve their aerobic working capacity even in late gestation. The physiological response to incremental exercise in healthy pregnant women consists of augmentation of both V′E and oxygen consumption, with higher ventilatory equivalent (i.e. V′E/oxygen consumption) [1, 4].
Hyperventilation occurs thanks to the recruitment of resting inspiratory capacity combined with pregnancy-induced bronchodilation, allowing VT to increase in order to meet the metabolic demands. Inspiratory capacity is recruited thanks to stable TLC and pre-exercise end-expiratory lung volume reduction. Because ERV is reduced, end-expiratory lung volume does not further decrease during exercise to avoid the mechanical disadvantage of the lower portion of the pressure–volume curve of the respiratory system.
The ratio of the contractile effort of the respiratory muscles (tidal Poes/maximal inspiratory Poes) to the thoracic volume displacement (VT/vital capacity), being an index of neuromechanical (un)coupling of the respiratory system, does not change with increasing exercise. Pregnancy therefore does not influence the symptom-limited perceptual reasons to stop exercise and the increased breathlessness is a normal consequence of the increment of both V′E and work of breathing [4].
Pregnancy during disease
In addition to the biochemical and mechanical factors, many illnesses produce significant negative effects on respiratory maternal (and fetal) outcomes. Table 1 summarises the principal features to consider when treating unhealthy pregnant women.
Principal features to consider when treating unhealthy pregnant women
Footnotes
Conflict of interest None declared.
- ©ERS 2015
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










