





Case 1
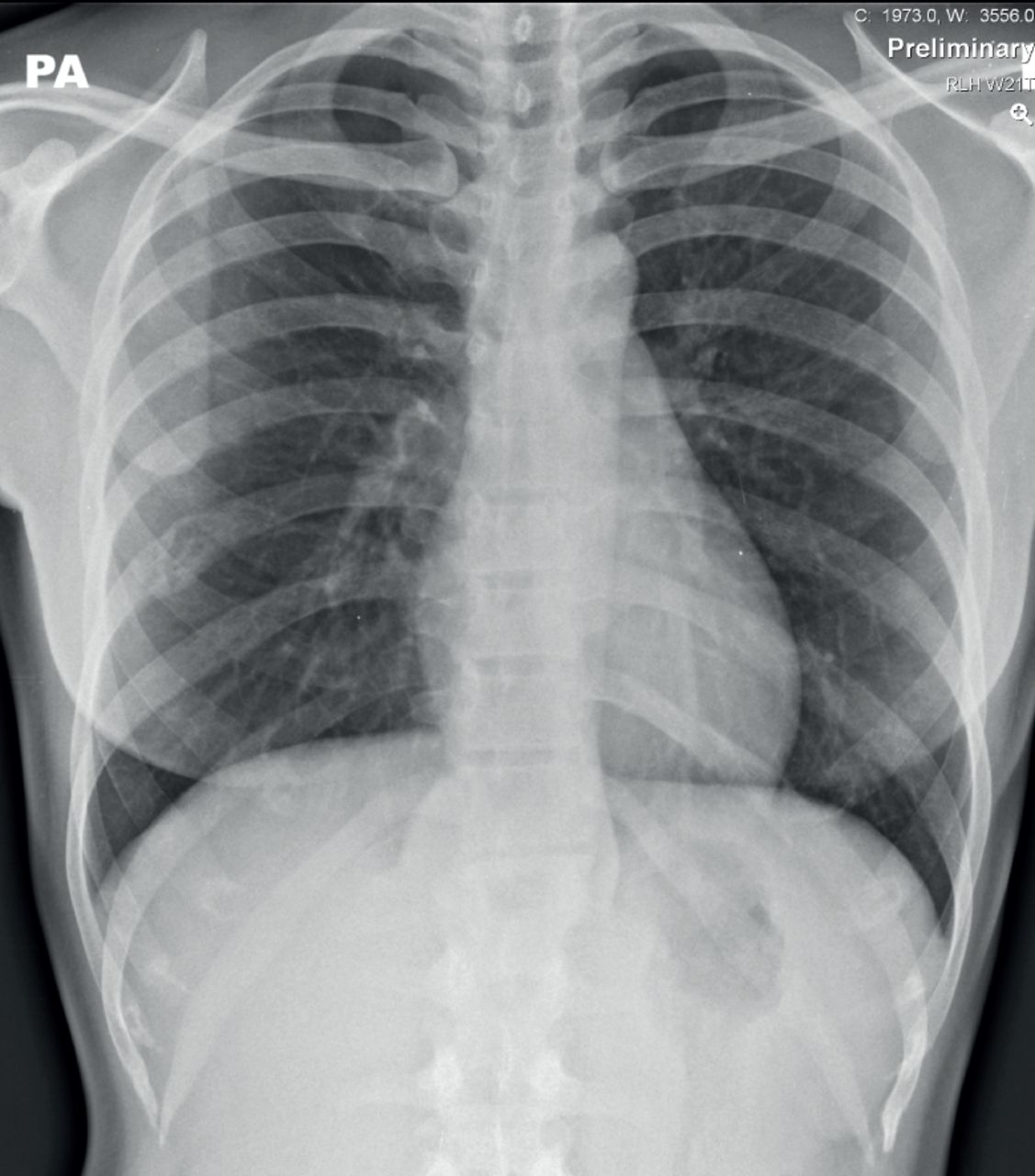
A 50-year-old male presents with chronic cough.
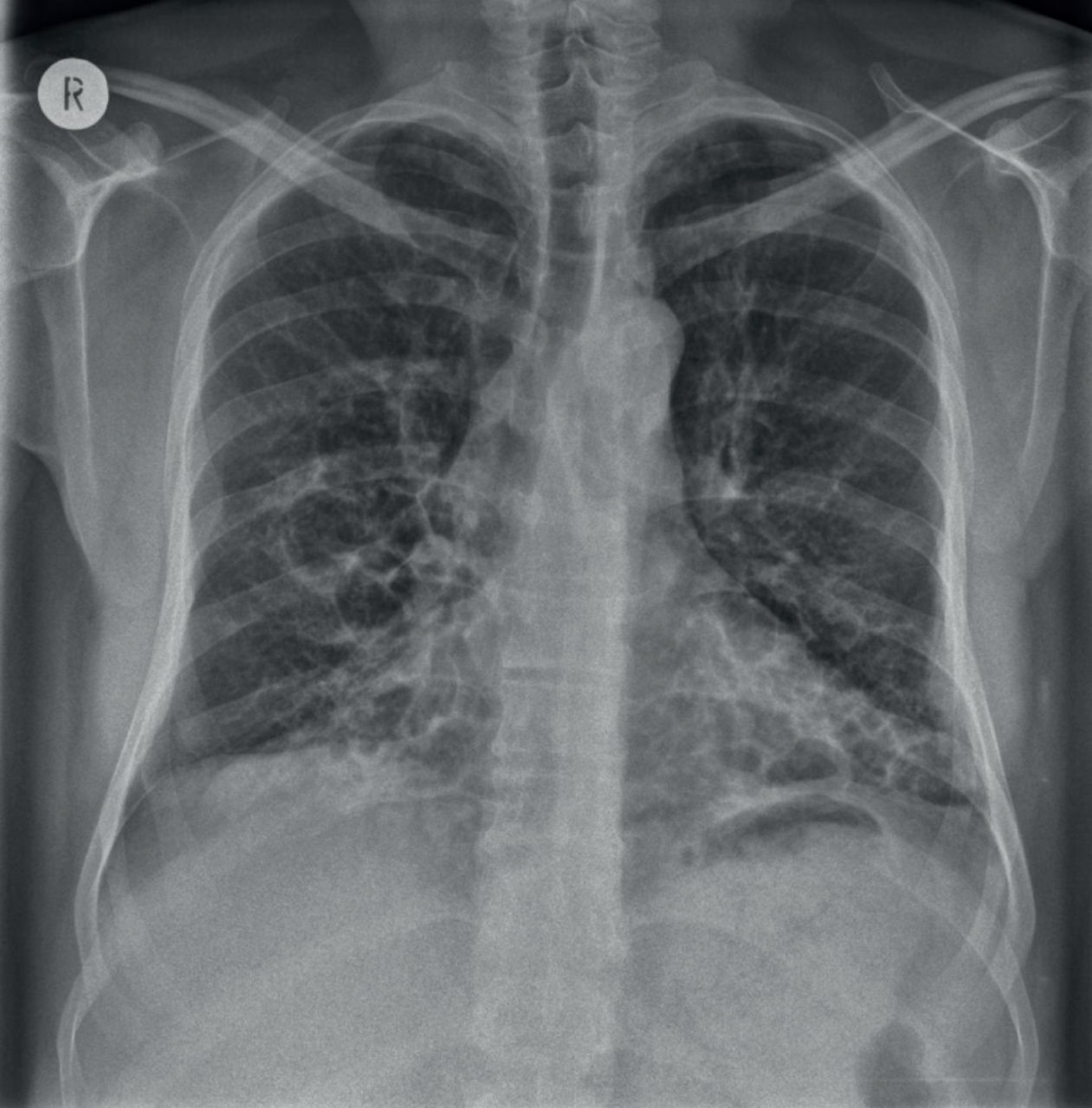
What is the main abnormality or underlying diagnosis?
a) Idiopathic pulmonary fibrosis
b) Cystic bronchiectasis
c) Pulmonary hypertension
d) Lymphangioleiomyomatosis
e) Cystic fibrosis
Case 2
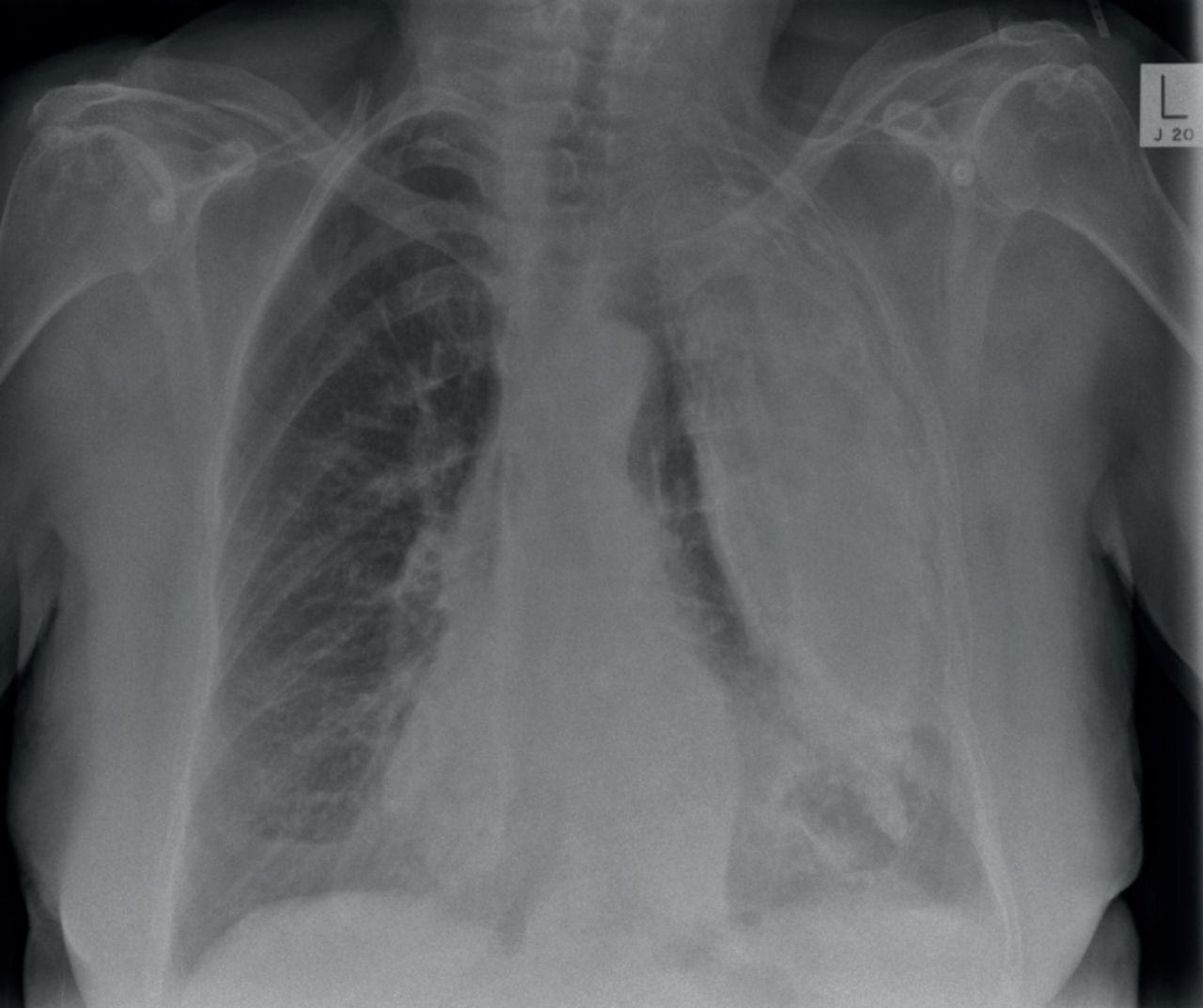
A 60-year-old male presents with haemoptysis and breathlessness.

What is the main abnormality?
a) Consolidation
b) Pleural abnormality
c) Post-radiotherapy change
d) Lobar collapse
e) Pulmonary fibrosis
Answers
Case 1
b) Cystic bronchiectasis. There is evidence of multiple cystic lucencies and thickened dilated airways predominantly within both lower zones. Marked bronchiectasis also occurs with advanced cystic fibrosis, but the distribution in such cases is usually more widespread and upper zone predominant. The distribution of chest radiograph abnormalities with idiopathic pulmonary fibrosis is peripheral and basal. In this case, the costophrenic angles are spared.
This patient had cystic bronchiectasis, which had developed due to a severe childhood infection.
Case 2

d) Lobar collapse. There is right upper lobe collapse due to a central obstructing bronchogenic carcinoma.
Note the dense opacification at the right apex with evidence of volume loss with tracheal deviation to the right and elevation of the right hilum. The right hilum also has an abnormal lobulated outline due to a central right hilar mass. This is called “Golden's S sign”. When the right upper lobe collapses the horizontal fissure is elevated and would normally have a straight margin when caused by a mucous plug or inhaled foreign body. The central bulge, as seen when the “Golden's S sign” is present, indicates the presence of a central obstructing mass lesion.
Case 3
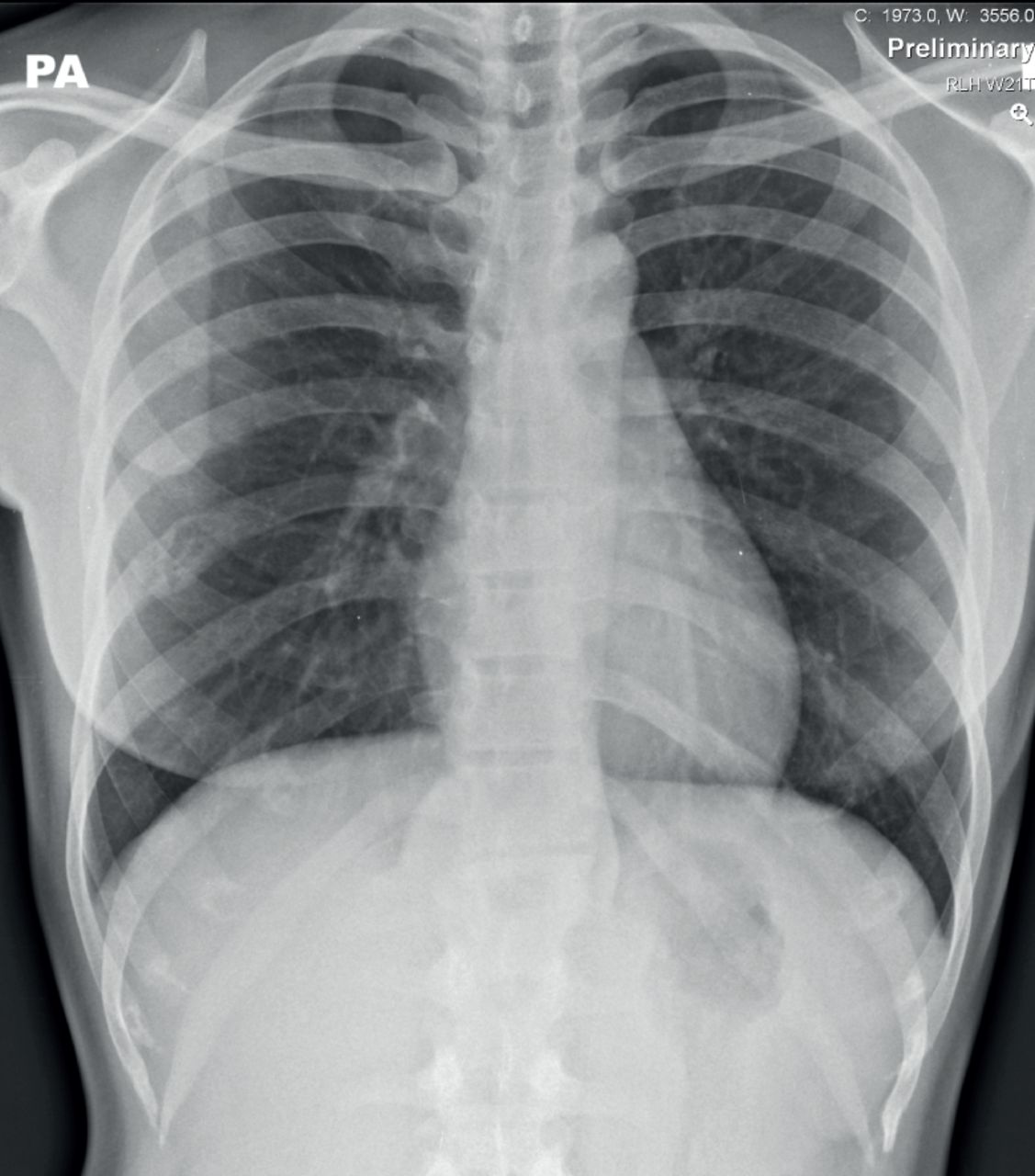
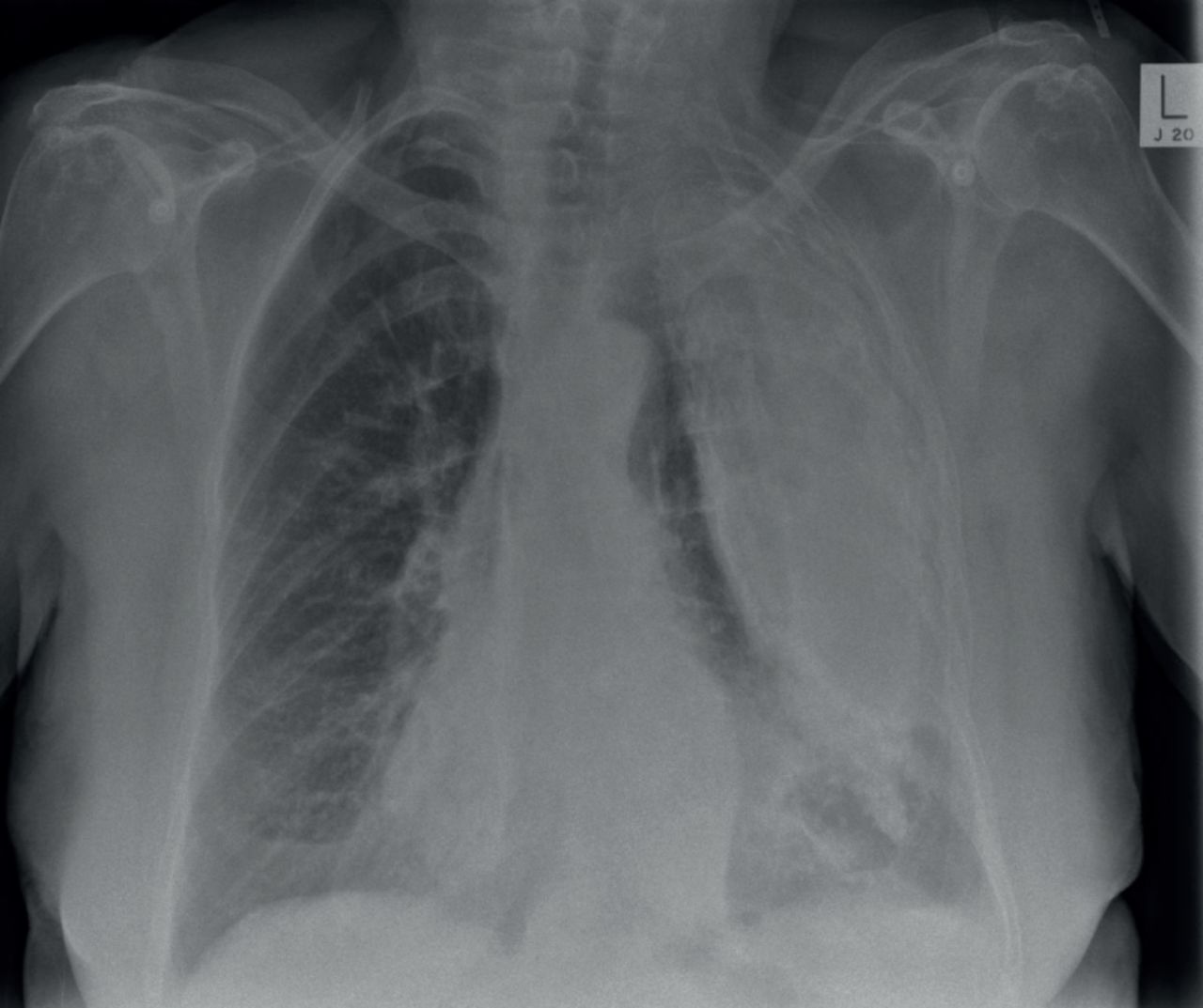
A 63-year-old female presents with shortness of breath on exertion.
Which of the following is the least likely cause for these appearances?
a) Previous tuberculosis
b) Previous trauma
c) Previous empyema
d) Past asbestos exposure
Case 4
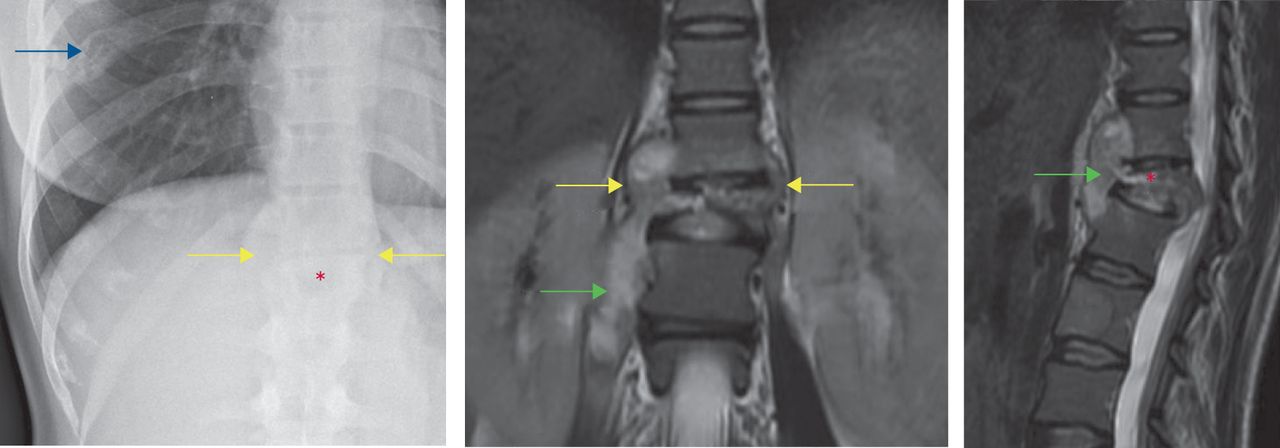
A 29-year-old female presents with night sweats and unexplained weight loss.
What are the main abnormalities?
a) Lung parenchymal and bony abnormalities
b) Paravertebral and bony abnormalities
c) Lung parenchymal and paravertebral abnormalities
d) Paravertebral and pleural abnormalities
e) Bony and pleural abnormalities
What is the most appropriate radiological investigation to perform next?
a) Magnetic resonance imaging
b) Dedicated plain radiographs
c) Computed tomography
d) Ultrasound
e) Repeat chest radiograph in 4–6 weeks following treatment
Answers
Case 3
d) Past asbestos exposure. There is extensive left-sided pleurally based abnormality with calcification. In this case it was due to previous tuberculosis. Calcified pleural plaques due to asbestos exposure are usually bilateral and reasonably symmetrical. Past asbestos exposure is the least likely of the options provided to cause this dense unilateral pattern.
The general differential diagnosis for pleural calcification would include: previous haemothorax; previous empyema; tuberculosis; osteosarcoma of the pleura (rare); previous talc pleurodesis (not true calcification); and pleural plaques due to asbestos exposure.
Case 4
b) Paravertebral and bony abnormalities. There is evidence of widening of both right and left paraspinal lines (yellow arrows in the figure), which correspond with the magnetic resonance images. Note the loss of height of the L1 vertebra, which may be appreciated on the plain radiograph but is well depicted on the coronal and sagittal T2 magnetic resonance images (red asterisk). These findings were due to tuberculosis infection and note the presence of the paraspinal abscess on the magnetic resonance images (green arrow in the figure).
On the plain radiograph also note the lucent abnormality centred on the right-sided eighth rib that wasn't present on a previous radiograph 3 months earlier and is suspected to represent a further focus of infection.
a) Magnetic resonance imaging would be the next appropriate radiological investigation as shown in the figure. It is the best way of assessing the spine and potential spinal canal encroachment.

- Copyright ©ERS 2018
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}