





Abstract
Radiology plays a key role in the diagnosis of bronchiectasis, defined as permanent dilatation of the bronchial lumen. Volumetric thin-section multidetector computed tomography is an excellent noninvasive modality to evaluate bronchiectasis. Bronchiectasis is categorised by morphological appearance. Cylindrical bronchiectasis has a smooth tubular configuration and is the most common form. Varicose bronchiectasis has irregular contours with alternating dilating and contracting lumen. Cystic bronchiectasis is the most severe form and exhibits saccular dilatation of bronchi. Bronchial dilatation is the hallmark of bronchiectasis and is evaluated in relation to the accompanying pulmonary artery. A broncho–arterial ratio exceeding 1:1 should be considered abnormal. Normal bronchi are narrower in diameter the further they are from the lung hila. Lack of normal bronchial tapering over 2 cm in length, distal from an airway bifurcation, is the most sensitive sign of bronchiectasis. Findings commonly associated with bronchiectasis include bronchial wall thickening, mucus plugging and tree-in-bud opacities. Bronchiectasis results from a myriad of conditions, with post-infectious bronchiectasis being the most common. Imaging can sometimes discern the cause of bronchiectasis. However, in most cases it is nonspecific or only suggestive of aetiology. While morphological types are nonspecific, the distribution of abnormality offers clues to aetiology.
Key points
Bronchiectasis is a chronic progressive condition with significant disease burden and frequent exacerbations, for which the diagnosis relies on cross-sectional imaging.
The major imaging findings include bronchial dilatation, bronchial contour abnormalities and visualisation of the normally invisible peripheral airways.
Bronchiectasis is the end result of various conditions, including immunodeficiencies, mucociliary disorders and infections. Imaging is often nonspecific with regard to aetiology but can be suggestive.
Distribution of abnormality in the lung offers helpful clues for establishing aetiology.
Educational aims
To review the cross-sectional imaging appearance of bronchiectasis and the common associated findings.
To get a sense of how radiology can aid in establishing the aetiology of bronchiectasis.
Abstract
Bronchiectasis is a chronic progressive condition with significant disease burden and frequent exacerbations for which the diagnosis relies on cross-sectional imaging http://bit.ly/2NxOLky
Introduction
Diagnostic imaging plays a key role in the diagnosis of bronchiectasis, defined as permanent dilatation of the bronchial lumen. Bronchiectasis is increasing in incidence and frequently encountered on imaging [1]. Bronchiectasis carries significant disease burden, with reduction in health-related quality of life and frequent exacerbations often requiring inpatient management, and it is associated with increased mortality [2]. Its pathogenesis is thought to result from an initial insult to the airway followed by a vicious cycle of repeated infection and ineffective mucociliary clearance. Disruption of the peribronchial interstitial scaffolding and outward traction is thought to be its pathogenesis in relation to fibrotic lung disease. Bronchiectasis is classically categorised by morphological appearance [3]. Cylindrical bronchiectasis has a smooth tubular configuration and is the most common form. Varicose bronchiectasis is often seen with fibrosis and has irregular contours with alternating dilating and contracting lumen. Cystic bronchiectasis is the most severe form and exhibits saccular dilatation of bronchi, often with air–fluid levels. Volumetric thin-section multidetector computed tomography (CT) is an excellent noninvasive modality to evaluate bronchiectasis and allows for contiguous millimetre image reconstructions, multiplanar reformations and minimal intensity projections [4].
In this concise pictorial review, we revisit the imaging hallmarks of bronchiectasis and associated imaging findings, along with pitfalls and clues to common aetiologies for the respiratory clinician. We limit the review to non-cystic fibrosis bronchiectasis in adults, with a focus on bronchiectasis in non-fibrotic lung disease.
Imaging findings
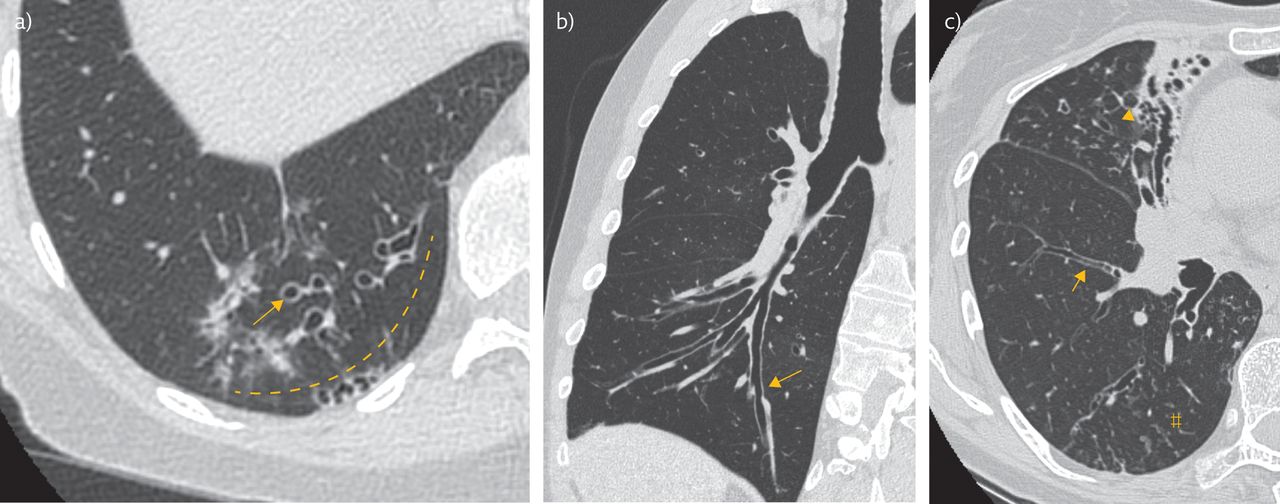
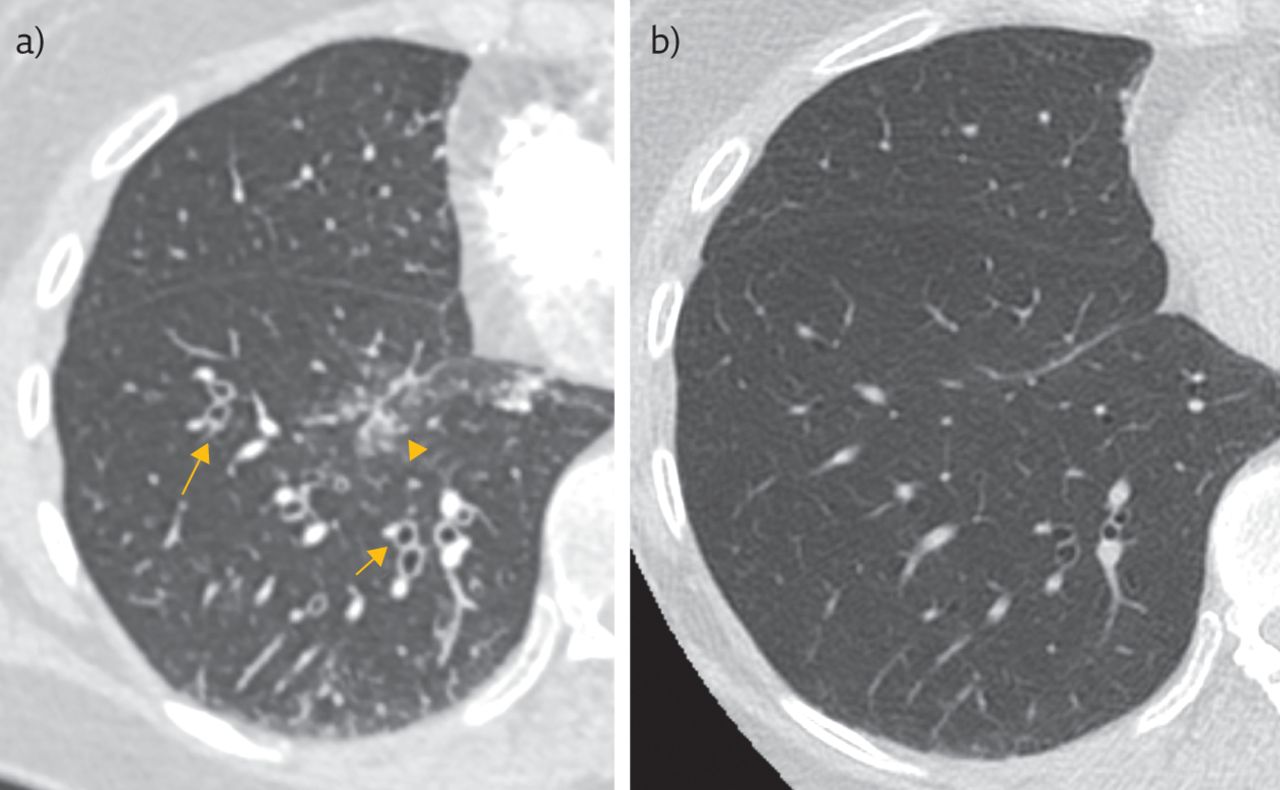
The diagnostic imaging findings in bronchiectasis are summarised in table 1. Bronchial dilatation is the hallmark of bronchiectasis and is evaluated in relation to the accompanying pulmonary artery (figure 1a). In practical terms, a broncho–arterial ratio exceeding 1:1 should be considered abnormal. Numerous physiological and disease-related conditions may affect the ratio and a cut-off of >1.3:1 or 1.5:1 results in increased specificity [5, 6]. Examples of other common causes of dilated bronchi and how to differentiate these from bronchiectasis are presented in table 2. Mild bronchial dilation can, for instance, be seen in high-altitude habitation and normal ageing. Pulmonary artery diameter can also be affected by vasoconstriction and pulmonary hypertension [6]. An important pitfall with the finding of bronchial dilatation is that mild reversible bronchial dilatation can be associated with atelectasis or inflammation, such as infectious pneumonia. This may be difficult to distinguish from true bronchiectasis, which is permanent, and precaution should be used in patients with signs of infection (figure 2).
Diagnostic imaging findings in bronchiectasis

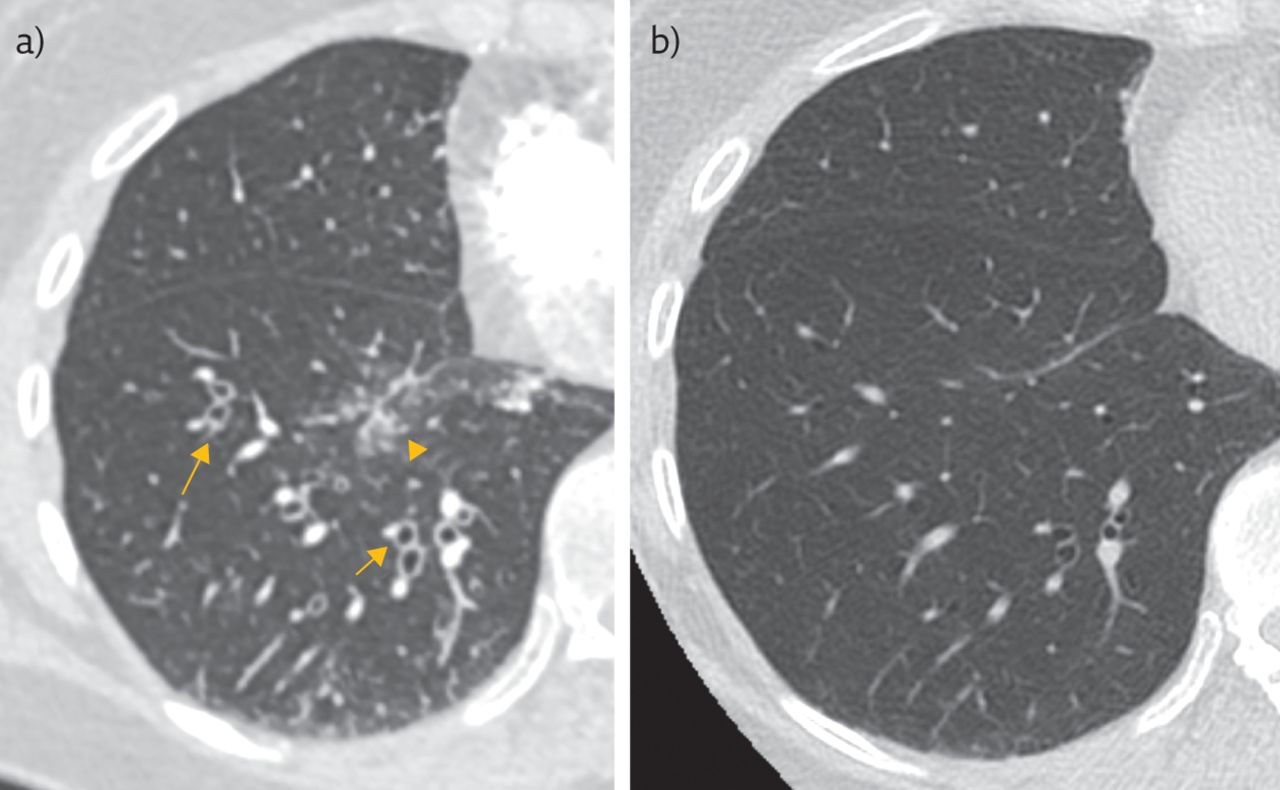
Imaging findings in bronchiectasis. a) The arrow points to cylindrical bronchiectasis in the right lower lobe. The bronchi are dilated in relation to the pulmonary artery, producing a signet ring sign. There are also visible airways in the subpleural 1 cm of lung, demarcated by the dashed line. Airways are normally not visible peripherally and when seen are indicative of bronchiolectasis. b) Curved planar reformation shows lack of bronchial tapering in the right lower lung, in keeping with cylindrical bronchiectasis (arrow). This is the earliest and most sensitive sign of bronchiectasis. The aetiology of bronchiectasis in this patient was bronchiolitis obliterans after allogeneic haematopoietic stem cell transplantation. c) Different morphological types of bronchiectasis are often seen in the same patient. This patient had cylindrical bronchiectasis (arrow) with lack of bronchial tapering in the right lower lobe and varicose bronchiectasis in the right middle lobe (arrowhead). Tree-in-bud opacities, a common associated finding, are also noted (#).
Examples of other common causes of dilated bronchi
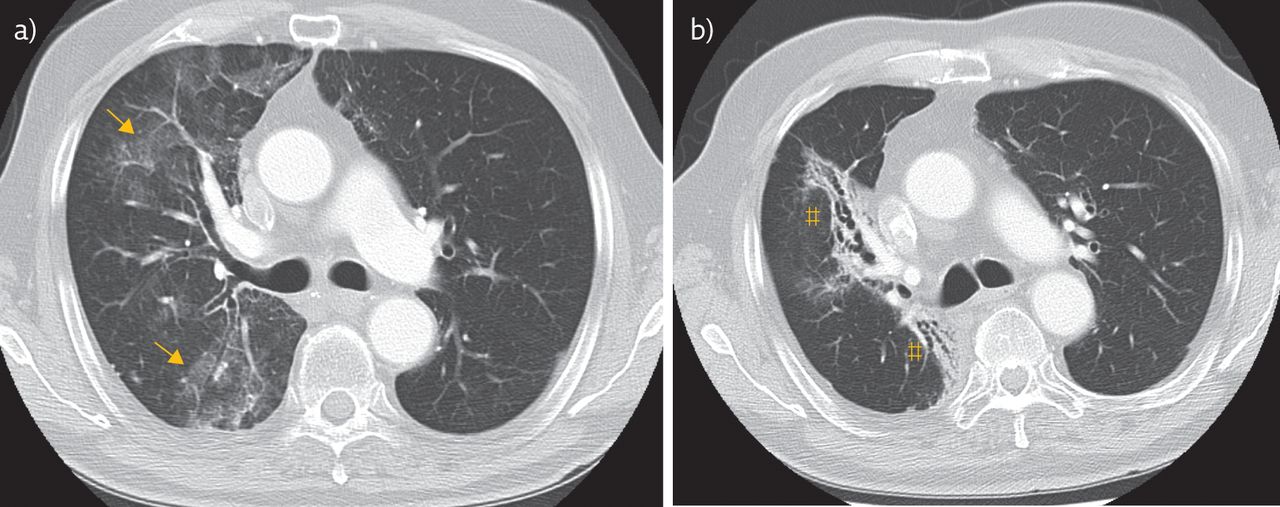
An important pitfall: mild reversible bronchial dilatation due to infection. This patient's clinical presentation gave concern for lower respiratory infection. a) Initial CT demonstrated bronchial dilatation with bronchial wall thickening (arrows) and areas of air space opacification (arrowhead), in keeping with bronchopneumonia. b) Subsequent imaging after antibiotic treatment revealed resolution of the air space opacification and a return of the bronchi to normal calibre. This does not reflect true bronchiectasis, which is irreversible.
Normal bronchi are narrower in diameter the further they are from the lung hila. Lack of normal bronchial tapering over 2 cm in length, distal from an airway bifurcation, is the most sensitive sign of bronchiectasis and is helpful in evaluating subtle cylindrical bronchiectasis (figure 1b) [7]. Visible airways in the 1-cm vicinity of costal subpleural lung are another useful sign of bronchiectasis (figure 1a). Airways are normally not visible peripherally in the lung and when visible are suggestive of dilatation of the non-cartilage-containing small airways, i.e. bronchiolectasis. Visible airways in the 1-cm vicinity of mediastinal subpleural lung are seen in many patients with bronchiectasis but also in a significant number of normal subjects and should, therefore, be considered a sign of bronchiectasis only when directly abutting the mediastinal pleural surface [8].
Findings commonly associated with bronchiectasis include bronchial wall thickening, mucus plugging and tree-in-bud opacities (figure 1c and table 1). These findings serve as indirect signs and can increase the radiologist's confidence in diagnosing mild bronchiectasis. Bronchial wall thickening is a potentially reversible finding and correlates with patient-reported symptoms, health status and frequency of exacerbation [9–11]. This finding, often subjectively evaluated, usually represents airway inflammation and can be seen in asthma and bronchitis but is also occasionally observed in normal individuals [5]. Tree-in-bud opacities represent mucus plugging or inflammatory material within the bronchioles at the level of the secondary pulmonary lobule and are usually a sign of endobronchial infection.
Common causes and imaging clues to aetiology
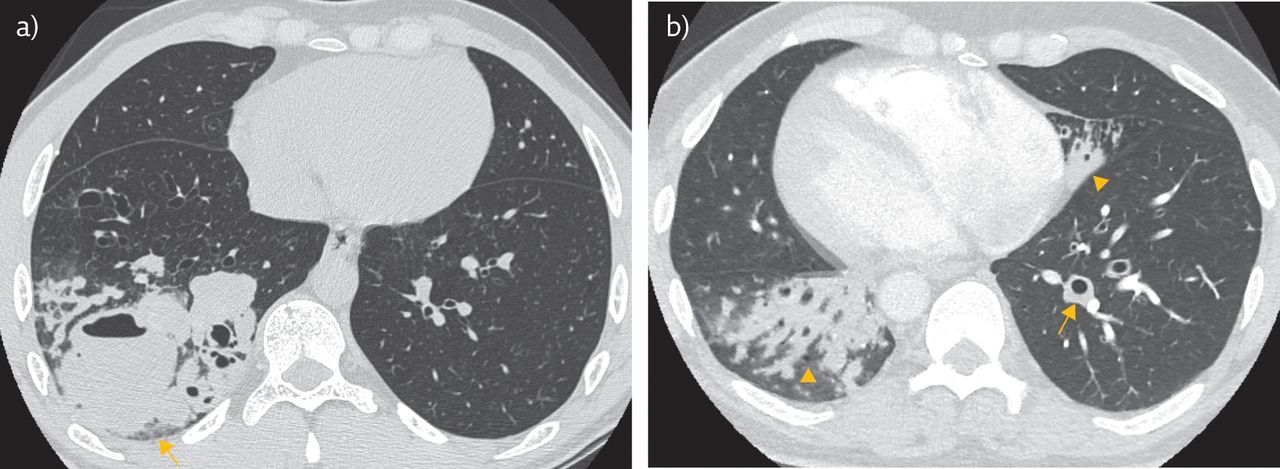
Bronchiectasis can result from a myriad of conditions, including immunodeficiencies, mucociliary disorders and infections, with post-infectious bronchiectasis being the most common [12]. Despite thorough diagnostic workup, the cause in many cases remains unknown [2]. Imaging can sometimes discern the cause of bronchiectasis, such as in the case of foreign bodies, obstructing tumours or post-radiation fibrosis (figure 3). However, in most cases it is nonspecific or only suggestive of aetiology. Morphological types are mostly nonspecific. Distribution of abnormalities, however, offers clues to aetiology. Upper lobe predominance is seen in cystic fibrosis, sarcoidosis (figure 4a), post-tuberculous scarring (figure 4b) and post-radiation fibrosis (figure 3). Calcified hilar or mediastinal lymph nodes and calcified pulmonary granulomas suggest granulomatous infection, such as tuberculosis. Anterior segment distribution (middle lobe and lingula) is typically seen in atypical mycobacterial infection, which often affects middle-aged or elderly female patients (figure 4c). Mycobacterium avium–intracellulare complex (MAC) infections usually affect two or more lobes, often with scarring and a few small nodules up to 1 cm in size. Consolidation and cavitation may also be a feature (figure 4d). Lower lobe distribution is most often seen in post-infectious bronchiectasis, chronic aspiration (figure 5), immunodeficiencies (figure 6a) and primary ciliary dyskinesia (figure 6b). Allergic bronchopulmonary aspergillosis (ABPA) bears mention due to the characteristic imaging appearance and need for specific medical management (figure 7). This condition is caused by a hypersensitivity reaction to endobronchial Aspergillus and imaging typically demonstrates central bronchiectasis with extensive mucus plugging, which in up to a fifth of cases is characteristically high attenuating (>70–100 HU) and is thought to be due to iron and manganese accumulation in the fungal debris. Location of bronchiectasis can have treatment implications in some cases, as focal bronchiectasis may be considered for lobectomy or segmentectomy, with good clinical results such as in middle lobe syndrome [13].
Post-radiation fibrosis. a) This patient had non-small cell lung cancer in the right lower lobe (not shown). The arrows show ground-glass opacities arising after radiation therapy, representing radiation pneumonitis. b) 4 months later there was interval development of post-radiation fibrosis with varicose bronchiectasis and volume loss in the treatment field (#).

a) Varicose bronchiectasis (arrow) in a patient with sarcoidosis. Note the typical upper lobe location and associated reticulation and lung architectural distortion (#), suggesting fibrosis. b) Post-tuberculous bronchiectasis in a 90-year-old patient with a previous history of tuberculosis. The apical unilateral distribution is typical. c) Bronchiectasis in the right middle lobe and lingula in a 50-year-old female patient with a MAC infection. The anterior lung segment involvement is typical. d) Bronchiectasis in a different elderly female patient with severe MAC infection. Bilateral cylindrical bronchiectasis is noted as well as nodules (arrowhead), some of which have benign pattern central calcification. Consolidation with cavitation (arrow) is seen in the left lower lobe.
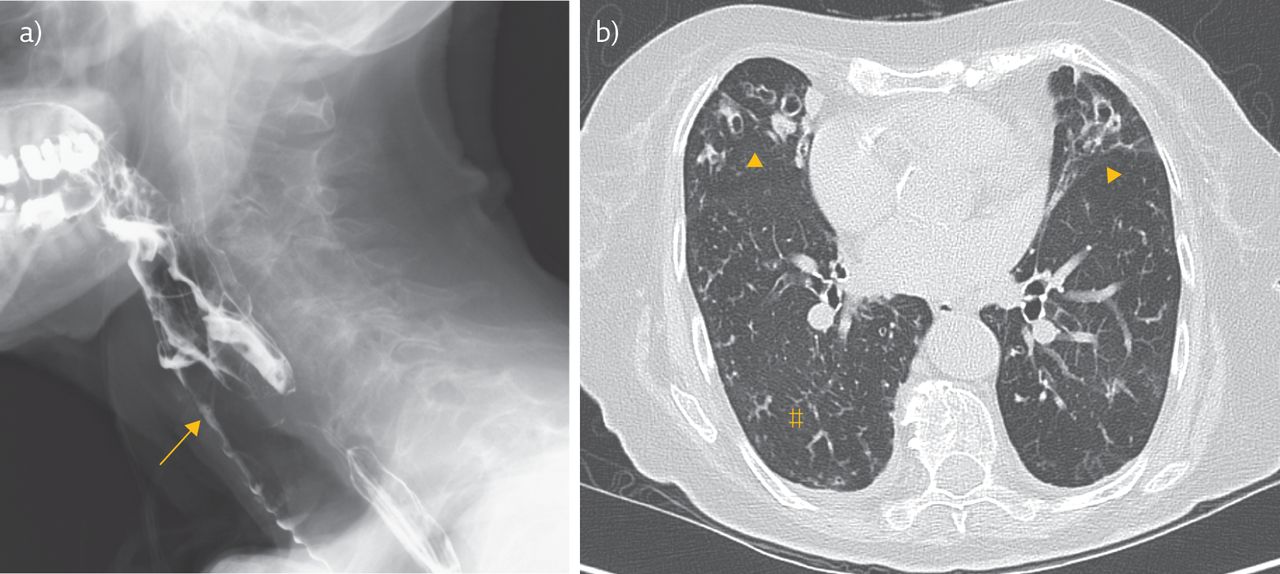
a) An 88-year-old female patient with chronic obstructive pulmonary disease (COPD), dysphagia and frequent lower respiratory infections. The arrow points to aspirated contrast material in the trachea. b) CT in the same patient shows bilateral lower zone bronchiectasis (arrowheads) and tree-in-bud opacities (#). The presumed aetiology was chronic aspiration.

a) Bronchiectasis in immunodeficiency. This patient had hyperimmunoglobulin E syndrome (Job's syndrome) and extensive bronchiectasis in the right lower lobe complicated by consolidation and an abscess formation (arrow). b) Ancillary findings with bronchiectasis. This patient had primary ciliary dyskinesia with widespread mucus plugging and adjacent consolidation, suggesting infection in the right lower lobe and middle lobe (arrowheads). The arrow points to bronchial wall thickening. Note the situs inversus.
A 71-year-old male with a history of asthma presented with a 3-month history of productive cough. This patient had a positive sputum culture for Aspergillus and peripheral blood eosinophilia. Skin-prick test was positive for Aspergillus and serum IgE levels, including Aspergillus-specific IgE levels, were markedly elevated. a) Non-contrast-enhanced CT shows high-attenuation mucus plugging (>70 HU) within dilated central airways (arrow) and atelectasis typical for ABPA. b) Follow-up imaging after antifungal and steroid treatment revealed resolution of the mucus plugging and atelectasis with residual cylindrical bronchiectasis (arrow).
Complications
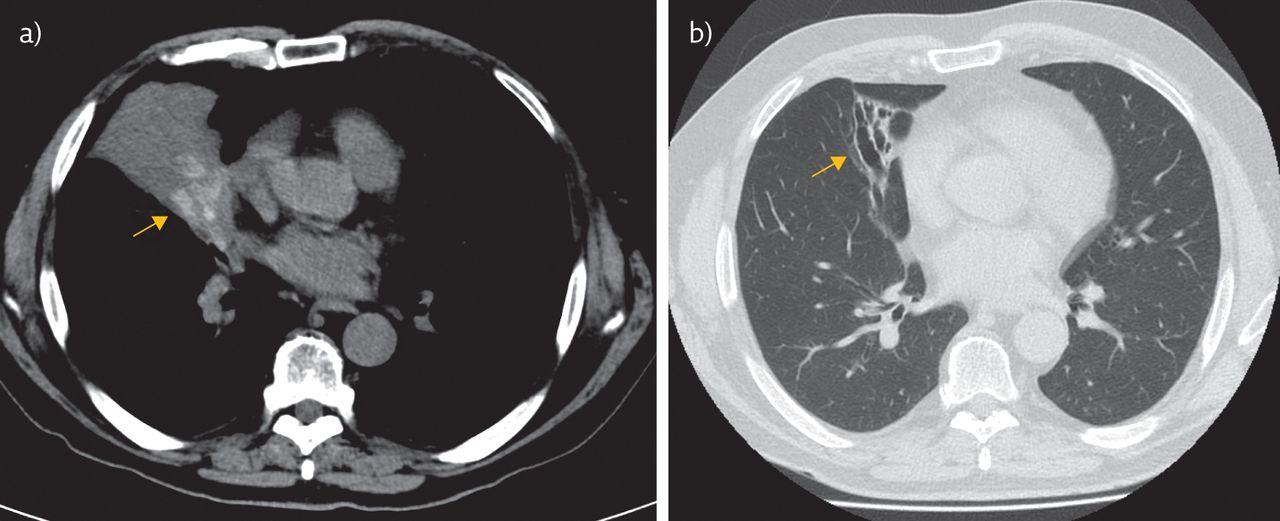
Bronchiectasis is a chronic progressive disease characterised by acute respiratory infections. Chronic airway inflammation promotes neovascularisation and arterial remodelling, resulting in fragile vessels that are prone to bleeding. This can cause haemoptysis, which is sometimes the presenting symptom in bronchiectasis and less commonly results in massive haemoptysis, requiring surgical intervention or therapeutic catheter angiography (figure 8a and b). Massive haemoptysis is due to bleeding from the bronchial arteries in the majority of cases (figure 8c) and less commonly from pulmonary arteries or non-bronchial systemic arteries [14].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
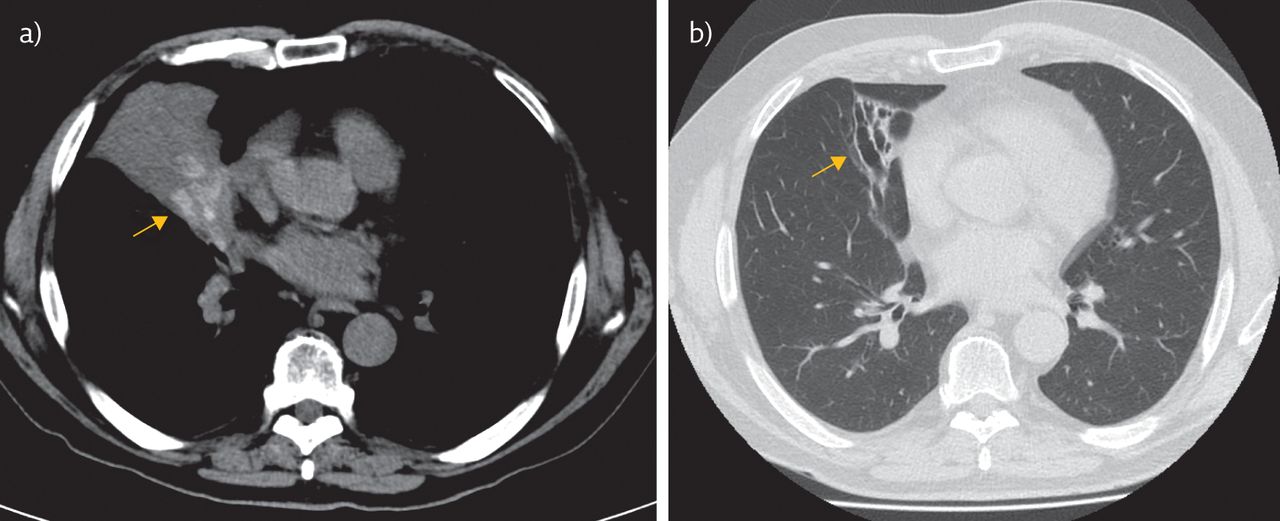
a) CT pulmonary angiogram of a 70-year-old patient with Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage four COPD on long-term oxygen therapy presenting with massive haemoptysis. Magnified sagittal reformation shows focal contour abnormality of a subsegmental pulmonary artery in keeping with a pseudoaneurysm associated with cylindrical bronchiectasis (arrowhead). The arrow points to adjacent air space opacities representing alveolar blood. b) Volume-rendered image of the pseudoaneurysm. The bleeding resolved with medical treatment and the pseudoaneurysm, bronchial wall thickening and air space opacities resolved on follow-up imaging. Case courtesy of Agusta Andresdottir (Landspitali University Hospital, Reykjavik, Iceland). c) Enlarged (>2 mm diameter) and tortuous bronchial arteries (arrow) in a different patient with severe bilateral bronchiectasis. This finding is not specific to bronchiectasis and is seen in disorders affecting the pulmonary circulation, and chronic infectious or inflammatory disease, as well as congenital conditions.
Conclusion
Bronchiectasis is a common finding on CT examinations of the chest. It is defined as permanent dilatation of the bronchial lumen, thus requiring radiological imaging for diagnosis. The condition carries significant disease burden, which makes it important for radiologists and clinicians to have detailed knowledge of its imaging appearance and associated findings, as well as findings that may aid in establishing aetiology.
Footnotes
Conflict of interest: G. Juliusson has nothing to disclose.
Conflict of interest: G. Gudmundsson has nothing to disclose.
Support statement: Funding was received from the Landspitali Research Fund (A-2018-023).
- Copyright ©ERS 2019
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










