





Abstract
Cognitive impairment is highly prevalent in patients with COPD and demonstrates multiple detrimental effects on many aspects of patient state and therapeutic outcomes. It is attributed to several overlapping pathophysiological factors, with the most common being the low level of oxygen saturation due to respiratory insufficiency. Despite the impact of cognitive impairment on clinical outcomes, the screening for coexisting cognitive deficits which may interfere with the successful progress of respiratory treatment is yet neglected. There is a special consideration that cognitive deficits should be taken into account when developing respiratory therapy plans. Cognitively impaired patients are likely to require more support and have need of an individualised respiratory care plan which can also be beneficial for their cognitive deficits. Pulmonary rehabilitation as a multidisciplinary approach could be prioritised for COPD patients with cognitive impairment.
To illustrate the common signs of cognitive impairment and define potential associations between lung and cognitive dysfunction.
To illustrate the potential influence of cognitive deficits on the optimal progress of respiratory therapy.
To illustrate the importance of cognitive evaluation as part of a comprehensive clinical assessment for patients suspected of suffering cognitive impairment.
Abstract
Cognitive impairment in COPD may affect respiratory treatment and should be considered in therapeutic strategy http://ow.ly/aK3s309RiS9
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by persistent respiratory symptoms and airflow limitation [1]. It is a progressive condition which is associated with pulmonary and systemic inflammation with numerous extrapulmonary consequences such as cognitive deterioration [2]. In particular, the brain can be vulnerable to the systemic effects of COPD as several features of the disease may increase the risk for impaired cognitive function and also contribute to cognitive decline across the progress of disease severity and the ageing process [3]. Cognitive impairment is characterised by several common signs (table 1) and seems to have detrimental effects on many aspects of patient function, health status and quality of life, as well as being related to lower adherence to medical treatment and increased rates of hospitalisation and mortality in COPD [4–6].
Signs of cognitive impairment: several symptoms may imply a cognitive dysfunction in patients with chronic obstructive pulmonary disease (COPD)
A growing amount of evidence has demonstrated an association between cognitive impairment, a pathological condition that acts as a barrier to cognition, and COPD manifestation [7, 8]. Indeed, the prevalence estimates of cognitive impairment are increased in patients with COPD, indicating lung dysfunction as a risk factor for cognitive impairment even when data are adjusted for age, sex, smoking habits and education level [9]. The degree of prevalence ranges from 10 to 61% amongst COPD patients and seems to depend on the study population and the method of neuropsychological assessment [7, 10]. The prevalence amongst older adults in the general population, as assessed in community samples, seems to be lower with between 3 and 20% having cognitive deficits depending on the way that cognitive function is assessed [11, 12]. On average, 36% of patients with COPD will present with incidents of cognitive impairment [8], whereas only 12% of individuals amongst the general population [13] will be cognitively impaired. These higher prevalence estimates for cognitive impairment in COPD indicate an association between impaired lung-function and brain pathology that cannot be disputed. Nevertheless, defining all the complex pathophysiological mechanisms in COPD that may interfere with brain function is really challenging. Lung dysfunction and disease severity in COPD do not fully explain the development of cognitive impairment in COPD patients. Moreover, the typical profile of patients with COPD includes numerous of comorbidities, such as cardiovascular disease or diabetes or a combination thereof (so called “multi-morbidity”), which may contribute to the genesis of cognitive impairment to a varying extent [14, 15]. In addition, the impact of disease severity (including comorbidities or other risk factors) can affect different domains of cognition variably, with some being unaffected while others present substantial impairment.
Cognition and neuropsychological domains
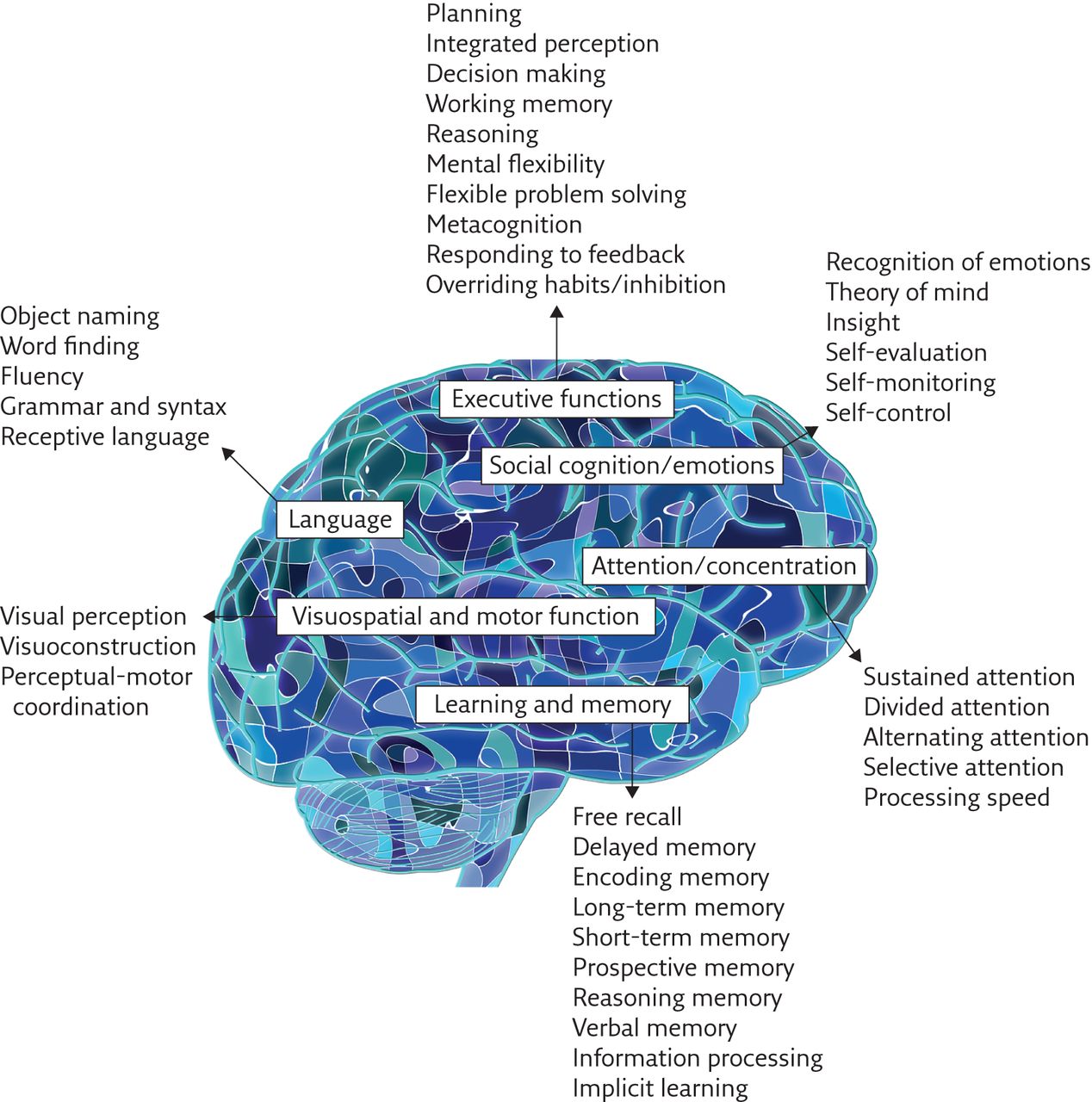
The word “cognition” is of Latin derivation but originally comes from the Greek verb “gignosko” which means to recognise, perceive and know [16]. Specifically, cognition is the mental action or intellectual process of acquiring, understanding and using knowledge or information, through thinking, experience and the senses, by which human behaviour can be adapted to new situations and/or preferences changed [17, 18]. Cognition involves different cognitive processes which can be divided into six basic neuropsychological domains including learning and memory, visuospatial and motor function, attention/concentration, language, social cognition/emotions and executive functions (figure 1). Each domain contains specific functions which provide individuals with basic and more complex capabilities that determine personal intellectual skills and knowledge (figure 1) [18, 19].
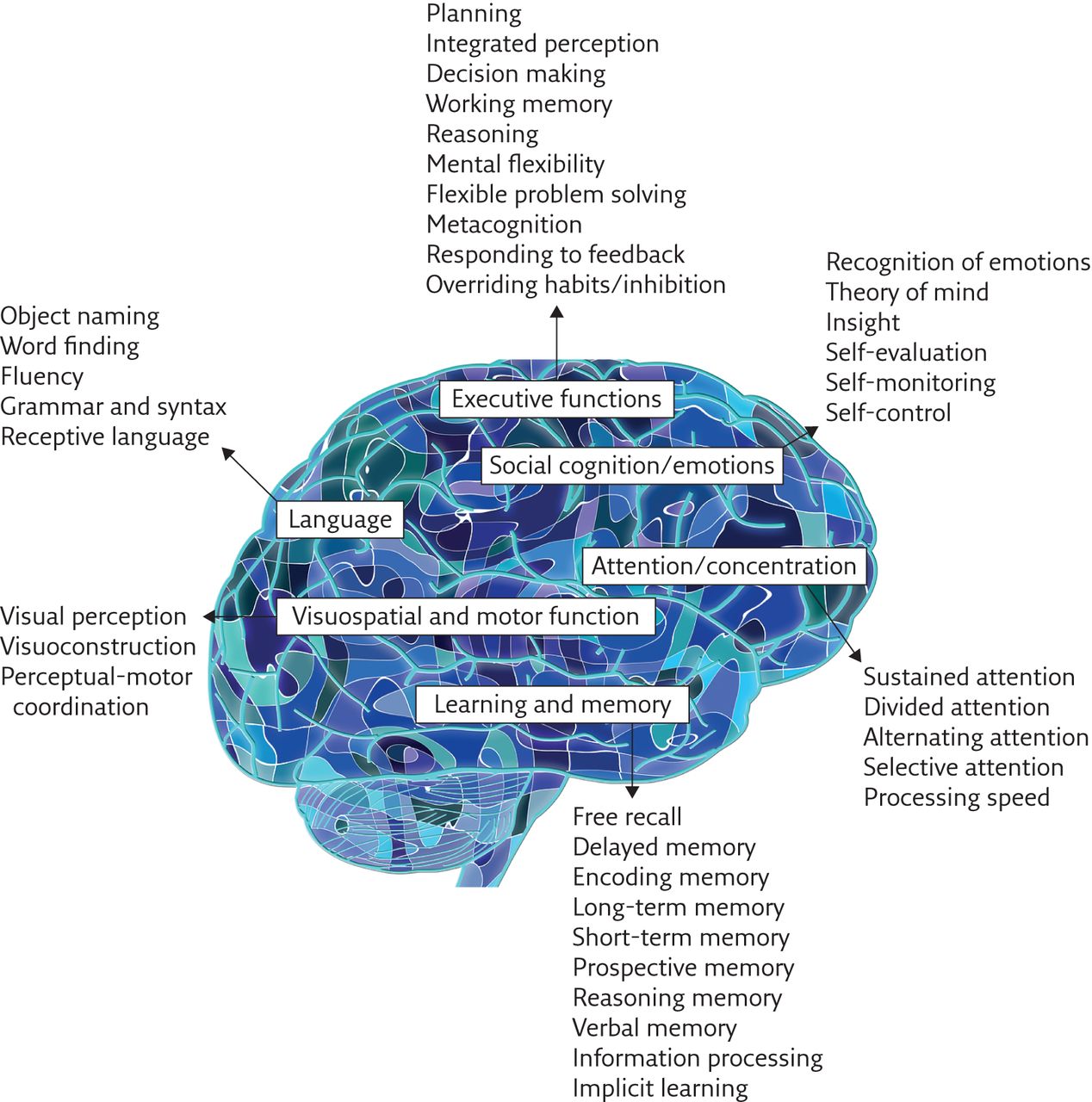
Major domains of cognitive function.
Assessment of cognitive function
Cognitive function can initially be assessed without complex procedures or sophisticated equipment. Using appropriately validated screening tests for cognitive impairment, healthcare professionals may obtain a first overview of the cognitive status of a patient, as inferred from the relationship of the patient’s score to reference norms. Patients with very low screening scores can be considered as cognitively impaired and may therefore be referred to a mental health clinic, whereas patients with borderline scores may be referred for further comprehensive assessment by a specialist with expertise in evaluating mental function [20]. A borderline score may identify patients in the first stages of cognitive decline, which is defined as mild cognitive impairment (MCI), differentiating patients who have worse cognitive deficits than those expected in normal ageing but not severe enough to warrant a diagnosis of dementia [21].
A wide range of tools has been developed for screening cognitive function. Some of them are freely available whereas for others a licence is required. These tools can be described as comprehensive when they cover each of the primary cognitive domains in cognitive function (figure 1) or non-comprehensive when they identify clinically significant levels of cognitive impairment across a limited spectrum of cognitive abilities [22]. The duration of screening ranges from a few minutes up to several hours in the case of a formal neuropsychological assessment [20]. Most of the tests designed for use in prompt cognitive evaluation during the daily clinical routine take from 4 to 12 min to be completed. The most widely-used tests which cover multiple cognitive domains are the Mini Mental State Examination (MMSE) [23], the Addenbrooke’s Cognitive Examination (ACE) [24, 25], the Montreal Cognitive Assessment (MoCA) [26], the Clock Drawing Test (CDT) [27] and the Mini-Cog test [28]. In addition, telephone interviews have been developed for use in distance situations where in-person cognitive screening is impractical or impossible [29, 30]. These tests have good diagnostic accuracy [31] and can provide healthcare professionals with a prompt overview of patients' cognitive status when cognitive impairment is suspected.
Lung impairment and cognitive function
Cognitive function refers to the general competence of cognitive abilities that can be affected by COPD pathophysiology. The relationship between lung impairment and cognitive function decline has already been confirmed in numerous studies, which have demonstrated the particularly negative impact of inadequate respiratory function on cognitive domains such as memory and learning, attention, psychomotor speed, visuospatial abilities, executive functions, and language skills [32–34]. These negative consequences on cognitive function are a result of complex interactions amongst COPD pathophysiological, genetic and environmental factors.
The most obvious independent risk factor for cognitive impairment in patients with COPD is reduced oxygen availability as a result of lung dysfunction. From a physiological point of view it is reasonable to consider that the brain, which has almost the highest oxygen demand of any organ in the human body (the biggest oxygen consumers are the liver (20.4%), the brain (18.4%), and the heart (11.6%)) [35], is highly sensitive and exposed to ischaemic damage. If oxygen supply is insufficient to meet the metabolic demands of the brain due to impaired lung mechanics or inadequate respiratory function in COPD patients, this can trigger the loss of vulnerable cerebral neurons [36]. Therefore, arterial hypoxia seems to be a major contributor to cognitive impairment with higher levels of oxygen desaturation increasing the risk of cognitive dysfunction [37]. Moreover, lower cognitive performance has been found to be related to elevated carbon dioxide tension (PCO2) and the occurrence of hypercapnia at rest or during activity [38, 39]. Evidence has shown that increased PCO2 is related to lower reaction times, delayed memory, slower information processing speed, and deficits in attention and concentration [40]. Also, study data has demonstrated that chronic hypoxia–hypercapnia can negatively affect patients’ cognitive function including some distinctive patterns of cognitive dysfunction [41]. In addition, Liesker et al. [42] have observed that overall cognitive impairment is significantly worse in both hypoxaemic and non-hypoxaemic COPD patients when compared to healthy individuals. Also, the overall relationship between PCO2 and cognitive impairment is even less clear when compared to low levels of oxygen. Van de Ven et al. [43] did not find abnormal cerebrovascular responses to carbon dioxide in hypercapnic patients with COPD and hypoxaemia or hypercapnia alone are not enough to entirely account for the observed cognitive deficits in patients with COPD. Additional risk factors that are not directly related to lung function could therefore be potential contributors to cognitive impairment in COPD.
Risk factors for cognitive impairment in COPD
Besides lower oxygen and/or higher carbon dioxide levels in blood, a complex interaction between pulmonary and non-pulmonary risk factors may account for COPD-related cognitive deficits [18]. According to the literature, other major risk factors which may potentially be associated with cognitive impairment are: 1) the presence of increased inflammation and oxidative stress [44, 45]; 2) reduced physical activity [46, 47]; 3) peripheral vascular disease [48]; 4) high or low blood pressure (non-normotensive patients) [49, 50]; 5) increased intracranial pressure associated with the narrowing of blood vessels in the brain [51]; 6) coexisting comorbidities [52]; 7) tobacco smoking [53]; and 8) genetic predisposition [54].
The pathophysiological mechanisms which link these risk factors with cognitive impairment are not clearly understood. It appears that there is a general concept that increased inflammation and oxidative stress, as well as the lack of physical activity, can express the ageing process and, therefore, increase age-related neurodegenerative changes [55]. Moreover, vascular disturbances leading to systemic hypertension or increased intracranial pressure are a risk factor for ischemic cortical infarcts [56]. On the other hand, systemic hypotension, which seems to be related to cerebral hypoperfusion in response to the reduced blood flow often caused by increased medication, may be responsible for protein synthesis abnormalities and reduced oxygen availability resulting in neurodegenerative lesions [57]. Moreover, reduced tonic cortical arousal related to hypoperfusion may contribute to lower cognitive performance [58]. Coexisting comorbidities that contribute to overall lung disease severity [59] and tobacco smoking, which appears to modulate brain function through nicotine [53], may also be accountable for cognitive dysfunction. Furthermore, genetic abnormalities are a major contributor to cognitive disability [60]. Several risk factors for cognitive deterioration, both with an independent impact and with overlapping contributions towards the development of cognitive impairment, are illustrated in Figure 2.

{kind=link}
{kind=link}
Determinants of cognitive impairment with potential independent and overlapping impact on cognitive function. TNF-α: tumour necrosis factor-α; IL-1: interleukin-1; IL-6: interleukin-6; CRP: C-reactive protein.
Should cognitive function be evaluated in the initial respiratory assessment?
Cognitive impairment has a negative impact on the personal characteristics of COPD patients including psychological profile, conscientiousness and the general ability to communicate and understand. The prevention of cognitive impairment by early intervention is thus important for treating, delaying or postponing its underlying processes and dealing with potential functional impairments that can act as barriers to the therapeutic management of COPD [61]. Specifically, cognitive deficits can result in an inability to accurately perform given instructions in respiratory examinations, such as in spirometry where several respiratory manoeuvres are included. A concerning issue then arises, as this could result in erroneous estimations of lung function capacity and potential misdiagnosis of the stage of disease severity in COPD [62]. Similarly, these patients may not understand the meaning of maximal exercise tests resulting in lower effort and underestimation of their exercise performance [63]. Moreover, cognitive impairment may be held responsible for insufficient adherence to therapeutic modalities and/or to medication and this is costly. The lack of adherence to a therapeutic strategy is a significant obstacle in optimal management of COPD and results in increased rates of morbidity, healthcare expenditure, and hospitalisation, as well as increased risk of mortality, unnecessary escalation of therapy and poorer quality of life [64]. Evidence has shown that an average of 40 to 60% of patients with COPD are committed to the prescribed regimen while only 1 in 10 patients with a metered-dose inhaler perform all of the essential steps correctly [65]. Communication problems and/or misunderstandings between patient and doctor may also result in refusal of treatment [66]. Forgetting or refusing to take a prescribed dose is usually the most frequent cause of non-adherence [67]. Furthermore, COPD patients with cognitive impairment may exhibit more functional dependence during a pulmonary rehabilitation programme and gain less benefits from it compared to cognitively intact counterparts [68].
Taking into account all the aforementioned issues, it is reasonable to conclude that cognitive function should be part of the initial respiratory assessment, especially for those patients presenting evident or self-reported symptoms of cognitive deficit, preferably corroborated by a close-informant [69]. Cognitive function also deserves particular attention in older patients (>65 yrs) at high risk, such as COPD patients with hypoxaemia, increased inflammation and coexisting comorbidities. Therefore, healthcare professionals who deal with elderly COPD patients are advised to be skilled in administering at least one brief cognitive test to a patient when cognitive impairment is suspected [70]. Timely detection of mild cognitive impairment (MCI) and awareness of this disorder is of great importance as actions can be taken to minimise or even to reverse cognitive decline and its consequences, and identify patients with increased risk of developing dementia.
Treatment of cognitive impairment as part of respiratory care
The goal of COPD management is to improve a patient’s functional status by preserving optimal lung function and to improve quality of life by mitigating the symptoms of disease and preventing secondary complications or recurrence of exacerbations [1]. However, the high prevalence of cognitive impairment in patients with COPD, in association with the detrimental consequences of cognitive deficits on functional status and quality of life, may indicate that action should be taken towards dealing with cognitive impairment within the frame of respiratory treatment. According to the literature there are some modifiable factors, such as physical activity [71, 72], balanced diet [73], cognitive training [74] and social engagement [75], that can be improved to provide beneficial effects to patients with COPD who have presented evidence of cognitive impairment.
Pulmonary rehabilitation as a multidimensional programme of exercise and education can be highly recommended for COPD patients with cognitive impairment [76]. The exercise programmes implemented during pulmonary rehabilitation, along with nutritional support, have been recommended as effective strategies to counteract neurological and cognitive disorders [77]. In addition, pulmonary rehabilitation provides patients with the opportunity to establish social contacts, obtain support and sympathy, and interact with, encourage, and motivate the other participants [78]. Pulmonary rehabilitation has also been found to reduce symptoms of depression and anxiety in COPD patients [79,80,81]. All these aforementioned favourable effects can be very promising for cognitively impaired patients with COPD. Indeed, Pereira et al. [82] have investigated the effects of pulmonary rehabilitation on cognitive function in patients with COPD and have reported significant improvements in cognitive performance even after adjustment for sociodemographic factors. Clinical improvements in visual attention, verbal memory and visuospatial skills have also been demonstrated in cognitively impaired COPD patients after participating in a 3-week rehabilitation programme [83]. Moreover, oxygen therapy may ameliorate or delay the progression of some cognitive deficits. Karamanli et al. [84] have demonstrated that the global cognitive function of COPD patients who did not use long-term oxygen therapy was worse compared to those who did. Indeed, the effect of such therapy on cognitive function has been found to be especially beneficial in hypoxaemic patients [37]. Considering the high prevalence of cognitive impairment, its consequences in patients with COPD and the importance of timely detection of cognitively impaired patients, special attention to COPD-related cognitive impairment is needed within the frame of respiratory assessment. Moreover, the beneficial effects of pulmonary rehabilitation on cognitive function could be an argument for prioritising the attendance of COPD patients with cognitive deficits in a comprehensive pulmonary rehabilitation programme.
Conclusions
Cognitive impairment is a prevalent limitation in patients with COPD and cognitive deficits should therefore be considered prior to healthcare planning. It is important for healthcare professionals to be aware of potential cognitive deficits in patients with COPD that could limit the effectiveness of respiratory therapy. Healthcare professionals in respiratory settings are advised to know how to administer a brief cognitive assessment test to detect COPD-related cognitive impairments when required. Early detection of cognitive impairment can prevent or delay its underlying processes and minimise potential obstacles in therapeutic strategy. COPD patients exhibiting evidence of cognitive impairment should be prioritised for participation in a comprehensive pulmonary rehabilitation programme.
Educational questions
Regarding the impact of lung impairment on cognitive function in COPD, which of the following is true?
a) COPD patients with cognitive impairment present disadvantageous cognitive deficits in all the major cognitive domains.
b) COPD patients with cognitive impairment present profound cognitive deficits, primarily on memory ability, even though they are able to provide detailed examples of forgetfulness.
c) COPD patients developing cognitive impairment present cognitive deficits in at least one cognitive domain, whilst the rest of the domains can be unaffected.
d) COPD patients developing cognitive impairment may only occasionally present cognitive deficits in several cognitive domains.
What is the major problem related to cognitive impairment in respiratory assessment?
a) Patients’ forgetfulness and inability to understand instructions for the ongoing management of their disease may cause delays and act as a barrier to therapeutic management.
b) Communication problems or memory deficits due to cognitive impairment may result in misleading information being provided to healthcare professionals by patients.
c) Communication problems between patients and healthcare professionals may limit the application of important tests during respiratory assessment.
d) Patients’ inability to accurately perform respiratory manoeuvres and their lack of effort in stress tests may result in erroneous estimations of the progress of disease severity.
Why is early detection of cognitive impairment within the respiratory assessment important?
a) Because it averts or addresses potential safety issues.
b) Because there are certain modifiable factors (i.e. physical activity, cognitive training and social engagement) that can be improved, presenting beneficial effects on cognitive impairment.
c) Because it ensures that patients will have a caregiver or someone else to help them with their medical treatment.
d)Because it allows healthcare professionals to plan long-term treatment and care.
Why can pulmonary rehabilitation (PR) be beneficial to cognitive impairment in COPD?
a) Because exercise training may counteract neurological and cognitive disorders.
b) Because patients establish social contacts, obtain support and reduce anxiety/depression, and these factors have favourable effects on cognitive impairment.
c) Because clinical improvement has been reported in visual attention, verbal memory and visuospatial skills even after a short-term PR program (3 weeks).
d) Because of all of the above.
Suggested answers
c
d
b
d
Footnotes
Support statement V. Andrianopoulos is the recipient of an ERS Long-Term Research Fellowship (LTRF 63-2012) and an ERS–EU RESPIRE2 Marie Sklodowska-Curie Postdoctoral Research Fellowship (MCF 8465-2015). Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interestNone declared.
- Received January 31, 2017.
- Accepted February 13, 2017.
- Copyright ©ERS 2017
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Cognition and neuropsychological domains
- Assessment of cognitive function
- Lung impairment and cognitive function
- Risk factors for cognitive impairment in COPD
- Should cognitive function be evaluated in the initial respiratory assessment?
- Treatment of cognitive impairment as part of respiratory care
- Conclusions
- Educational questions
- Suggested answers
- Footnotes
- References
- Figures & Data
- Info & Metrics