





Abstract
Case report: An asymptomatic man undergoes a chest radiograph http://ow.ly/4nmyfG
Case history
An asymptomatic 45-year-old man who is a non-smoker with an unremarkable personal medical history underwent a chest radiograph (figure 1) during a medical examination prior to the issuance of a work card.
Task 1
Describe the radiographical findings.
What is your differential diagnosis?
What investigation would be helpful?

Chest radiograph.
Answer 1
The chest radiograph shows bilateral, symmetrical hilum enlargement and scattered small nodules mainly in the upper lung fields.
Differential diagnosis would be sarcoidosis/lymphoma.
Useful investigations would be: clinical examination; blood tests, including serum calcium and angiotensin-converting enzyme; 24-h urine calcium test; pulmonary function tests, such as static volumes, flow–volume curve and lung diffusion capacity; chest computed tomography (CT); and flexible bronchoscopy.
The clinical examination was normal with no abnormal findings on chest auscultation and no palpable peripheral lymph nodes or skin lesions. The patient’s pulse oximetry was 97% on room air with no change during the 6-min walk test. Blood pressure was 120/75 mmHg, and pulmonary artery systolic pressure was 20 mmHg with cardiac ultrasound.
Laboratory testing was remarkable for increased levels of serum angiotensin converting enzyme (86.4 U⋅L−1; normal range 8.0–42.0 U⋅L−1) and 24-h urine calcium (373 mg; normal range 100–300 mg). Serum calcium was within the normal range (9.3 mg⋅dL−1). A tuberculin skin test (Mantoux) was negative with a diameter of induration of 0 mm.
Pulmonary function tests (static and dynamic volumes, flow–volume curve and lung diffusion capacity) were within the predictive values. Vital capacity: 4.87 L (92%); forced expiratory volume in 1 s (FEV1): 3.97 L (97%); forced vital capacity (FVC): 4.87 L (96%); FEV1/FVC ratio: 82% (103%); single-breath diffusing capacity of the lung for carbon monoxide (DLCO): 9.09 (nmol⋅min−1⋅kPa−1) (82.65%); and corrected DLCO by alveolar ventilation: 1.45 nmol⋅min−1⋅kPa−1⋅L−1 (96.34%).
A chest CT (figure 2) and flexible bronchoscopy (figure 3) were performed.
Task 2
Describe the following.
The chest CT findings
The flexible bronchoscopy findings

Chest CT.
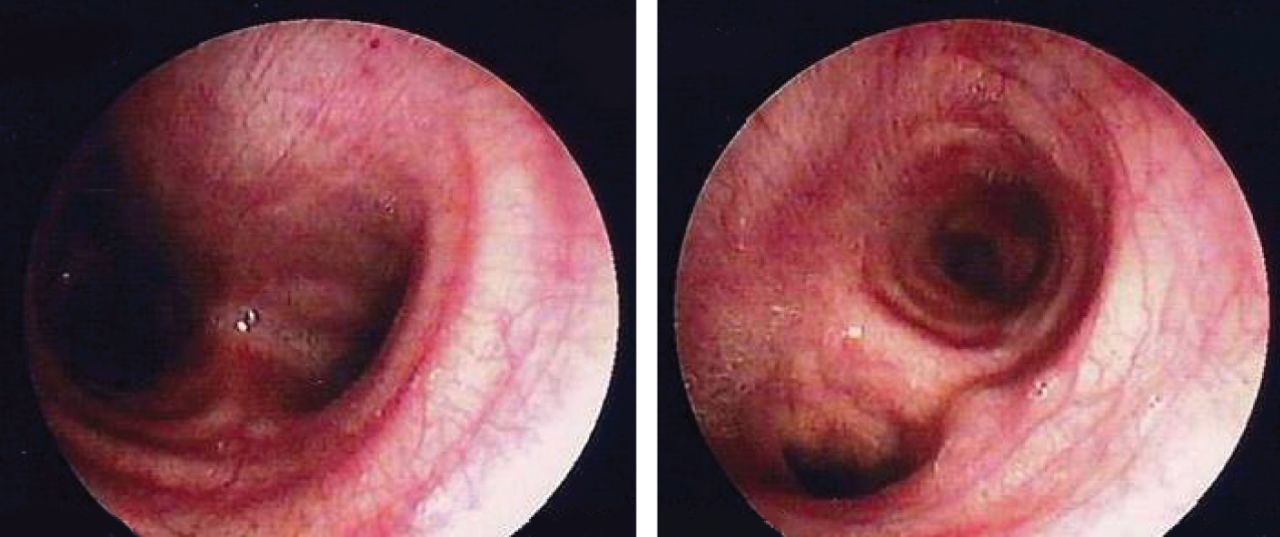
Flexible bronchoscopy.
Answer 2
The chest CT shows multiple, bilateral, small nodules, a few millimetres in diameter, along the bronchoalveolar bunds (perilymphatic distribution), especially in the upper lobes. Larger nodules (approximately 1 cm in diameter) can also be seen. Multiple enlarged lymph nodes are present in both hila.
The flexible bronchoscopy shows diffuse redness of the bronchial mucosa dotted with haemorrhagic foci and intense vascularisation.
Task 3
What bronchoscopic sampling techniques would you perform for a histological diagnosis of sarcoidosis?
Answer 3
Transbronchial lung biopsy (TBLB), endobronchial biopsy (EBB) or a combination of both with or without transbronchial needle aspiration (TBNA).
An EBB was performed (figure 4).
Task 4
Describe the EBB.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
EBB.
Answer 4
The EBB showed two well-formed, non-caseating epithelioid (sarcoid) granulomas in the lamina propria of the mucosa. Special stains for fungus and mycobacteria were negative.
Diagnosis: stage II sarcoidosis
The patient was given steroids to treat the hypercalciuria. In the follow-up 24-h urine calcium test, calcium levels were within the normal range, and the abnormal findings on the chest CT were diminished.
Discussion
This is a case of asymptomatic stage II sarcoidosis with bronchial involvement that was diagnosed histologically with EBB.
Bronchial involvement in sarcoidosis was first described by Renedict and Castleman in 1941 [1]. Today, it is well established that sarcoidosis can affect the entire respiratory tree, from the nose to the terminal bronchioles. Bronchial involvement has been reported in 55% [2] and 70.5% [3] of sarcoidosis cases and may cause obstructive disorders of both the small and large bronchi [4] with respiratory symptoms and an increased risk of mortality [5].
The inflammation of the bronchial mucosa observed in our case is one of the abnormal bronchoscopic findings observed in patients with sarcoidosis. A retrospective study [2], including a total of 150 patients with sarcoidosis, described the following endoscopic findings: normal (70 patients), erythema (28 patients), plaque (12 patients), nodule (12 patients) and cobblestoning (28 patients). In a prospective study, including 101 patients with sarcoidosis, the bronchoscopic abnormalities found were bronchostenosis (26% of patients), mucosal nodularity (64%), hypervascularity (38%) and mucosal oedema (55%) [6]. The bronchoscopic findings did not correlate to the radiographic stage of the disease, except for the nodular mucosal appearance [6].
In the presenting case, sarcoidosis was diagnosed with EBB. EBB together with TBL and TBNA in patients with enlarged lymph nodes in the mediastinum and hilar regions are the basic bronchoscopic techniques used to obtain biopsy material for the histological diagnosis of sarcoidosis [7, 8].
Lung parenchyma involvement in over 90% of sarcoidosis cases has established TBLB as the standard method for making the histological diagnosis of sarcoidosis. The diagnostic yield from TBLB ranges from 50% to 80%, depending on the extent of parenchymal involvement [3]. However, TBLB may occasionally cause serious complications, such as a pneumothorax or pulmonary haemorrhage [2].
The diagnostic yield from EBB is also high, ranging from 45% to over 70% of patients [6–10] and the diagnostic sensitivity of EBB correlates to the abnormal bronchial mucosa appearance. Patients with erythematous airways (as in our case), thickening of the mucosa or both, are seven-times more likely to have positive EBB compared with patients with normal airways [3]. The diagnostic yield of positive EBB has been described in 91% of sarcoidosis cases with intrabronchial stenosis, nodular mucosa appearance and increased vascularisation, compared with 37% of cases with the absence of these bronchial findings [6]. EBB may be positive even in bronchoscopically normal bronchial mucosa (30% to 50% of cases) [2, 3, 7].
Τhe diagnostic yield of EBB does not correlate with the patient’s sex, symptoms, radiographic stage of disease, pulmonary function tests or serum markers (angiotensin converting enzyme, erythrocyte sedimentation rate, C-reactive protein) [2, 3]. However, it has previously been shown that patients with positive EBB for sarcoidosis tend to have a worse clinical course with more patients requiring treatment with systemic steroids [10].
Studies have shown that EBB, in combination with TBLB and TBNA, significantly increases the diagnostic yield of bronchoscopy in sarcoidosis compared with the techniques when used individually. Shorr et al. [3] showed that the addition of EBB to TBLB increased the diagnostic yield of bronchoscopy by 20.6%. Armstrong et al. [6] reported that the combination of both techniques (EBB and TBLB) increased the individual diagnostic sensitivities from 57% for EBB and 73% for TBLB to 88% of cases when the two techniques were used together. In a prospective study including 151 patients with sarcoidosis, Gupta et al. [11] found that the diagnostic yield was 81.4% for EBB+TBLB, 73.7% for TBLB+TBNA, 62.9% for TBNA+EBB, 86.9% for TBLB+EBB+TBNA and 86.4% for TBLB+EBB+endobronchial ultrasound-TBNA (EBUS-TBNA). The diagnostic yield of the individual techniques was 68.7% for TBLB, 49.6% for EBB, 22.43% for the conventional TBNA and 57.1% for EBUS-TBNA.
The diagnostic yield of the different combinations of bronchoscopy sampling techniques differs in accordance to the disease stage. A study of 74 patients with suspected stage I–III sarcoidosis found that the combination of EBB+TBLB+TBNA was positive in 91% of patients with stage I sarcoidosis and 88% of patients with stage II sarcoidosis. The diagnostic yield for the combination of EBB+TBLB was 100% in patients with stage III sarcoidosis [12].
Although the combination of bronchoscopic biopsy techniques has a greater diagnostic sensitivity compared with the individual techniques, it increases the complexity of the bronchoscopy procedure and the risk for the patient.
In addition to its optimal diagnostic sensitivity, EBB is a safe technique with minor or no complications [2, 3, 6, 9, 12], as was observed in our case.
The high diagnostic yield and safety of EBB supports its use as a method of choice for histological diagnosis of sarcoidosis in cases with visual abnormalities in the bronchial tree, as in the presenting case.
Conclusions
This is a case of asymptomatic stage II sarcoidosis with bronchial involvement that was diagnosed histologically with an endobronchial biopsy. EBB is a safe technique with a high diagnostic yield in sarcoidosis, especially in cases with abnormal appearance of the bronchial mucosa. In combination with TBLB and TBNA (in cases of enlarged lymph nodes), EBB significantly improves the diagnostic yield of bronchoscopy in sarcoidosis. However, the presenting case supports the observation that, in patients with suspected sarcoidosis and visual abnormalities in the bronchial tree, EBB is likely to result in a conclusive specimen.
Footnotes
Conflict of interest None declared.
- ©ERS 2016
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










