





Figures
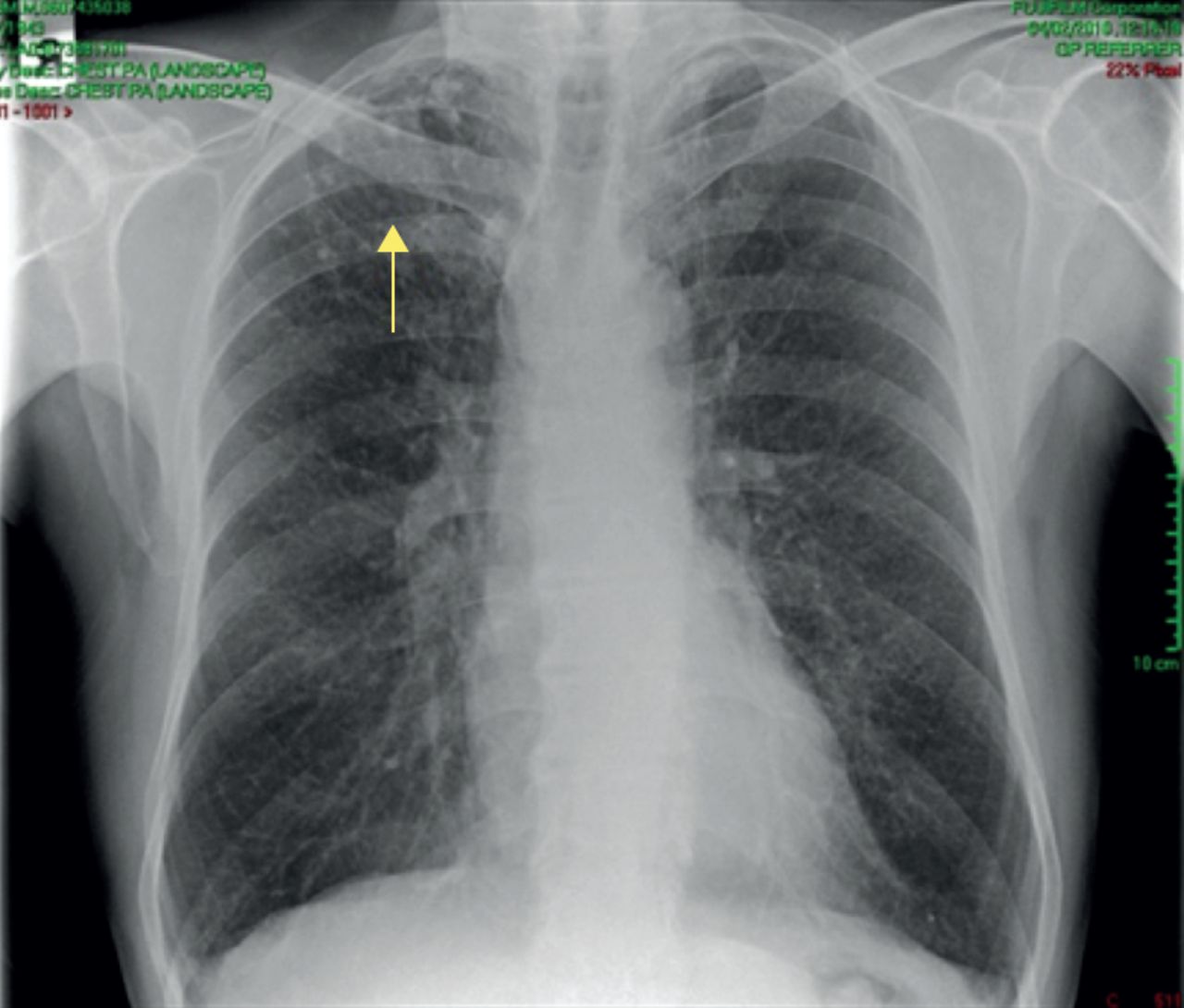
- Figure 1
Baseline chest radiograph, February 2010.
- Figure 2
Repeat chest radiograph in 2011.
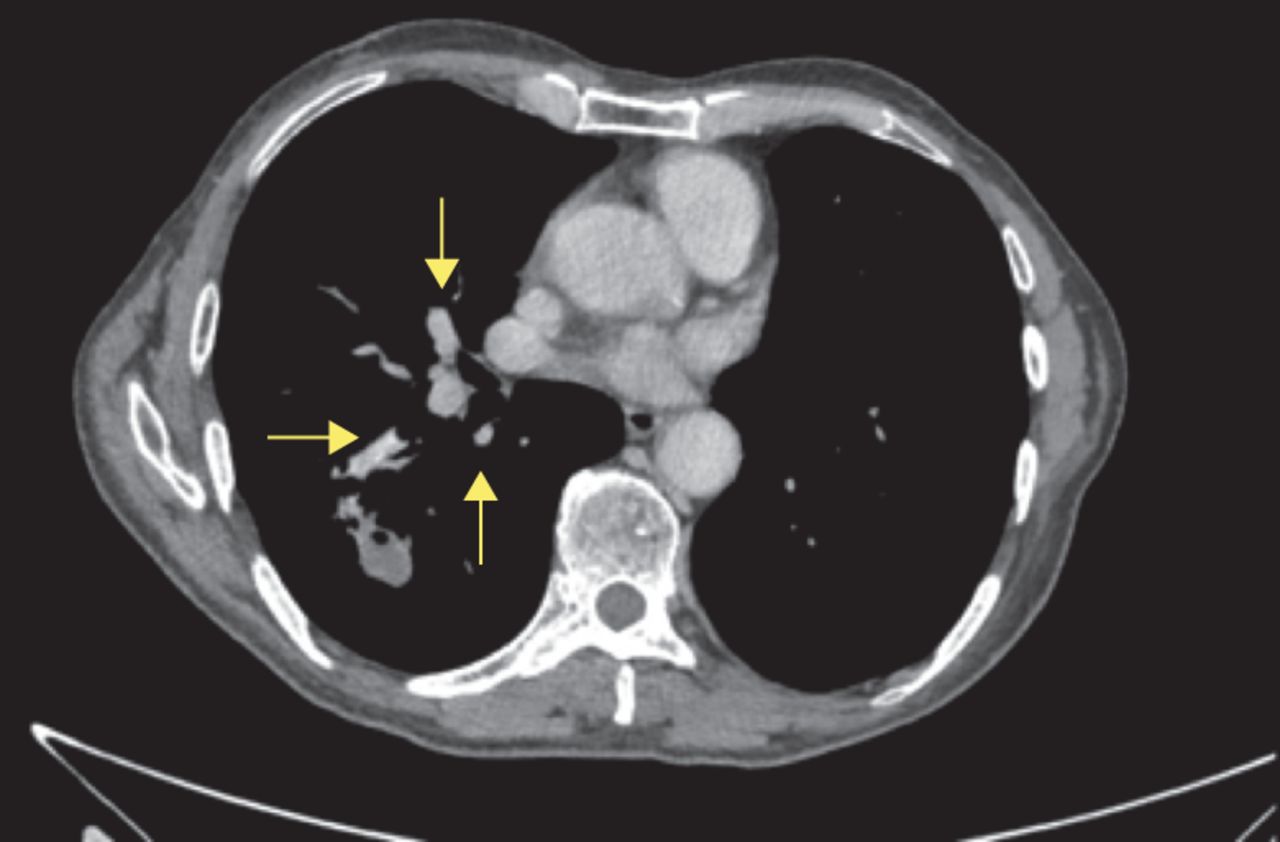
- Figure 3
CT scan, August 2011.
- Figure 4
Initial PET–CT scan showing “hot spots”.
- Figure 5
Post-lobectomy chest radiograph.
- Figure 6
a) Iron stain showing welder’s lung and various lung segments consistent with welder’s lung changes: fibrosis with carbon and iron pigment. b) Lung tissue with scarring, abundant histiocytes and multinucleated giant cells containing pigment both iron and carbon. The alveoli contain numerous macrophages and chronic inflammatory cells. At higher magnification, there is dystrophic calcification and ossification. c and d) Lymph nodes with a lot of pigment deposition but no evidence of malignancy.
- Figure 7
CT scan, September 2012. Several new lung masses can be seen. There is a cavitating soft tissue mass measuring 2.5×1.9 cm within the right lower lobe with adjacent consolidation and inflammatory changes. There is a further mass within the left upper lobe measuring 1.3 cm. No other sizeable intrapulmonary mass lesions are seen. A precarinal node measures 9 mm in the short axis. These are highly suggestive of malignancy.
- Figure 8
Follow up PET–CT scan.
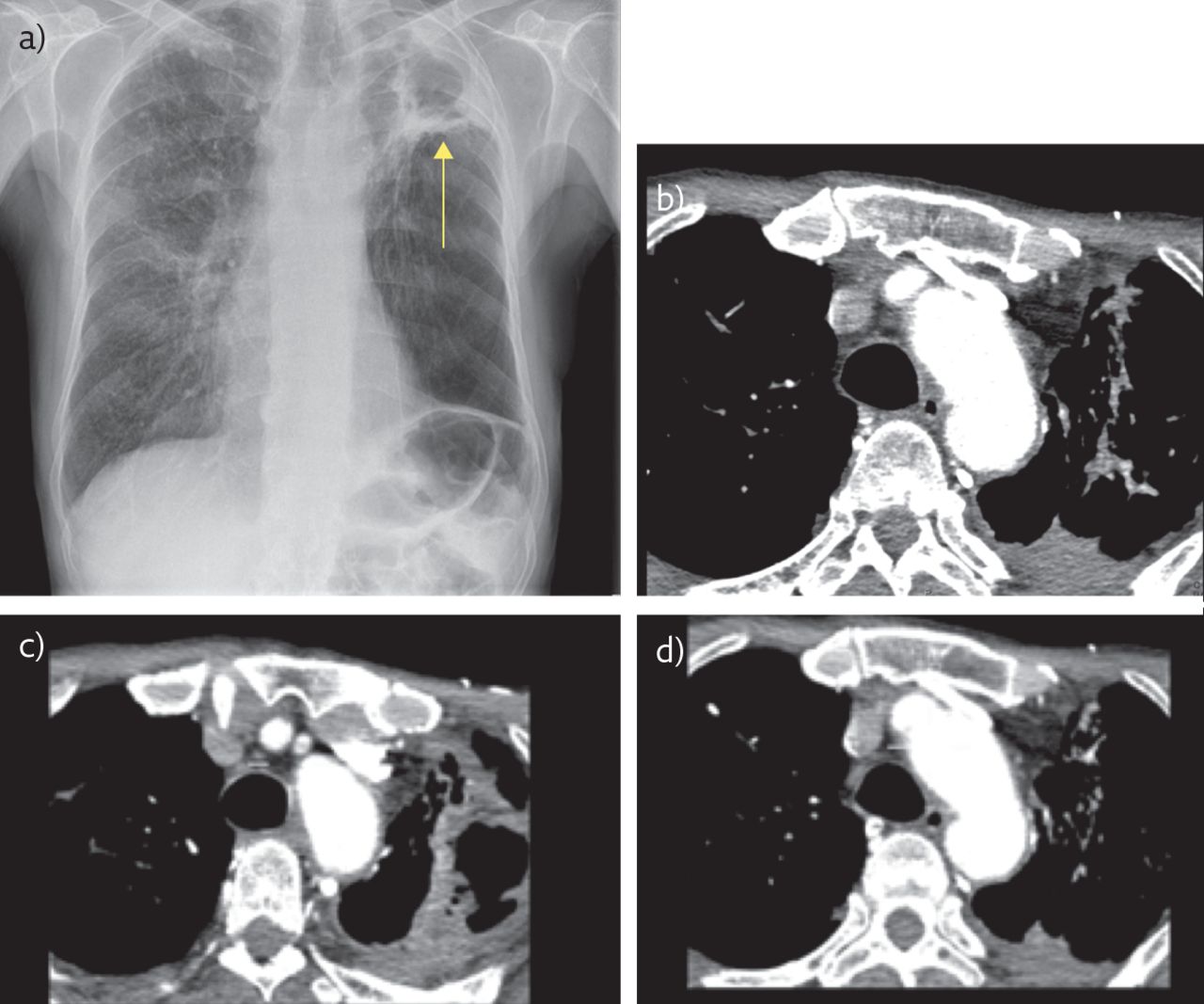
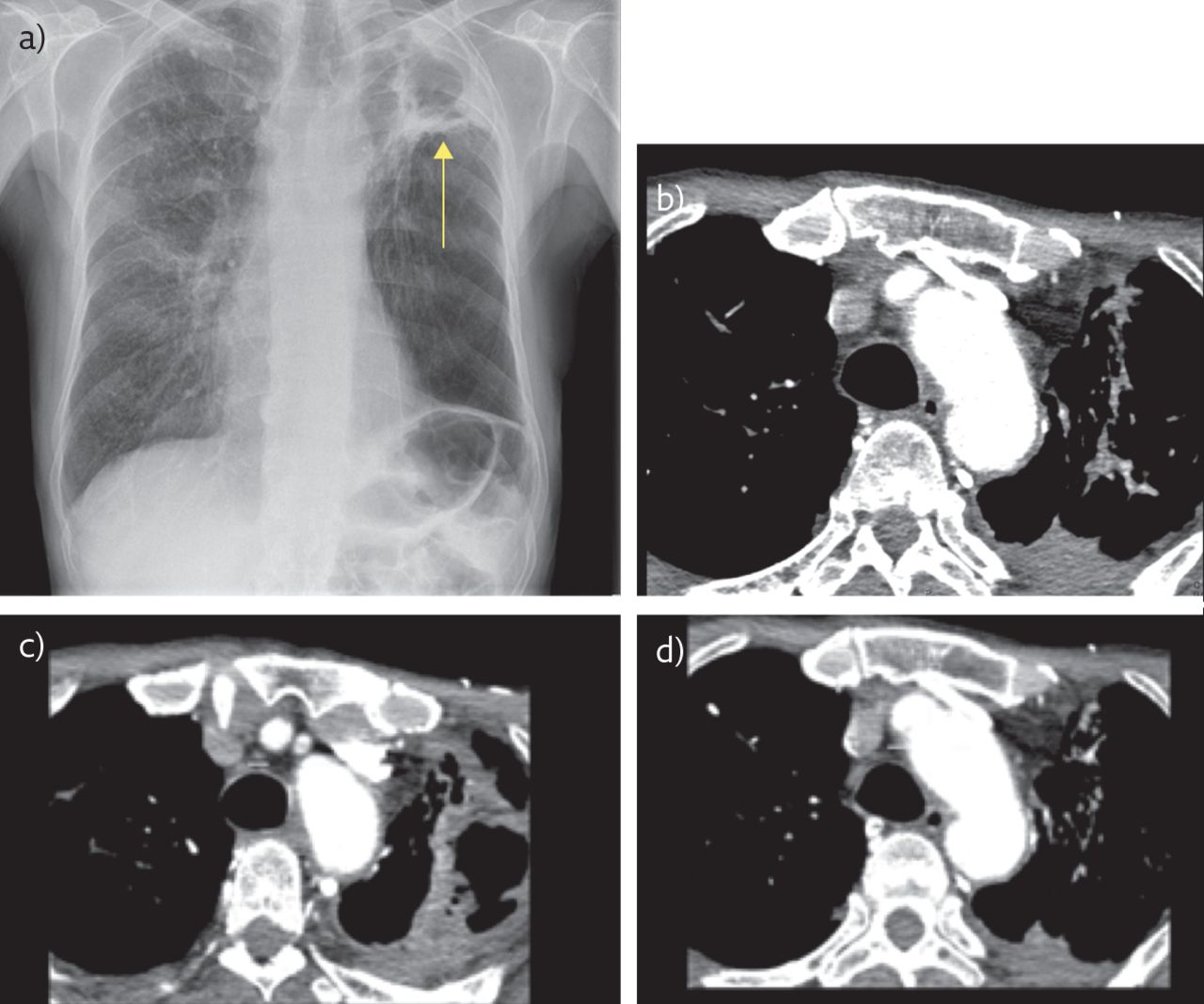
- Figure 9
a) Chest radiograph (2016) of the patient showing areas of old TB disease (arrow). b–d) Thoracic CT thorax snapshots showing areas of marked fibrosis.
- Figure 10
CT scan, June 2015. There is a thick-walled cavity in the left apex at the site of the previous bulla that incorporates the previously noted 1.5-cm soft tissue nodule.
- Figure 11
CT scan with contrast, 2016. A further increase in the cavitation in the left upper zone with marked related emphysema in the residual left lower lobe can be seen.
- Figure 12
CT scan, June 2105. A cavitating lesion can be seen in the right lobe.
- Figure 13
CT scan, October 2016. The lesion has now become a spiculated nodule.
- Figure 14
Latest chest radiograph.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}










