





Abstract
Doubling time, clinical prediction models of malignancy and positive bronchus sign are useful in stepwise evaluation of SPN to avoid thoracotomy. GeneXpert can be used as initial diagnostic test for tuberculosis and detection of rifampicin resistance.
http://ow.ly/N37030mB8Fi
A 54-year-old, nonsmoking woman was referred for a solitary pulmonary nodule (SPN) discovered during her routine preoperative pulmonary evaluation prior to right total knee replacement surgery. She had no respiratory symptoms. Around 4 months ago she had undergone a left total knee replacement surgery. She had a SPN at that time as well, but the radiologist erroneously reported it normal. So, she did not undergo any evaluation 4 months ago. She had diabetes mellitus and was on regular oral treatment. She denied prior history of antitubercular drug intake or any other chronic disease. There was no significant family history of respiratory disease or malignancy.
On physical examination, her pulse rate, respiratory rate, blood pressure and oxygen saturation were 90 per min, 16 per min, 110/70 mmHg and 98%, respectively. The respiratory system examination was unremarkable. The routine investigations performed for preoperative evaluation showed haemoglobin of 10.7 g·dL−1 with normal total and differential leukocyte counts. Her serum urea was 33 mg·dL−1, creatinine was 1.1 mg·dL−1 and HbA1c level was 6.6%. The enzyme-linked immunosorbent assay for HIV was negative.
The radiograph performed ∼4 months ago and the one with which she was referred for preoperative pulmonary evaluation are shown in figure 1a and b, respectively. Both the radiographs have a SPN in the right upper zone. On comparing both the radiographs, we observed that the nodule had grown in size in 130 days from 1.8×1.8 cm to 2.3×2.3 cm.

Chest radiograph in posteroanterior projection: a) initial and b) after 130 days at the time of presentation.
Task 1
What was the doubling time of the SPN in the given case?
a) 120 days
b) 133 days
c) 123 days
d) 113 days
Answer 1
c) 123 days
The doubling time of the SPN can be calculated by using the following formula.
Doubling time in days=(t×log 2)/(3×log (d2/d1)) [1], where t is the number of days between the radiographs. The “t” in this case was 130 days. d1 and d2 are the diameters of the nodule on the initial and follow-up radiographs, which were 1.8 cm and 2.3 cm, respectively.
The evaluation of an incidental SPN begins with the assessment of the probability of malignancy. Clinical parameters that favour malignant aetiology include older age, positive smoking history, female sex and prior history of malignancy. The malignant potential can also be evaluated by the growth rate or doubling time. An average doubling time for a malignant tumour is 120 days and ranges from 30 to 400 days. Infection, infarction and lymphoma usually grow faster, whereas benign lesions usually grow slower. There are however exceptions to the rule, e.g. small cell carcinoma may double in <30 days and bronchoalveolar carcinoma may grow more slowly [2–4]. However, a doubling time between 30 and 400 days definitely requires further investigation.
A high-resolution computed tomography (CT) scan of chest is useful in evaluating the details of the SPN. The various imaging characteristics on the chest radiograph and CT scan that can help in distinguishing a benign from a malignant nodule include size of the nodule, margins of the nodule, presence of calcification and cavitation. The probability of malignancy increases with increasing size of the nodule, spiculated margins and the presence of an irregular thick-walled cavity. The presence of calcification usually suggests a benign lesion, except for patterns like eccentric and speckled calcification which are seen in malignant SPN. The CT scan of our patient is shown in figure 2. The CT showed the presence of a soft tissue density solid nodule of 2.3×2.2×2.0 cm in size in the posterior segment of the right upper lobe, with regular margins and no contrast enhancement. It did not have any cavitation, calcification or satellite nodules.
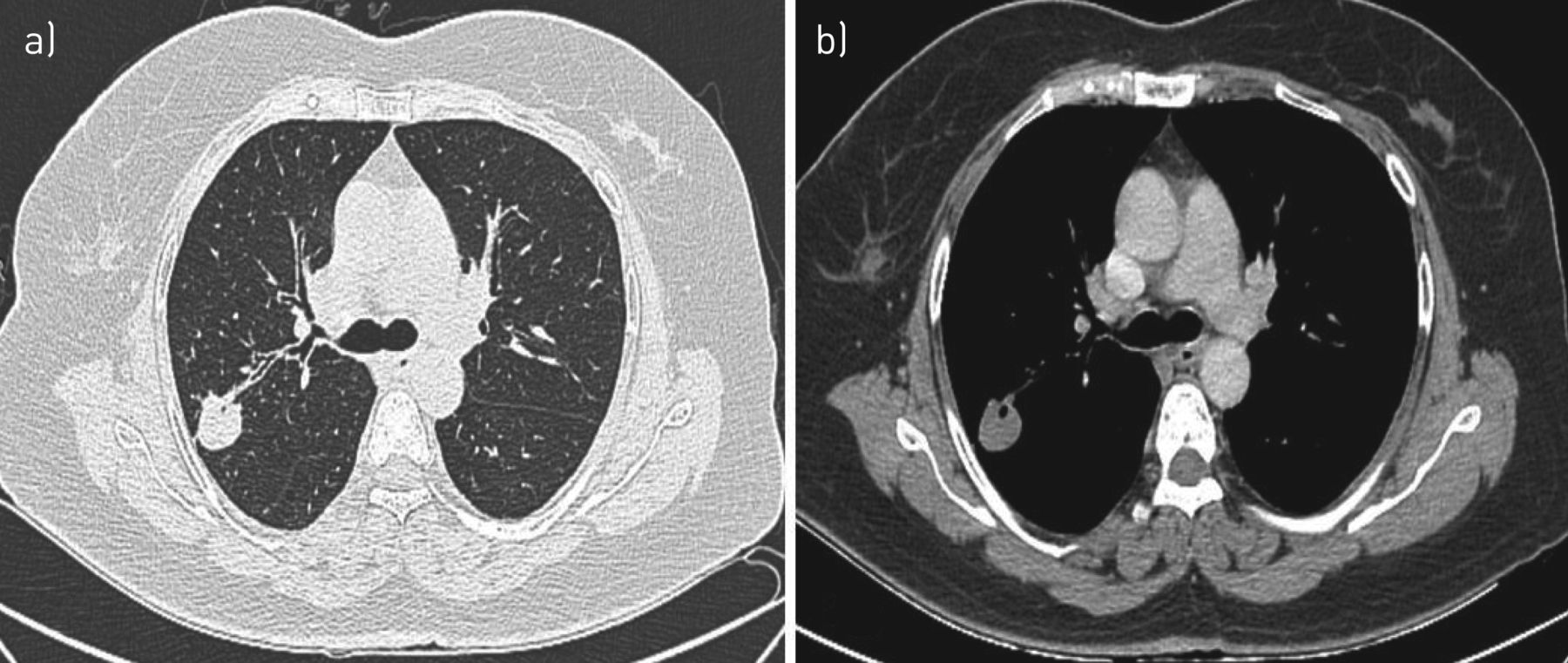
CT image: a) lung window and b) mediastinal window.
Once the characteristics of the SPN are ascertained, the probability of malignancy is estimated using clinical judgement, imaging characteristics or by quantitative assessment using a validated prediction model [5, 6]. There are various clinical prediction models for predicting malignancy in SPN, of which the Mayo Clinic model [7], the Veteran's Affairs cooperative clinical model [8], the Peking University model [9] and the Pan-Canadian Early Detection of Lung Cancer (Brock University) model [10] are well known. All of them have a variable predictive accuracy depending on the study population characteristics and local prevalence of malignancy. There are no recommendations about which model is appropriate for a specific population. Zhang et al. [11] compared three prediction models (the Mayo Clinic, Veteran's Affairs cooperative clinical model and Peking University models) and found that all three have similar predictive accuracy.
Task 2
What is the pretest probability of cancer in this case using the Mayo Clinic model?
a) 16%
b) 27%
c) 54%
d) 72%
Answer 2
b) 27%
The pretest probability of cancer using the Mayo Clinic model [7] is defined by the equation:
Probability of malignant SPN = ex/(1+ex)
Where:
x = −6.8272 + (0.0391 × age) + (0.7917 × smoking history) + (1.3388 × cancer history) + (0.1274 × diameter) + (1.0407 × spiculation) + (0.7838 × upper lobe)
e is the natural logarithm, and a value of 1 for “yes” and 0 for “no” is given in the smoking history, cancer history, spiculation and upper lobe elements. Diameter indicates the largest nodule measurement (in mm) on the chest radiograph or CT scan.
The pretest probability of malignancy is useful in deciding further management strategies. When the pretest probability of malignancy is low (<5%), the patient needs serial CT surveillance. If the probability is moderate, i.e. 5–60%, the patient needs further evaluation with functional imaging, preferably a positron emission tomography (PET) scan. If the nodule on PET scan is hypermetabolic, then a nonsurgical biopsy is advised. In some circumstances with moderate probability (5–60%), the nonsurgical biopsy is preferred over a PET scan based on other clinicoradiological parameters (discussed further on in this case report). Nonsurgical biopsy procedures include: CT-guided transthoracic biopsy, transbronchial lung biopsy under fluoroscopic guidance, radial probe endobronchial ultrasound, electromagnetic navigational bronchoscopy (ENB) and virtual bronchoscopic navigation. The decision regarding the type of biopsy is based on the radiological characteristics (size, location and relationship to airways), potential risk of complications and expertise of the practitioners [6]. In cases with a high probability of malignancy (>60%) direct surgical biopsy is advised. The surgical biopsy can be via open thoracotomy or thoracoscopic wedge resection.
Our patient had a moderate probability of cancer and a decision regarding PET versus nonsurgical biopsy was required. The chest CT, however, showed an important sign which was useful in deciding the next course of action.
Task 3
What is the radiographic sign seen on the chest CT?
a) Tumour bronchus sign
b) Positive bronchus sign
c) Feeding vessel sign
d) Tsuboi sign
Answer 3
b) Positive bronchus sign
A positive bronchus sign is a radiological finding described on a CT scan where a hypoattenuating tube (bronchus) leads directly to a lung lesion.
The anatomical relationship between a peripheral lung nodule or mass with the adjacent bronchi was initially studied by Tsuboi et al. [12]. They performed transbronchial biopsy with a specially designed curet introduced directly into the lesion through a bronchial catheter under fluoroscopic guidance. They described four types of tumour–bronchi relationships: 1) the bronchial lumen is patent up to the tumour; 2) the bronchus is contained within the tumour; 3) the bronchus is compressed and narrowed by the tumour but the mucosa is intact; and 4) the proximal bronchial tree is involved by peribronchial or submucosal spread of the tumour or by the enlarged nodes along with narrowing of the proximal bronchial tree (figure 3).
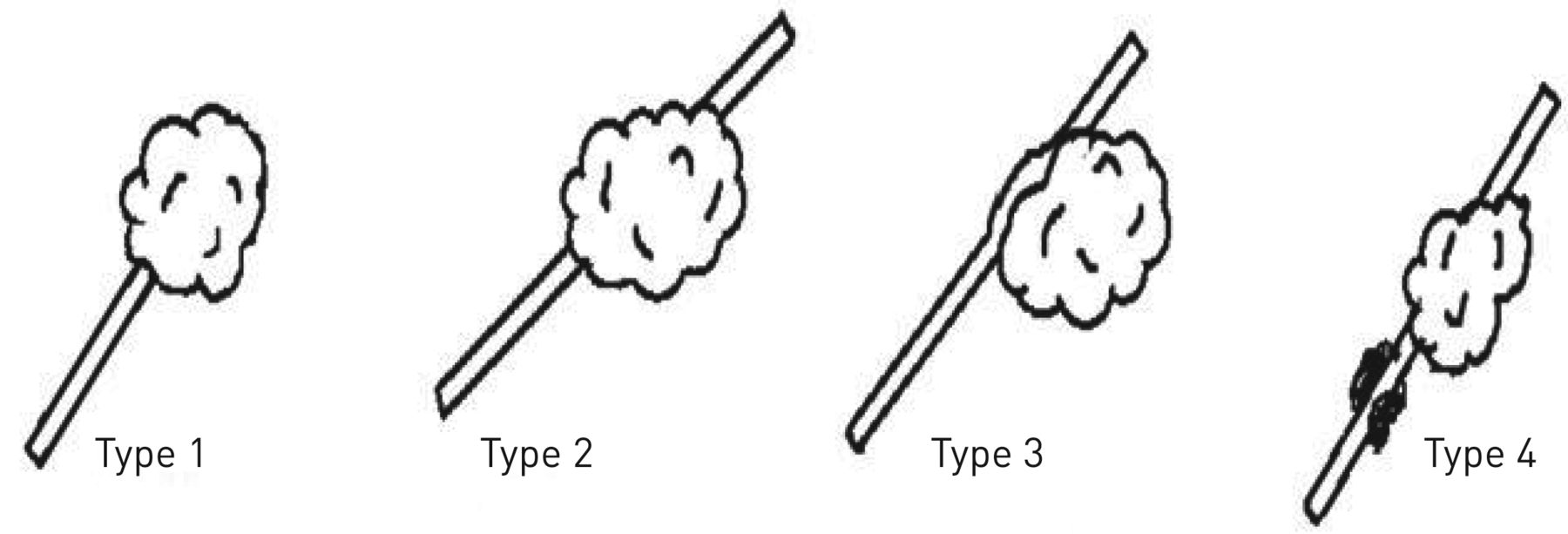
Relationship between the tumour mass and the bronchus, as described by Tsuboi et al. [12]. Details of the four types of relationship are described in the text.
The presence of type 1 and 2, i.e. a bronchus leading to or contained within the nodule or mass on CT, is termed as “positive bronchus sign”.
Task 4
Which of the following next line of investigations will be most helpful in this case?
a) PET-CT scan
b) CT-guided lung biopsy
c) Bronchoscopy/radial probe endobronchial ultrasound-guided biopsy with lavage for acid-fast bacilli (AFB) and GeneXpert MTB/RIF assay
d) Bronchoscopy/linear probe endobronchial ultrasound-guided biopsy with lavage for AFB and GeneXpert MTB/RIF assay
e) Bronchoscopy/radial probe endobronchial ultrasound-guided biopsy
Answer 4
c) Bronchoscopy/radial probe endobronchial ultrasound-guided biopsy with lavage for AFB and GeneXpert MTB/RIF assay
In developed countries, for a new solid SPN with moderate probability of cancer, the PET scan is the primary investigation, but it has its limitations in countries with a high incidence of infectious diseases such as Asian and African countries. It lacks specificity in glucose uptake to distinguish inflammatory disease from cancer. Also, the PET scan has limited accessibility and is not cost-effective in some countries [6, 13]. Thus, in countries with high incidence of infectious and inflammatory diseases, the next step is focused on obtaining a tissue diagnosis rather than a PET scan [6, 13]. The nonsurgical biopsy techniques are preferred over surgical biopsy in patients with moderate probability of cancer, i.e. our patient. Of the nonsurgical techniques described previously, SPN with a positive bronchus sign is accessed using bronchoscopy rather than CT-guided biopsy as the positive bronchus sign is associated with 60% to 90% yield on bronchoscopy [1, 14]. The bronchoscopic biopsy can be performed with bronchoscopy under fluoroscopic guidance or via radial probe endobronchial ultrasound. The radial probe endobronchial ultrasound helps with better access to a peripheral SPN. However, considering its limited availability and high cost, simple bronchoscopy can be considered as an alternative in resource limited settings. Hence, bronchoscopy or radial probe endobronchial ultrasound-guided biopsy is the next choice of investigation in this case.
Further, for a SPN in an Asian country with a high rate of tuberculosis (TB) (∼981 per 100 000 population) a search for AFB is required [13]. This includes induced sputum, bronchoscopic lavage and in patients with enlarged lymph nodes endobronchial ultrasound or endo-oesophageal ultrasound. Since this patient was asymptomatic and did not produce sputum and there were no mediastinal lymph nodes, bronchoscopic lavage for identifying AFB was an ideal additional investigation in this case. The newer, rapid test for identifying the bacilli, i.e. the GeneXpert MTB/RIF assay, is a very useful investigation because of its very high sensitivity and specificity in bronchial washings or bronchoalveolar lavage fluid [15, 16].
She underwent bronchoscopy, which was normal with no evidence of an endobronchial lesion. A transbronchial biopsy was taken from the right upper lobe posterior segment and sent for histopathology. Bronchial washings were negative for malignant cells. The biopsy specimen on histopathology showed septal thickening, haemorrhage and mild pigment deposition along with normal bronchial epithelium. No conclusive pathology could be seen. Bronchial washings were also sent for AFB and GeneXpert for Mycobacterium tuberculosis. The lavage for AFB was negative. But, the GeneXpert on bronchial washings detected the presence of M. tuberculosis with rifampicin resistance. The SPN with positive bronchus sign was finally proven to be a drug-resistant tuberculoma.
Task 5
What is the role of the GeneXpert MTB/RIF assay in the diagnosis of pulmonary TB and rifampicin resistance?
a) GeneXpert is useful neither for the diagnosis of TB nor for the detection of drug resistance
b) GeneXpert can be used for the diagnosis of TB but it doesn't reliably detect drug resistance; drug-resistant TB can be diagnosed based on phenotypic culture methods only
c) GeneXpert can only be performed for detection of drug resistance in suspected drug-resistant cases but not as the initial diagnostic test
d) GeneXpert can be used as the initial diagnostic test for the diagnosis of TB as well as for detection of rifampicin resistance
Answer 5
d) GeneXpert can be used as the initial diagnostic test for the diagnosis of TB as well as for detection of rifampicin resistance
The diagnosis of smear-negative pulmonary TB, which represent the majority of TB cases is a major concern. In such cases the genotypic tests as compared with conventional culture methods, have the added advantage of detecting TB as well as drug resistance in less time. The GeneXpert MTB/RIF assay is a rapid, automated cartridge-based molecular technique which simultaneously detects M. tuberculosis and rifampicin resistance within 2 h. It was first endorsed by the World Health Organization (WHO) in 2011 for the initial diagnosis of TB in cases with a high risk of drug resistance. The guidelines also advised its use as a follow-up test to microscopy, especially in smear-negative specimens (conditional recommendation) [17]. Gradually this was scaled up to include testing in all cases of suspected TB as the initial diagnostic test [18]. GeneXpert is also recommended for detecting rifampicin resistance by WHO over conventional testing or no testing at the time of diagnosis [19]. GeneXpert reliably detects rifampicin resistance with a specificity of 99% and a negative result rules out rifampicin resistance. WHO also recommends starting drug-resistant treatment in case of a positive result based on GeneXpert [17, 18].
Our patient was advised treatment for drug-resistant TB. However, the patient refused to accept the diagnosis of resistant TB and did not agree to start second-line treatment. She was thus started on first-line anti-tubercular therapy. She became symptomatic. The CT scan showed cavitation and consolidation around the lesion after 2 months (figure 4). She was proven to be a case of multidrug-resistant TB and was referred to a drug-resistant TB centre for the management.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow-up CT scan of the chest after 2 months of first-line anti-tubercular therapy.
Discussion
A SPN is defined as a single, spherical, well-circumscribed radiographic opacity of up to 3 cm in diameter surrounded by aerated lung, not associated with adenopathy, atelectasis or effusion [1, 20]. On imaging studies, a SPN is found incidentally in 0.09–0.2% of all chest radiographs [21].
The differential diagnoses of SPN are wide and variable for solid and subsolid nodules. The aetiology of solid SPNs are malignant neoplasms like primary lung cancer, solitary metastases and benign lesions such as hamartomas, congenital lesions, infectious and non-infectious granulomas. Subsolid nodules may be due to infection, inflammation, haemorrhage and malignancy, specifically lung adenocarcinoma [4]. All SPNs need appropriate work-up in order to achieve diagnosis. In our case although the patient was asymptomatic, the nodule had a doubling time of 123 days. It warranted further evaluation. The finding of a positive bronchus sign on CT and moderate probability of cancer prompted bronchoscopy. The comorbidity of diabetes and high prevalence for TB incited us to actively search for TB bacilli in the bronchoscopic sample, which led to the diagnosis of TB.
Positive bronchus sign has been commonly reported in malignant lesions; however, in our case it was associated with a benign lesion of tuberculoma. To the best of our knowledge there is no previous case report of TB presenting as a SPN with positive bronchus sign, although TB often mimics malignancy clinically as well as radiologically posing many diagnostic challenges. Pitlik et al. [22] reported 26 cases with a presumptive diagnosis of neoplasm that were bacteriologically proven to be TB. Chawalparit et al. [23] found that CT features of malignancy and pulmonary TB can be similar and there is no conclusive finding as a potential predictive factor for TB. Such cases are difficult to differentiate from lung cancer because AFB are often negative on routine bacteriological examinations, as observed in our case. GeneXpert MTB/RIF assay of bronchoscopic samples has emerged as a useful investigation in the past decade and should be used optimally in suspected cases.
Conclusion
A stepwise approach to SPNs is useful in achieving diagnosis and avoiding thoracotomy. In rare cases a positive bronchus sign can be associated with benign lesions such as tuberculoma. GeneXpert MTB/RIF assay can be relied on as a useful adjunctive investigation for the diagnosis of TB even in cases of SPN where the bacillary load is very low.
Footnotes
Conflict of interest: M. Patro has nothing to disclose.
Conflict of interest: D. Gothi has nothing to disclose.
Conflict of interest: R.B. Sah has nothing to disclose.
Conflict of interest: S. Vaidya has nothing to disclose.
- Copyright ©ERS 2019
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










