





Abstract
Can you diagnose this 61-year-old male with generalised lymphadenopathy, dyspnoea and radiographic infiltrates? http://ow.ly/AXDg306hfqo
Case presentation
A 61-year-old man presented for evaluation of a 6-week history of dyspnoea on exertion that had worsened over the past week. He denied having any recent illness, fevers, night sweats, nausea, vomiting, cough, chest pain, palpitations, or leg or back pain. He was diagnosed with chronic lymphocytic leukaemia (CLL) 5 years previously and had never been on chemotherapy.
On examination, he appeared healthy and in no apparent distress. His blood pressure was 133/82 mmHg, pulse 76 beats per min, respiratory rate 17 breaths per min and oxygen saturation 96% on room air. Physical examination revealed no jugular venous enlargement, few mobile nontender anterior cervical lymph nodes and tender bilateral axillary lymphadenopathy. No adventitious sounds were audible over either lung. Cardiac examination revealed normal heart sounds with no gallop or murmur. His abdomen was benign. Pertinent laboratory test results included a serum sodium concentration 145 mmol⋅L−1, potassium 4.4 mmol⋅L−1, blood glucose 113 mg⋅dL−1, blood urea nitrogen 21 mg⋅dL−1, bicarbonate 26 mmol⋅L−1, creatinine 0.9 mg⋅dL−1, haemoglobin 14.1 g⋅dL−1, white blood cells 23.2×103 per dL (neutrophils 16%, lymphocytes 82%, monocytes 1%, basophils 1%) and platelets 133 000 per dL. Sputum cultures were negative for bacteria, acid-fast bacilli and fungus including Aspergillus. The patient underwent chest radiography (figure 1).

Chest radiograph.
Task 1
What does the chest radiograph demonstrate and what would you do at this point?
Answer 1
The chest radiograph demonstrated well-defined scattered rounded nodules bilaterally and a large dense opacity overlapping the left cardiac contour. Obtaining a computed tomography scan of the chest should be a reasonable next step to define these opacities more comprehensively.
Task 2
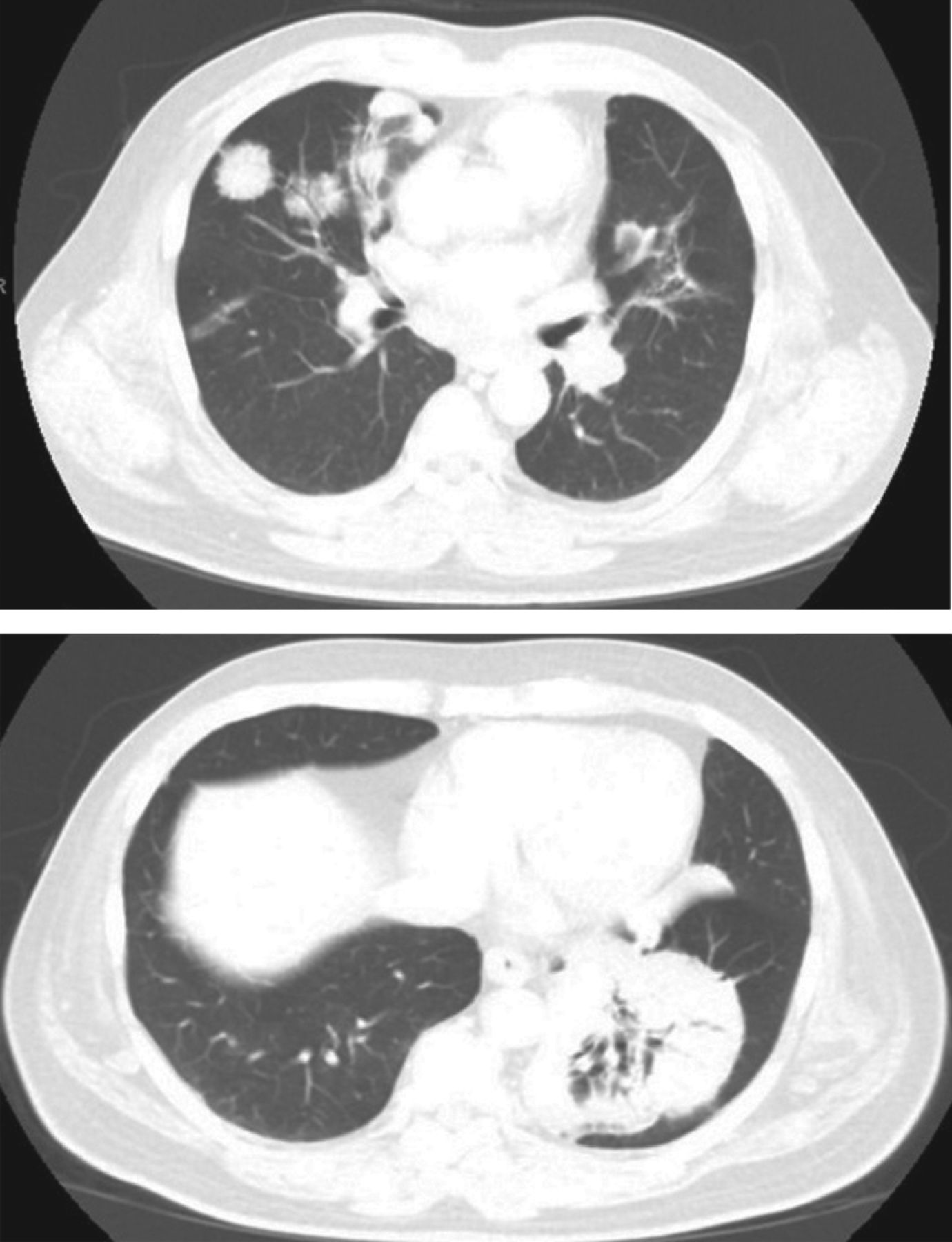
Describe the imaging findings noted on the computed tomography scan of the chest (figure 2).

Chest computed tomography.
Answer 2
The images demonstrate multifocal variably dense nodular consolidation, many of which are clearly peribronchial in distribution. A dense consolidation occupies the vast majority of the posterior basal and medial basal segments of the left lower lobe (LLL) (10×9×7 cm). Multistation bulky lymphadenopathy involving the cervical, bilateral axillary, mediastinal and hilar (left greater than right) was noted.
Task 3
What is the most appropriate diagnostic step and what are the differential diagnoses?
Answer 3
The next step should be an attempt to obtain lung tissue for histopathological diagnosis. Review of the location of the consolidation and nodules indicates that a bronchoscopic approach with transbronchial biopsies from the area of interest is a reasonable option.
The patient underwent bronchoscopy that showed a raised polypoidal mucosal irregularity arising from the right wall of the distal trachea, above the carina from which endobronchial biopsies were obtained. Bronchoalveolar lavage (BAL) revealed lymphocytic-predominant fluid with negative cultures. Transbronchial biopsies from the LLL consolidation were obtained
Patients with leukaemia will often have abnormalities on chest imaging; the differential diagnosis is broad. Nodules, masses and infiltrates are commonly seen in patients with haematologic malignancies and the differential diagnosis for each of these is expansive. Factors that help to narrow the list of possibilities include: the stage of leukaemia, its aggressiveness, and history of prior treatment including previous stem cell transplant. Approaching the clinical problem begins with a review of the differential diagnosis for pulmonary infiltrates in the immunocompromised patient (table 1) [1].
Causes of focal/nodular lung infiltrates in a patient with leukaemia

Infections with Mycobacterium tuberculosis, nontuberculous mycobacteria, Nocardia sp., Pneumocystis jirovecii or Aspergillus sp. are more likely in those who are immunosuppressed. The size and location of the lesion may often help with diagnosis. Subcentimetre lesions are infrequently neoplastic. However, masses >3 cm are likely to be cancerous. Upper lobe lesions are more likely to be neoplastic. Ground-glass opacification may indicate malignancy, as does air bronchogram within the nodule. Calcification patterns such as diffuse, central and laminar patterns indicate a benign process. The halo sign (dense nodule with surrounding ground glass) is classically associated with invasive aspergillosis but can also be seen with leukaemic bronchopulmonary infiltration (LBPI) [1]. The reverse halo (ground glass surrounded by ring of consolidation) is described with invasive fungal infections, pulmonary infarcts, sarcoidosis, pneumocystis pneumonia, cryptogenic organising pneumonia and pulmonary neoplasms [2]. Ante mortem diagnosis of leukemic lung infiltration due to CLL is rare. Its incidence has been reported to be 2.1% among patients with CLL who are admitted with any respiratory symptoms [3]. Surprisingly, an autopsy series reported that 41% of patients with CLL have leukaemic infiltration of the lungs, indicating that the bulk of such infiltration is subclinical [4].
Notwithstanding the broad differential diagnosis, it is to be emphasised strongly that pulmonary infiltrates in the setting of CLL should be considered to be infectious in nature unless proven otherwise. Besides infection and LBPI, other infrequent causes of pulmonary infiltrates include drug toxicity, pleural effusions and extrinsic bronchial obstruction due to mass effect from enlarged lymph nodes without actual parenchymal involvement [5]. Hence, in the absence of a clear diagnosis from history and physical examination in this case, a bronchoscopy and lung biopsy should be pursued.
Answer 4
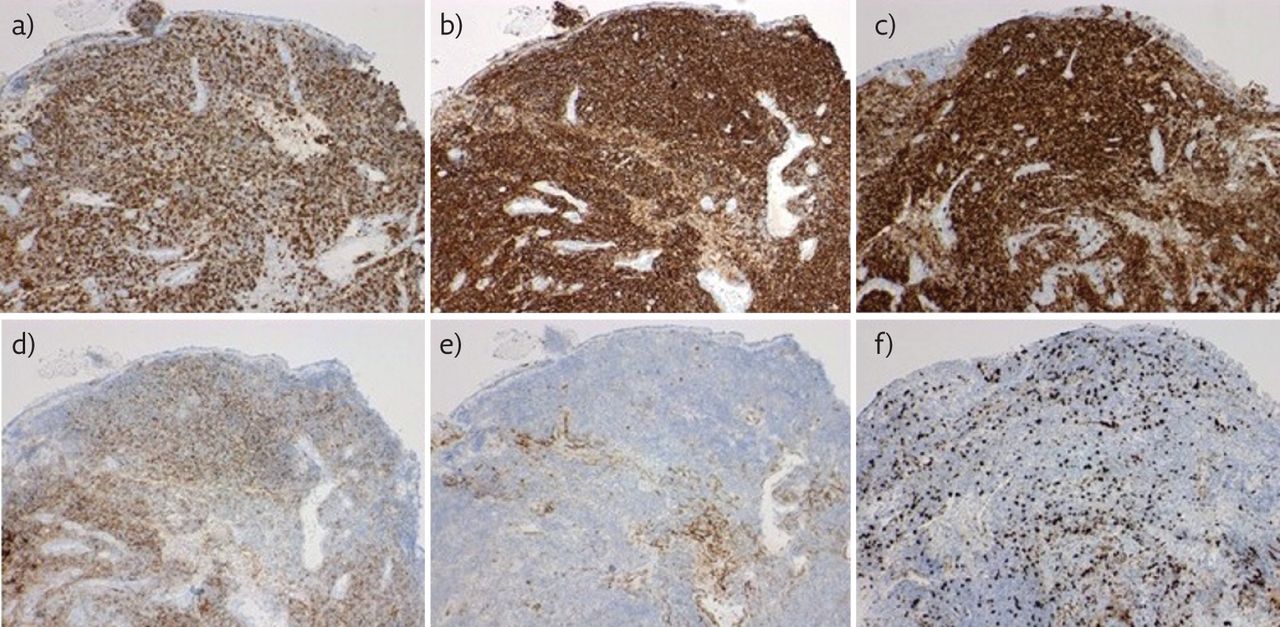
BAL revealed lymphocytic predominant fluid with negative cultures. Results of transbronchial lung biopsy revealed diffuse small and uniform lymphocytic infiltrates (figures 3 and 4). Immunostaining of the LLL mass tissue samples was positive for BCL2, CD20, CD3, CD5, CD10 (focal) and negative for cyclin D1 (figure 5). Endobronchial biopsies from the tracheal lesion demonstrated similar lymphoid infiltrates supportive of endobronchial involvement by leukaemic cells. Flow cytometry and fluorescence in situ hybridisation (FISH) on the lymphocytes revealed that the lymphocytes were ZAP70 and CD38 positive, and had deletion of ATM (ataxia teleangiectasia mutated) gene on chromosome 11q.
We then performed peripheral blood flow cytometry that confirmed the presence of leukaemic cells with CD19 and CD20 markers indicative of a B-cell origin. Peripheral lymphocyte FISH analysis showed 11q deletion.
Documenting identical molecular signature of the circulating malignant lymphocytes in blood with those in the lung indicated that the patient had leukaemic bronchopulmonary infiltration from progressive B-cell CLL.

High-power images (haematoxylin and eosin staining). a) 20×; b) 40×.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemistry of the transbronchial biopsy specimen. a) CD3 (10×); b) CD20 (10×); c) CD5 (10×); d) CD23 (10×); f) Ki-67 (10×).
Discussion
Pulmonary involvement in CLL may take one of the following forms.
1) LBPI
2) Peribronchial and perivascular infiltration leading to endobronchial obstruction and post-obstructive pneumonia
3) Pleural effusion and intrathoracic lymphadenopathy
4) Pulmonary hyperleukostasis
5) Richter’s syndrome/transformation
Clinical features of LBPI
Those with LBPI often present with vague symptoms such as dry cough, progressive dyspnoea, chest pain and haemoptysis.
Radiology
LBPI is radiologically characterised by bilateral reticular prominence that may, at times, resemble lymphangitis carcinomatosis. The presence of peribronchovascular thickening and nodules, and interstitial septal thickening is common [6]. Septal thickening may either be smooth or nodular (equally common). Infiltration of leukaemic cells into the adjacent air spaces can give rise to focal areas of consolidation in a peribronchial distribution. Bilateral mediastinal adenopathy and centrilobular nodules in a “tree-in-bud” pattern have also been described [7]. Some patients may develop bronchiectasis and ground-glass opacities (GGO) in a centrilobular distribution. Bronchiectasis is thought to be a sequelae of repeated infections in the presence of extrinsic obstruction of a bronchus [8]. Unfortunately, there is no specific radiological feature that can be considered sine qua non for LBPI.
Histopathology
Diagnosis is challenging in most cases. BAL, endobronchial and transbronchial biopsies are the most useful means of diagnosis. A lung biopsy, either bronchoscopic or open, should be obtained if LBPI is clinically suspected. It is to be remembered that the mere presence of lymphocytic alveolitis on a BAL should not be taken as conclusive proof of LBPI since CD8 alveolitis can occur with many infections and drug toxicity. BAL samples often do not provide information on organisation, infiltration or interaction of these cells with the underlying tissues, and hence, their utility is limited. Hence, with a high clinical suspicion, even in the face of negative BAL cytology, a lung or endobronchial biopsy should be obtained.
A lung biopsy demonstrating bronchocentric lymphoid hyperplasia is thought to be suggestive of this condition. However, this can also be seen in other conditions such as collagen vascular diseases, hypersensitivity pneumonias, sarcoidosis and follicular bronchiolitis. This makes flow cytometry the most useful ancillary study in detecting a clonal population of lymphocytes. With a lymphocyte-dense tissue biopsy, the differential diagnosis can again be quite broad. This would include nonmalignant conditions (normal bronchus-associated lymphoid tissue, infection, lymphocytic interstitial pneumonitis, etc.), haematopoietic disorders (other low-grade and high-grade B-cell disorders, mucosa-associated lymphoid tissue, lymphomatoid granulomatosis, etc.) and even epithelial malignancies that are histological mimickers (lymphoepithelial-like carcinoma and small cell carcinoma). The characteristic phenotype for B-cell CLL is CD20, CD5 and CD23 positive. B-cell prolymphocytic leukaemia cells can express CD22, which helps to differentiate it from CLL. Occasionally, other B-cell neoplasms such as hairy cell leukaemia, lymphoplasmacytic lymphomas and follicular lymphomas also have B-cell lineages (CD19 and CD20 positive) but lack the CD5 marker, thus helping us to distinguish these from classic B-cell CLL. Cyclin D1 negativity can help distinguish CLL from mantle-cell lymphoma, which is CD22 positive, CD23 negative and cyclin D1 positive [9]. Although we could confirm CLL involvement of the lung, the question of Richter’s transformation is one that requires morphological evaluation. Richter’s syndrome is a rare condition (2–10% of all cases) where CLL transforms into a more aggressive form of diffuse B-cell lymphoma. The lung is considered an important extranodal site of involvement in Richter’s syndrome (13%). The infiltrate in our case consists of small to medium-sized lymphocytes with an overall low Ki-67 proliferation index (usually Ki-67 >40% and large lymphocytes are seen in Richter’s transformation) not favouring a high-grade/Richter’s transformation [10].
In the absence of high-quality data, LBPI is thought to carry a grave prognosis. It is unclear if the advanced form of CLL predisposes to the development of LBPI. That possibility appears unlikely based on the results of a case series of six patients which revealed that all patients with LBPI had stable disease and were in remission for 6 months prior to diagnosis [5]. The treatment of choice is chemotherapy with the goal focused on controlling the disease, rather than a cure. Radiation therapy, biological therapy and bone marrow transplantation are rarely viable options for these patients.
Follow-up
The patient had an uneventful recovery after lung biopsy. He has experienced significant improvement in respiratory symptoms with combined bendamustine and rituximab therapy.
Conclusion
LBPI is infrequently seen in CLL. There are no pathognomonic radiological signs for this condition. Diagnosis depends on histopathological examination of the lung biopsy samples, and in requesting flow cytometry and FISH analysis. This will help in identifying similar lymphocyte markers and genetic rearrangements between the peripheral blood leukaemic cells and the cells infiltrating the lungs.
Footnotes
Conflict of interestNone declared.
- Copyright ©ERS 2017
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










