





Abstract
Pleural effusions are associated with various aetiologies: systematic evaluation is needed to reach a correct diagnosis. In 20% of cases the aetiology of exudative pleural effusion is elusive and pleural biopsy is required to reach a diagnosis. http://bit.ly/2HyZGVZ
Pleural disease is a common respiratory condition affecting ∼3000 people per million population annually [1]. Pleural effusion has multiple underlying aetiological conditions and therefore requires a systematic assessment to reach a final diagnosis. Despite detailed evaluation, there may be situations, where the aetiology of a pleural effusion remains unknown [2]. Various experts have suggested a step-wise approach in the management of these undiagnosed pleural effusions [3]. The role of detailed history, proper clinical examination and appropriate investigations, including computed tomography (CT) of chest and pleural biopsy, in an attempt to establish the correct cause of pleural effusion cannot be overemphasised. We present an interesting case of pleural effusion that was managed at our institute.
Case presentation
A 52-year-old woman, who was a native of Bahrain, presented to our hospital with intermittent low-grade fever, dry cough and exertional dyspnoea of 3 weeks duration. She denied orthopnoea or paroxysmal nocturnal dyspnoea, wheeze, chest pain and haemoptysis. There was no anorexia or weight loss. There was no swelling of the lower extremities, palpitations or syncopal episodes. She had had gastro-oesophageal reflux disease for the past 10 years. She was also suffering from osteoarthritis in both knees and had undergone knee replacement surgery 1 year earlier. There was no history of other comorbidities such as hypertension, diabetes or heart diseases. She was a home-maker and was a nonsmoker. There was no history of food or drug allergies. There was no history of drug abuse.
On examination, her temperature was 36.7°C, pulse rate was 115 beats·min−1, respiratory rate was 20 breaths·min−1, blood pressure was 187/98 mmHg and arterial oxygen saturation measured by pulse oximetry was 97% on room air. There was no pallor, clubbing, pedal oedema, icterus or lymphadenopathy. The breath sounds were absent in the infra-scapular, infra-axillary and mammary areas on the right side. No adventitious sounds were heard on either side of the chest. Examination of the other systems was unremarkable.
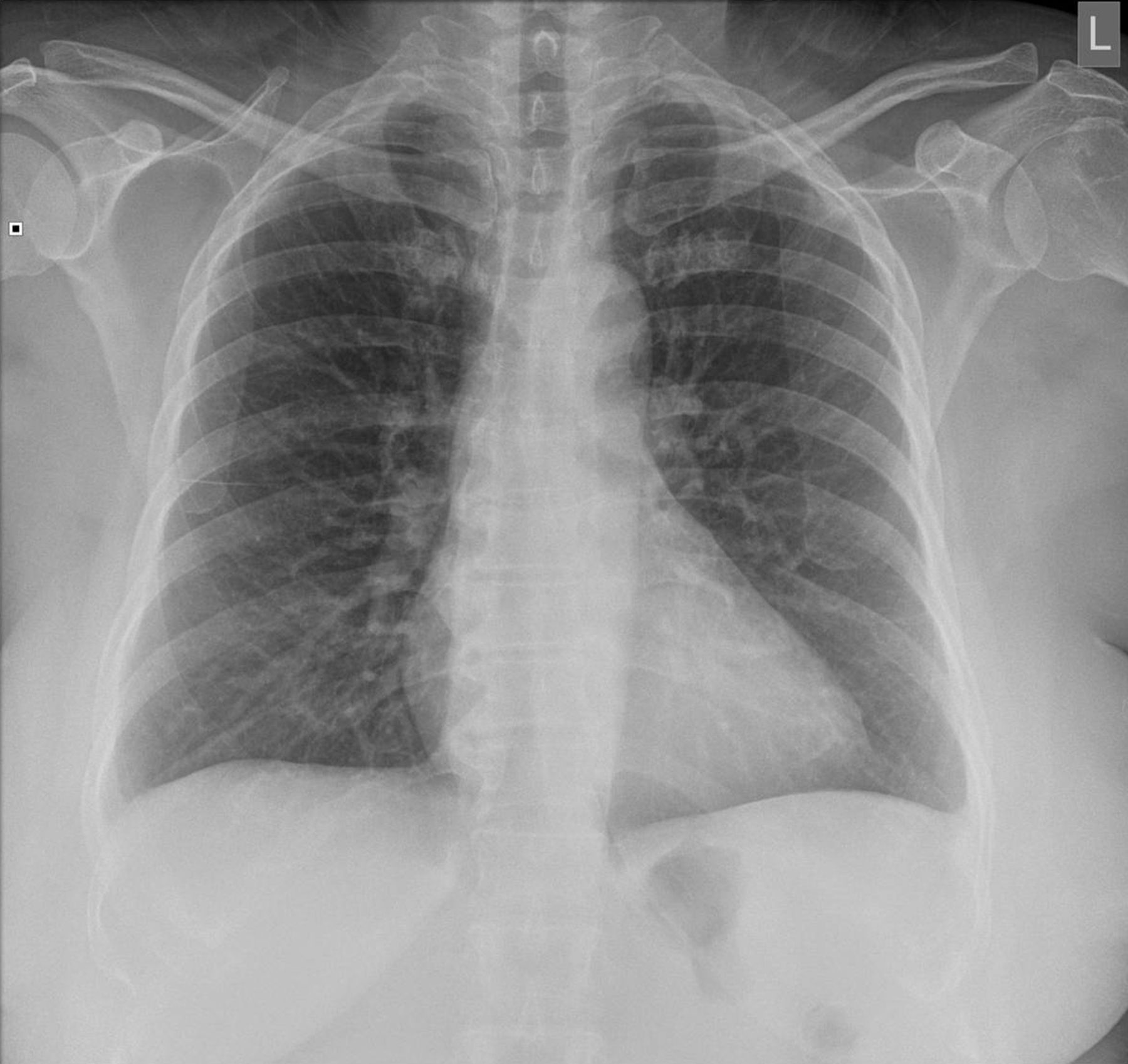
A complete blood count revealed a haemoglobin level of 11.4 g·dL−1 and a total leukocyte count of 5680 cells·mm−3, with a differential count of 62% neutrophils, 32% lymphocytes, 5% eosinophils and 1% basophils. The platelet count was 3 71 000 platelets·mm−3. Erythrocyte sedimentation rate was 75 mm in the first hour, while the C-reactive protein level was 61.2 mg·L−1. Creatinine, electrolytes and liver function tests were normal. The ECG and arterial blood gas analysis were normal. The chest radiograph (figure 1) showed a mild right-sided pleural effusion, no mediastinal shift and normal lung parenchyma. Purified protein derivative was negative. Anti-nuclear antibody and rheumatoid factor (RF) were also negative. Sputum, urine and blood cultures were sterile. Serological tests for common respiratory bacteria and viruses were negative.

Chest radiograph showing mild right-sided pleural effusion, no mediastinal shift and normal lung parenchyma.
She was subjected to a diagnostic pleurocentesis which showed a protein level of 6.3 g·dL−1 (corresponding serum proteins were 7.9 g·dL−1), lactate dehydrogenase (LDH) of 1606 U·L−1 (corresponding serum LDH was 303 U·L−1) and glucose of 1.0 mmol·L−1 (corresponding blood glucose was 4.5 mmol·L−1). The white blood cell count was 6240 cells·µL−1, with a differential count of 12% neutrophils, 78% lymphocytes, 5% eosinophils and 5% monocytes. The Gram stain and bacterial cultures were sterile. There were no acid-fast bacilli (AFB) seen in the smear, and the Mycobacterium tuberculosis reverse transcriptase-PCR was negative. The cytological examination showed no malignant cells. The adenosine deaminase (ADA) level was 107 U·L−1 (normal range: <40 U·L−1).
Task 1
What is/are the differential diagnoses of pleural effusion?
a) Tuberculosis (TB)
b) Malignancy
c) Connective tissue disease related (especially rheumatoid arthritis)
d) None of the above
Answer 1
a and b) The pleural fluid was an exudate according to Light's criteria. Pleural fluid glucose was low and this may be seen in parapneumonic effusions, where it is an indication for chest tube drainage. It is also reduced in other conditions like rheumatoid pleural effusion, TB and malignancy. Therefore, differential diagnosis for the pleural effusion included TB and malignancy (either primary or metastatic). Rheumatoid arthritis was not considered as there were no clinical features of connective tissue disease and RF was negative. Other causes like asbestosis were also not considered as there was no history suggestive of asbestos exposure and the chest radiograph did not reveal any characteristic features of asbestosis.
Task 2
What is the next appropriate step in the work-up of pleural effusion?
a) Contrast enhanced CT of the chest
b) Treatment with antibiotics
c) Pleural biopsy
Answer 2
a) Para-pneumonic effusion was unlikely as the differential count in these effusions is neutrophilic predominant. Pleural fluid and blood culture were sterile, with serological tests for infective aetiologies also being negative. In addition, there was no leukocytosis. These parameters were a sufficient reason not to initiate this patient on empirical antibiotics. As TB and malignancy were important differentials being considered, a CT of the chest would be useful as it would help in visualisation of the pleural surfaces, lung parenchyma and mediastinum. It also would be helpful in planning a pleural biopsy. Chest CT is thus the next step in the work-up of pleural effusion.
Contrast enhanced CT of the thorax (figure 2) showed a mild right-sided pleural effusion. There were no lung parenchymal opacities and significant mediastinal or hilar lymphadenopathy seen. Incidental nodules were seen in the left lobe of the thyroid, which were found to be benign on fine needle aspiration cytology. Thyroid-stimulating hormone was 1.46 mIU·L−1, which was within normal range.

a, b) Contrast enhanced CT of the thorax showing mild right-sided pleural effusion. There is no lung parenchymal opacity and significant mediastinal or hilar lymphadenopathy.
Task 3
What is the utility of ADA in areas of low TB prevalence?
Answer 3
ADA estimation in pleural fluid is helpful in differentiating tuberculous effusions from malignant ones, especially in the setting of lymphocytic predominance with malignant cytology and TB microbiological studies being inconclusive. The cut-off of 40 U·L−1 is taken as a value supportive of a diagnosis of TB pleural effusion (sensitivity: 81–100%; specificity: 83–100%). There may be false positives (empyema, rheumatoid arthritis, lung cancer, mesothelioma and haematological malignancies are associated with high ADA levels) and false negatives (early phase of disease, elderly patients and current smokers may have low ADA levels) associated with this test; therefore, its interpretation should be undertaken in light of the clinical background of the patient. In low prevalence settings, this test is more useful to exclude the possibility of TB, and in high prevalence settings it is used to rule in a diagnosis of TB [4–6].
Task 4
What is the next step in the evaluation of exudative pleural effusion?
Answer 4
In exudative pleural effusions, if the clinical features and diagnostic pleurocentesis are not helpful in arriving at a diagnosis, percutaneous pleural biopsy should be considered, especially when malignancy is considered and pleural nodules are shown on the contrast enhanced CT of the chest. In areas with a high prevalence of TB, Abrams needle biopsy is also a reasonable choice to achieve the diagnosis. In places where thoracoscopy is available, it is the investigation of choice after clinical examination and thoracentesis is inconclusive. It may either be carried out by physicians under local anaesthesia (medical thoracoscopy) or it may be carried by surgeons under general anaesthesia (video-assisted thoracoscopic surgery (VATS)). Both the procedures have similar success rates in the detection of pleural malignancies.
Thus, as the aetiological diagnosis of the pleural effusion was still elusive, the patient underwent VATS which revealed very thick erythematous fibrous parietal pleura. Lung and visceral pleura were healthy. A biopsy was taken from the parietal pleura, which showed diffuse infiltration by chronic inflammatory cells comprising of mainly lymphocytes and plasma cells. No granulomas or malignant cells were seen. Ziehl–Neelsen stain for AFB was negative. Deeper sections studied failed to show features of any specific diagnosis. The pleural biopsy was suggestive of nonspecific pleuritis (figure 3). The pleural fluid AFB culture was negative at the end of 6 weeks. Her symptoms gradually improved over a few weeks and the clinical examination was normal. The patient was reviewed at 3-monthly intervals in the outpatient department for 1 year. During this period, the patient was asymptomatic and showed no clinical or radiological evidence, i.e. on the chest radiograph (figure 4) and ultrasound of the thorax, of recurrence of pleural effusion.

a) Mesothelial lining is seen with underlying pleura showing infiltration by chronic inflammatory cells. Haemotoxylin and Eosin stain, 200× magnification. b) Pleural tissue shows infiltration by lymphocytes and plasma cells. Haemotoxylin and Eosin stain, 400× magnification.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chest radiograph showing resolution of the right-sided pleural effusion. Minimal blunting of costophrenic angles are seen on both sides. Ultrasound of the thorax showed no pleural effusion or thickening on both sides.
Discussion
Almost all pleural effusions need to be investigated with diagnostic thoracentesis to help in their diagnosis and management [7]. The classification of pleural fluid as transudate or exudate serves as a starting point in the analysis of pleural effusion. Light's criteria are widely used for this purpose. It is still useful four decades after its first publication as it is simple, easy to remember, readily measurable and accurate [8]. Cancer, pneumonia and TB are the common causes of exudates, while heart failure accounts for most of the cases of transudates [9]. Pleural fluid cytology is useful in diagnosis of malignant effusions in around two-thirds of cases [10]. Addition of the cell block technique to fluid cytological analysis augments the diagnostic yield of malignant pleural effusion [11]. The routine use of CT of the thorax in evaluation of pleural effusion is futile and only ends up in increasing the cost of managing such patients [12]. If a CT chest is required, it should be done after aspirating the pleural fluid so that the underlying lung parenchyma can be easily visualised. This is useful in moderate to large pleural effusions. Contrast infusion protocols should be modified in these patients so that the pleural surfaces are seen better [13]. A CT pulmonary angiogram should be performed in cases where pulmonary embolism is suspected as almost half of these cases are found to have pleural effusion [14]. Pleural fluid tumour markers may have a role in diagnosis of malignant pleural effusions where the cytology is negative and there is a high pretest probability of malignancy [15]. Pleural fluid ADA has a good diagnostic accuracy for tubercular pleural effusions in high prevalence areas [16]. Closed pleural biopsy is the next step in the evaluation of aetiology of pleural effusion when the clinical features and pleural fluid analysis have been inconclusive. Addition of image guidance increases the yield of the procedure. It is easy, safe and economical, and has a yield comparable to that of thoracoscopy [17]. The diagnostic yield comes down in the absence of pleural nodules or thickening <1 cm. Medical thoracoscopy is an effective and safe procedure for diagnosing exudative pleural effusion [18]. It is considered the procedure of choice for evaluating undiagnosed pleural effusion. There is no direct comparison between VATS and medical thoracoscopy in the evaluation of pleural effusion. Depending on various factors, like the appearance of the pleura on imaging, the patient's background comorbidities, availability of tests and expertise in performing procedures, a choice may be made between closed pleural biopsy and thoracoscopy to make a tissue diagnosis. As seen in our case, the patient had no clear-cut diagnosis after a detailed clinical evaluation, including the pleural fluid analysis. Therefore, the patient was subjected to thoracoscopy and pleural biopsy. A sizable number of patients with exudative pleural effusion are found to have nonspecific pleuritis on pleural biopsies [1]. It may be encountered in various conditions, including, but not limited to, exposure to asbestos, radiation or certain drugs, inflammatory conditions and idiopathic pleuritis.
Idiopathic pleuritis, also known as nonspecific pleuritis or fibrinous pleuritis accounts for ∼10% of exudative pleural effusions [19]. Studies involving thoracoscopy as a part of the diagnostic work-up are associated with fewer cases of idiopathic pleural effusion while those without it are associated with idiopathic cases accounting for almost 20% of all the causes.
This entity is a dilemma to the treating physician, as it poses as a doubt in their minds as to whether this result is indeed a benign condition or a “false negative” sampling error of malignancy. The natural evolution of nonspecific pleuritis was retrospectively studied in 75 patients. It was found that 8.3% eventually developed malignancy over the follow-up period. In 91%, the clinical evolution followed a benign course. Over a period of time, the cause of pleural effusion in these cases was found in 40 patients, while 25% were diagnosed as true idiopathic pleuritis [20]. In another study of 44 patients with nonspecific pleuritis, who were followed up until death or for a mean period of 21 months, it was found that 12% of these cases were subsequently diagnosed with malignant pleural effusion after a mean period of 9 months. All the malignancies were mesothelioma. Pleural effusion recurrence was associated with false negative pleural biopsy results [21]. These findings have been replicated in other studies where a majority of such patients have been found to follow a benign course with malignancy occurring in 8–12% of these patients, particularly mesothelioma [22]. It is challenging to diagnose mesothelioma in such situations because differentiating benign from malignant mesothelial cells is difficult. Further, in these cases, the thickened pleura is usually paucicellular. Thoracoscopic biopsies may miss these histological changes deep within the fibrotic thickened pleura. VATS or thoracotomy and pleural biopsy should be considered in patients with a high clinical suspicion of malignancy (especially in high prevalence areas for mesothelioma) and incomplete examination of the pleural surfaces by medical thoracoscopy and histological diagnosis of nonspecific pleuritis on thoracoscopic biopsies. In a prospective study of 40 cases of idiopathic pleural effusion followed for 10 years, it was found that these effusions resolved in a mean time of 5.6 months. In 12.5% of the cases there was a relapse on one or more occasions. These results justify treating the patients conservatively [23]. Most of the malignancies in nonspecific pleuritis are diagnosed within 1 year of the initial pleural biopsy. Thus, a diagnosis of nonspecific pleuritis warrants a follow-up of at least 1 year to allow for timely detection of occult pleural malignancy [24]. In our patient, follow-up was undertaken for 1 year at 3-monthly intervals and no evidence of recurrence of pleural effusion was found. The final diagnosis of pleural effusion in this patient was true idiopathic pleuritis.
Conclusion
Pleural effusion should be systematically evaluated as it has a wide range of differential diagnoses and basic fluid analysis is not specific for any particular diagnosis in many patients. After the pleural fluid analysis, if the diagnosis is elusive, thoracic CT imaging is desirable. If the imaging is inconclusive, pleural biopsy should be obtained. Where available, medical thoracoscopy is the best way to obtain the sample for analysis. Histological diagnosis of nonspecific pleuritis presents a diagnostic dilemma to the physician: whether the result presents a genuine benign pathology or is a sampling error. This would lead to consideration of either subjecting the patient to a more invasive procedure like VATS or thoracotomy, and its attendant complications, or following up the patients for a long time, which may result in significant anxiety for them. True idiopathic pleuritis occurs in less than a quarter of the patients with nonspecific pleuritis. As 12% of these cases subsequently develop malignancy and the majority of them do so within a year, these patients should be followed up for at least 1 year.
Footnotes
Conflict of interest: A. Panjwani has nothing to disclose.
Conflict of interest: M.R. Salman has nothing to disclose.
- Copyright ©ERS 2019
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










