





Abstract
In contrast to airway diseases like chronic obstructive pulmonary disease or asthma, and rare diseases such as cystic fibrosis, there has been little research and few clinical trials in bronchiectasis. Guidelines are primarily based on expert opinion and treatment is challenging because of the heterogeneous nature of the disease.
In an effort to address decades of underinvestment in bronchiectasis research, education and clinical care, the European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) was established in 2012 as a collaborative pan-European network to bring together bronchiectasis researchers. The European Respiratory Society officially funded EMBARC in 2013 as a Clinical Research Collaboration, providing support and infrastructure to allow the project to grow.
EMBARC has now established an international bronchiectasis registry that is active in more than 30 countries both within and outside Europe. Beyond the registry, the network participates in designing and facilitating clinical trials, has set international research priorities, promotes education and has participated in producing the first international bronchiectasis guidelines. This manuscript article the development, structure and achievements of EMBARC from 2012 to 2017.
Educational aims
To understand the role of Clinical Research Collaborations as the major way in which the European Respiratory Society can stimulate clinical research in different disease areas
To understand some of the key features of successful disease registries
To review key epidemiological, clinical and translational studies of bronchiectasis contributed by the European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) project in the past 5 years
To understand the key research priorities identified by EMBARC for the next 5 years
Abstract
Learn about @EMBARCnetwork, a successful @ERStalk Clinical Research Collaboration with @EuropeanLung http://ow.ly/IOl230drGf1
Patients with bronchiectasis typically suffer from cough, sputum production, frequent chest infections and a number of other symptoms on a daily basis [1, 2]. In addition, patients have to struggle with the uncertainty provoked by frequent, unpredictable disease exacerbations [3, 4]. On top of the physical symptoms, patients have to deal with a diagnostic delay that is not infrequently more than a decade, and many patients are acutely aware that primary care physicians and nonspecialists know little about their condition, and that the evidence base for treatment is poor [5, 6].
Bronchiectasis has been described as an orphan disease but while the European Union (EU) defines an orphan or rare disease as one affecting fewer than one in 2000 people, the latest estimates suggest that bronchiectasis is relatively common [7–10]. Most recent estimates place the true prevalence at one in 206 for men and one in 176 for women in the UK, one in 276 persons in Catalonia (Spain), and one in 1492 persons in Germany [7–10]. Bronchiectasis is therefore not an orphan disease in the true sense of prevalence but has the characteristics of an orphan disease in terms of a weak evidence base, a lack of attention from scientists, clinicians, regulators and funders, and an absence of high-quality randomised controlled trials [11–13].
Although guidelines on the management of cough from CHEST in the USA in 2006 may be regarded as one of the first guidelines for bronchiectasis, the first guidelines to attempt to cover the totality of investigation and management of bronchiectasis worldwide were the Spanish (SEPAR) guidelines published in 2008 and subsequently the British Thoracic Society Guidelines in 2010 [12, 14, 15]. A reflection of poor state of evidence at that time is the fact that only three recommendations in the ≥200-page British Thoracic Society document were given a grade A recommendation, meaning the authors had a high degree of confidence in the recommendation [12]. These were to screen for antibody deficiency by measuring immunoglobulins, to offer physiotherapy exercises such as the active cycle of breathing technique and that recombinant DNAse should not be used for treatment [12, 16]. The majority of treatment recommendations were given a Grade D recommendation indicating expert opinion in the absence of robust evidence [12].
Europe has contributed a substantial majority of the published data on bronchiectasis over the past 20 years. A systematic review by Aliberti et al. [17] (2000–2015) showed that even within Europe, the majority of published studies were from the UK, with further contribution from Spain, Italy and other Western European countries but with a paucity of published data from Eastern Europe (figure 1). Collaborative studies involving data from more than one European country could not be identified prior to 2014.

Published original research studies in 2000–2015 on adult bronchiectasis worldwide (excluding cystic fibrosis).

Sites participating in the EMBARC registry as of January 2017.

The EMBARC registry flow chart. CT: computed tomography. Reproduced from [18].
The backdrop to the development of the European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) project was therefore a common and disabling chronic disease, a limited research and evidence base, a hostile funding environment, and an absence of pan-European cooperation and coordination.
What is EMBARC?
EMBARC was established in 2012 as a collaborative group within European Respiratory Society (ERS) Assembly 10 (Respiratory Infections) with the objective of creating a European bronchiectasis registry, harmonising existing databases, and identifying opportunities to raise the profile of bronchiectasis at ERS and EU levels [18, 19].
In 2013, EMBARC applied to become an ERS Clinical Research Collaboration (CRC). ERS contributes to the coordination of activities in respiratory medicine across Europe by funding CRCs, which are designed as pan-European networks aiming to create a critical mass of research expertise to improve clinical research within a specific disease area [20]. EMBARC was one of the first ERS CRCs to be funded (in 2013, with funding running from 2014 to 2017). The portfolio of CRCs is now highly diverse, covering disease areas from sleep apnoea, intensive care unit-related respiratory infections, childhood and adult interstitial lung diseases, severe asthma, and pulmonary function [20, 21].
CRCs stimulate research in a number of ways. In addition to funding, they provide access to the considerable resources of the ERS, providing access to ERS members, national delegates and national societies through the Forum of International Respiratory Societies (FIRS) (https://www.firsnet.org/news-and-actions). They provide the ability to hold meetings and symposia at the ERS International Congress and, perhaps most importantly in the case of EMBARC, they provide an identity and mark of approval to the network, which enables the network to recruit both funders and participants through the trust that individual healthcare professionals, patients and funders have in the ERS [20, 21].
EMBARC was approved as an ERS CRC in 2013, chaired by J.D. Chalmers from the University of Dundee (Dundee, UK) and E. Polverino from the University of Barcelona (Barcelona, Spain), with the collaboration offices based at the University of Dundee.
Setting up an international registry
The primary objective of the EMBARC CRC was the creation of a pan-European, prospective registry of patients with bronchiectasis [18]. No pan-European registries for bronchiectasis existed prior to 2015, with only a small number of countries or individual regions within countries having registries [22].
In developing the registry, the project coordinators followed EU guidance on the development of rare disease registries [23, 24]. The recommendations from the EU Committee of Experts on Rare Diseases (EUCERD) are shown in table 1, along with the mechanisms used by EMBARC to address these recommendations [23].
EUCERD recommendations for rare disease (RD) registries
Selected translational research priorities from the EMBARC roadmap [19]
The EMBARC registry used a “hub and spoke” model to grow the registry across Europe, initially recruiting national experts or “champions” in individual countries who acted as the initial recruiting centres, and assisted with obtaining ethical/institutional review board approval and recruiting other centres in their respective countries, with the support of FIRS and the ERS national delegates. This was supplemented with e-mail invitations to participate through ERS Assembly 10 and publicity surrounding the launch of the registry at the ERS International Congress. This resulted in the recruitment of >150 centres in >40 countries (including both EU and non-EU countries) (figure 2). Importantly, EMBARC sought to establish a pan-European registry rather than merging existing datasets or national registries. By defining a core dataset that everyone in Europe shared, EMBARC avoided the problem of later having to achieve interoperability between different registries using different definitions on different platforms. This may not be possible for all disease areas, where existing infrastructure in some countries may already exist.
The EMBARC registry
The EMBARC registry is managed from a data coordinating centre in the UK at the University of Dundee and received ethical approval in the UK in January 2015 (14/SS/1101). The study website is www.bronchiectasis.eu. A detailed protocol of the study has been published [18]. In brief, the inclusion criteria are a clinical history consistent with bronchiectasis (cough, chronic sputum production and/or recurrent respiratory infections) and computed tomography of the chest demonstrating bronchiectasis (bronchial dilatation) affecting one or more lobes. The exclusion criteria are bronchiectasis due to known cystic fibrosis, age <18 years and patients that are unable or unwilling to provide informed consent (figure 3). Patients are followed up on an annual basis with a detailed review case report form [18]. To date, the registry has recruited >8000 patients in just over 2 years of recruitment.
Data access rules and governance
Involvement of all relevant stakeholders, and fair and open access to data is essential for the success of large-scale registries and studies. EMBARC has achieved this by involving key opinion leaders and experienced bronchiectasis researchers in a registry steering committee that has guided the project from 2014 to 2017 (https://www.bronchiectasis.eu/steering-commitee), by maintaining an international advisory board that includes the leads for the key non-European registries and experts representing four continents (https://www.bronchiectasis.eu/international-advisory-board), and by having a transparent data access policy.
Patients contribute their time to participating in research, and contribute their data to a registry because they want to see the data used to improve clinical care and to bring forward advances in medical research. The EMBARC registry has therefore been developed with the principle that data should be a freely available as possible, and that the results of the study should be disseminated as widely as possible in order to have the greatest possible impact on health and patient care.
The process of applying for data access is simple. The data access application form can be downloaded from https://www.bronchiectasis.eu/dataaccess
Governance processes surrounding data management and access are fully compliant with the UK Data Protection Act 1998, and Data Protection Directive 95/46/EC of the European Parliament and of the Council (1995) (this will be updated when the new EU data protection regulations take effect) [18].
A scientific committee, consisting of up to seven academic members of the EMBARC network, review all data requests to ensure scientific quality, and to plan the most appropriate publication and dissemination plans for registry data.
A crucial component of a successful network is a transparent, democratic and open approach. All positions within EMBARC committees and working groups are elected. Decision making is transparent with consultation and voting among the relevant committees where required. An annual meeting of the whole EMBARC network is held at the ERS International Congress each year with more regular meetings of the executive and steering committees. All of the major contributing countries to EMBARC have a representative that forms part of the governance structure, ensuring that each contributing country has an equal voice in decision making.
Patient involvement
EMBARC works closely with the European Lung Foundation (ELF) (www.europeanlung.org), which was established by the ERS in 2000 with the aim of bringing together patients and the public with respiratory professionals to positively influence lung health. The design of the registry and all EMBARC activities have been informed by review and feedback from patients and patient groups [26, 27]. The ELF and EMBARC have ensured ongoing patient involvement in the network through the creation of a patient advisory group (PAG) consisting of people with bronchiectasis and those affected by bronchiectasis, such as parents, partners or children of someone with bronchiectasis. All EMBARC projects and meetings now involve patient representatives.
Achievements of EMBARC
The EMBARC registry represents a major achievement in the field of bronchiectasis given the lack of coordinated research activity prior to the commencement of the EMBARC study in 2015. The EMBARC protocol was published in 2016 and the first data publications from the EMBARC registry will be submitted for publication in mid- to late 2017 [18]. In addition to the registry, EMBARC has contributed to the field in a number of important ways since 2012 as described below.
Publications
EMBARC aligned 10 datasets from different European countries, which were collected by investigators prior to the start of the EMBARC registry in 2015 [28–34]. This approach of pooling existing datasets is commonly utilised in other diseases; for example, cystic fibrosis and primary ciliary dyskinesia [35, 36]. By standardising definitions, end-points and covariate data-points, a dataset of >2000 patients has been built for epidemiological studies. The dataset is designated FRIENDS (Facilitating Research Into Existing National Datasets) [28–34]. This cohort was used to derive and validate the first multicomponent clinical prediction tool for bronchiectasis, the bronchiectasis severity index (BSI) [37]. The study showed that a small number of key parameters were associated with mortality, hospital admissions, quality of life and future exacerbations [37]. Specifically, the BSI consists of age, functional status (Medical Research Council dyspnoea score), forced expiratory volume in 1 s (FEV1), radiological severity (number of lobes involved or the presence of cystic dilatation), low body mass index (<18.5), frequency of exacerbations, history of hospitalisation for severe exacerbations and the presence of chronic infection with bacteria or particularly with Pseudomonas aeruginosa. The resulting score is available at www.bronchiectasisseverity.com [37].
Subsequently, the BSI was compared to a second scoring system, the FACED score (FEV1, age, chronic colonisation, extension and dyspnoea), for its ability to predict clinically relevant outcomes [29]. Both scores appear to perform equally well for the prediction of mortality across several cohorts but the EMBARC study of 1612 patients found that the BSI also predicted hospital admissions for severe exacerbations, moderate exacerbations, quality of life, respiratory symptoms, and even 6-min walk distance and lung function decline [29]. In contrast, the FACED score did not consistently predict any relevant clinical outcomes beyond mortality [29].
Collaborators from EMBARC have also published data demonstrating the characteristics of bronchiectasis in the elderly [30], demonstrating that only a minority of bronchiectasis patients are represented in current randomised clinical trials, such as those of inhaled antibiotics and mucoactive therapies [31].
A cluster analysis of different clinical characteristics performed by Aliberti et al. [32] identified four clusters of patients with different “phenotypes” and different outcomes. Bacteriology in sputum, defined by the presence of P. aeruginosa or other bacteria, were key drivers of clinical characteristics, while a third cohort was patients with daily sputum without chronic colonisation, and the final group were patients with dry bronchiectasis. Higher levels of neutrophilic inflammation were associated with the two bacterial colonisation phenotypes, consistent with prior literature [32].
Research priorities identified by the PSG have led directly to important EMBARC publications. The PAG overwhelmingly felt that comorbid conditions were often their most important determinants of quality of life. Based on their recommendation, the FRIENDS database was used to investigate the relative importance of comorbidities to disease outcomes in bronchiectasis. Standardised definitions of comorbidities were applied across the datasets to 986 patients with bronchiectasis. Patients had a median of four comorbidities per patient (with some patients having up to 20). 13 comorbidities were independently associated with mortality in multivariable analysis [28]. Although the individual contribution of each comorbidity was modest, multiple comorbidities that could be added together as part of an aetiology and comorbidity index (Bronchiectasis Aetiology and Comorbidity Index) predicted mortality and were associated with health-related quality of life as measured by the St George’s Respiratory Questionnaire. Patients with more comorbidities also had more exacerbations. The study confirmed the view of the PAG that multimorbidity is a major determinant of quality of life and outcomes in bronchiectasis [28].
Further work has defined the most common underlying causes of bronchiectasis in Europe, with 20% being classified as post-infective, 15% due to chronic obstructive pulmonary disease (COPD), 10% due to connective tissue diseases and 6% due to immunodeficiency [33]. 13% of cases led to a change in patients’ management [33]. De Soyza et al. [34] recently confirmed that patients with rheumatoid arthritis-associated bronchiectasis and COPD have worse clinical outcomes. EMBARC researchers have also recently identified a series of biomarkers associated with worse outcomes [38, 39].
A meta-analysis performed by EMBARC researchers identified that patients with P. aeruginosa infection are at three-fold increased risk of death and seven times more likely to be admitted to hospital for severe exacerbations [40].
Improving the quality of care for patients with bronchiectasis is also a major priority for the network. An audit conducted in Italy showed only 32% of patients had aetiological testing for allergic bronchopulmonary aspergillosis and immunodeficiency, with nearly 60% of patients having no aetiological testing [41]. Only 27% of patients had a sputum culture once per year. Compliance with other quality standards of care was similarly low. Improving standards of care across Europe is important and will be a major objective following the publication of the 2017 ERS guidelines [41].
World Bronchiectasis Conference
EMBARC held the first international conference specifically focussed on bronchiectasis in 2016 in Hannover, Germany. The meeting was attended by nearly 300 delegates and was a great success both in terms of the scientific content and also in raising the profile of bronchiectasis. The second EMBARC World Bronchiectasis Conference was held in Milan, Italy in July 2017 and the third is scheduled for Washington, DC, USA, in 2018.
Consensus statements
Expert networks like EMBARC can provide important guidance to the field by producing consensus statements. The first such document was published by EMBARC in 2016 describing the research priorities for the field: the European Bronchiectasis Research Roadmap [19]. A Delphi process was conducted identifying the research priorities of a Europe-wide group of experts in bronchiectasis. This was complemented by a survey of nearly 1000 patients and carers to produce a physician/patient consensus of research priorities. 22 research questions and 55 different studies were proposed, emphasising the volume of work there is to be done [19] (table 2).
Exacerbations are the key clinical end-point in randomised controlled trials of bronchiectasis but all studies to date have used slightly different definitions of exacerbation [42–46]. This can have a major effect on the results of trials: too stringent a definition can result in missing a signal for benefit while too loose a definition can result in normal day-to-day variation in symptoms or side-effects from medications being classified as exacerbations. This can dilute a signal for benefit.
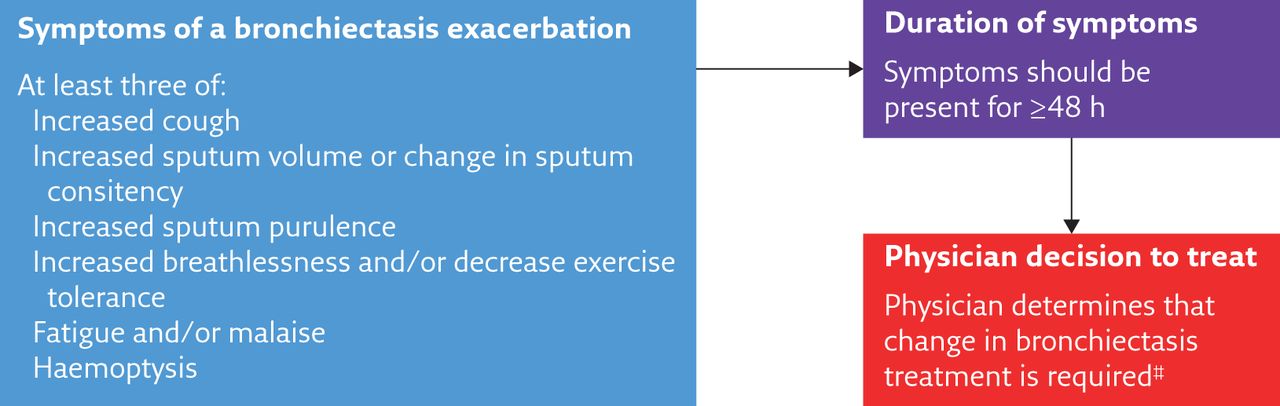
To address this, members of EMBARC led a consensus working group at the World Bronchiectasis Conference in Hannover, in collaboration with colleagues from the USA, Australia, South Africa and New Zealand [47]. A Delphi process identified the key symptoms and signs of exacerbation as determined by expert opinion, and a resulting simple and operational definition of exacerbation was approved and published (figure 4). It should be noted this definition is for use in clinical trials and is not intended to impact clinical care [47].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Consensus definition of bronchiectasis exacerbations for use in clinical trials. #: physicians should exclude other possible causes of deterioration in symptoms. Reproduced and modified from [47].
Such consensus statements, while based on expert opinion, can have an important impact on the field. Further consensus documents are planned in 2017 and beyond.
International bronchiectasis networks
In addition to supporting European research, EMBARC has made the dataset and platform available for international collaborators to use. Alignment with other international initiatives is a key EUCERD recommendation for registries, and allows integrated analysis and higher impact outputs. Two excellent examples of partnered international networks are the Australian and Indian registries.
The Australian registry is an initiative of the Lung Foundation of Australia. It collects the “core” dataset using the EMBARC platform allowing collaborative analyses but also incorporates unique Australian features, such as a paediatric component and data fields related to indigenous Australians, among others [48, 49]. This demonstrates the value of having a core dataset while permitting the flexibility to explore local strengths and key research questions at a local level. The Indian registry (EMBARC-India) is further example of this. Coordinated by the Respiratory Research Network of India and collecting data across 25 sites, this dataset represents the first attempt to understand the impact of bronchiectasis in south-east Asia where virtually no data have been published. The first results were presented at the American Thoracic Society Conference in 2017, with 680 patients reported. In contrast to European cohorts, the majority of patients were male (60%) and post-tuberculosis was the most frequent underlying cause (35.7%) [50].
More and more countries are developing bronchiectasis research infrastructure using the EMBARC platform as a basis for ensuring interoperability and future intercontinental research.
Randomised controlled trials
EMBARC ultimately wishes to facilitate and support randomised controlled trials within its network. At the time of writing, EMBARC is actively supporting three randomised controlled trials of new therapies for bronchiectasis. The registry provides a powerful tool for planning and executing trials, by allowing feasibility studies to determine how changes in protocol design may impact recruitment, and by identifying which sites are most likely to contribute to trials and can be used to actively encourage investigators to take part in trials. The registry and EMBARC network can also provide patient input into trial design as well as facilitating expert review.
EMBARC is part of the iABC (Inhaled Antibiotics in Bronchiectasis and Cystic Fibrosis) consortium, an EU Innovative Medicines Initiative consortium that includes a programme to develop tobramycin dry powder for inhalation [51]. A phase 2 study is currently enrolling in Europe for bronchiectasis patients with P. aeruginosa infection.
The future: EMBARC 2
The registry and the associated projects described above represent important achievements for a previously neglected disease [52–55]. Nevertheless, the European Bronchiectasis Roadmap identified a series of priorities for research, only around half of which can be answered by epidemiological studies such as registries. In renewing the EMBARC project from 2017 to 2020, EMBARC has developed ambitious plans to expand its activities.
There has been little translational research into bronchiectasis and its pathophysiology remains largely unexplored. From 2017 to 2020, EMBARC will expand an international bioresource, using the registry as a backbone to build a repository of blood, DNA, sputum and other biological materials for use in translational research. This study will allow detailed studies on airway and systemic inflammation, microbiota and genomics to answer fundamental questions regarding pathophysiology [56–61].
The overlap between COPD, asthma and bronchiectasis is a key priority in the field, and will be explored in new clinical and translational studies within the network [6]. Furthermore, there are very few data published on the presentation and outcomes of patients with bronchiectasis during exacerbation. EMBARC has initiated an exacerbation study where patients are enrolled at the onset of exacerbation with detailed data collection and longitudinal follow-up in the registry. This will allow a deeper understanding of presentation and outcomes of bronchiectasis exacerbations.
Nontuberculous mycobacterial (NTM) disease represents a major healthcare problem linked to bronchiectasis [62]. >50% of patients in the US bronchiectasis registry have co-existing NTM disease, whereas the rate is much lower in Europe [25]. Since NTM patients require different management to those with bronchiectasis without NTM, EMBARC will launch a specific registry for NTM, with new data fields and a separate governance structure, in 2017 to capture and study in greater detail this important patient group.
The development of EMBARC from 2017 to 2020 illustrates what is possible with the support of a successful registry and with the support of a group of highly motivated international experts.
Conclusion
EMBARC is a successful ERS CRC. The major factors in its success are a clear set of objectives, engagement from the overwhelming majority of experts and stakeholders in the field, a highly professional organisational infrastructure, and dedicated cooperative members who have a unifying goal of improving patient care.
EMBARC has already made an important contribution to bronchiectasis research and guidelines. Developments in the next 3 years should result in an even greater impact, with contributions to epidemiology, translational research, advocacy, education and clinical trials.
Educational questions
1. Which of the following statements regarding the EUCERD recommendations for rare disease registries is correct?
a. To ensure data quality, data entry to registries should always be performed by trained healthcare professionals and not directly by patients
b. Data quality in routine or electronic healthcare records is typically poor, and should not be integrated with registry data
c. Registries should be made available to perform feasibility studies for randomised controlled trials
d. European centres of excellence for rare or complex diseases do not have a responsibility to contribute to registries
e. Pooled analysis of data with registries outside of Europe is not permitted by data protection regulations
2. Which of the following statements regarding registry governance are correct?
a. There are no specific European/EU data protection requirements and so processes should be determined by requirements at national level on a case-by-case basis.
b. It is easier and more efficient to establish individual registries at national levels and then develop algorithms to integrate datasets than it is to have a single pan-European database
c. Centres participating in registries generally do not require funding for this activity
d. EUCERD guidelines suggest that industry should never be involved in registry governance
e. Data access procedures should be simple, and ensure that all relevant stakeholders can access data where it is in the public interest
3. Which of the following features have not been identified as determinants of bronchiectasis severity in EMBARC studies?
a. Post-infective aetiology
b. A history of rheumatoid arthritis
c. A history of three or more exacerbations per year
d. Chronic infection with P. aeruginosa
e. Low FEV1
4. Which of the following statements regarding bronchiectasis registries internationally is not correct
a. Pulmonary tuberculosis is an important underlying cause of bronchiectasis in India
b. Pulmonary NTM were isolated in >30% of patients in the USA bronchiectasis registry
c. The Australian registry incorporates data on indigenous Australians as this group has a high prevalence of bronchiectasis
d. COPD is a rarely reported comorbidity (<5%) in European patients with bronchiectasis
e. The finding that comorbidities predict mortality in the EMBARC dataset is likely to be a unique finding to Europe
Suggested answers
c. A key role of registries is to facilitate randomised controlled trials. EUCERD recommends that registries should establish methods to perform feasibility studies for randomised controlled trials.
e. EUCERD and other’s guidance related to registries emphasise the importance of making data available and disseminating results. Patients provide their data to the registry with the understanding it will be used for research and to improve clinical care. This mandates simple and open approaches to data sharing. There are specific EU data protection regulations that apply throughout the EU and must be followed for EU projects. It is highly complex and challenging to integrate different datasets compared to having a single core dataset with unified procedures. Again, this is a recommendation of EUCERD. Finally, industry involvement may be entirely relevant and appropriate for some registry projects and not appropriate for others, but EUCERD guidelines certainly do not forbid industry involvement in registries.
a. No evidence of long-term prognostic benefit or harm associated with post-infective aetiology has been reported. In contrast, all of the other four factors have been reported to be associated with higher mortality, increased rates of hospital admission or other adverse outcomes.
d. COPD is reported relatively frequently in European studies (10–50%) and in the most recent EMBARC data reports is reported in 15–20% of cases. It is also commonly reported in the USA and in all other territories where bronchiectasis data are available.
Disclosures
Supplementary Material
S. Aliberti EDU-0051-2017_Aliberti
J.D. Chalmers EDU-0051-2017_Chalmers
A. De Soyza EDU-0051-2017_De_Soyza
P.C. Goeminne EDU-0051-2017_Goeminne
C. Haworth EDU-0051-2017_Haworth
M.R. Loebinger EDU-0051-2017_Loebinger
Footnotes
Conflict of interest J. Boyd is an employee of the European Lung Foundation. All other disclosures can be found alongside this article at breathe.ersjournals.com
- Copyright ©ERS 2017
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










