





Abstract
Can you diagnose this young adult with post-traumatic breathlessness, unconsciousness and rash? http://bit.ly/2LlpkiV
A 23-year-old Bangladeshi male was referred to our hospital for gradual worsening of breathlessness over 3 h, developed following a road-accident about 14 h previously. He had a close fracture of mid-shaft of his right tibia, which was immobilised with back slab at the previous healthcare facility. During presentation at the emergency department, he was conscious and oriented (Glasgow coma scale 15/15), tachycardic (heart rate 132 per min), blood pressure 100/70 mmHg, tachypnoeic (respiratory rate 34 per min) with oxygen saturation 89% on room air, and afebrile. Chest examination revealed restricted chest movement, hyper-resonant percussion notes and reduced breath sound on the left, and diffuse crackles on both sides.
He was fit before the accident with no known medical illness. Oxygen supplementation (up to 8 L·min−1) and intravenous fluids were provided as required. Simultaneously, a portable anteroposterior radiograph of chest was performed (figure 1).

Chest radiography: a) anteroposterior view; b) magnified view of same image showing the clear margin of a pneumothorax on the left-hand side (dots and arrow).
Task 1
Analyse the chest radiograph.
Answer 1
The bilateral patchy opacities are likely due to pulmonary contusion or acute respiratory distress syndrome (ARDS) along with the left-sided traumatic pneumothorax.
In the meantime, as the patient's respiratory status deteriorated rapidly and he developed type 1 respiratory failure, endotracheal intubation was performed and mechanical ventilation commenced; the patient was transferred to the intensive care unit for further management. A high-resolution computed tomography (HRCT) scan of chest was performed (figure 2).
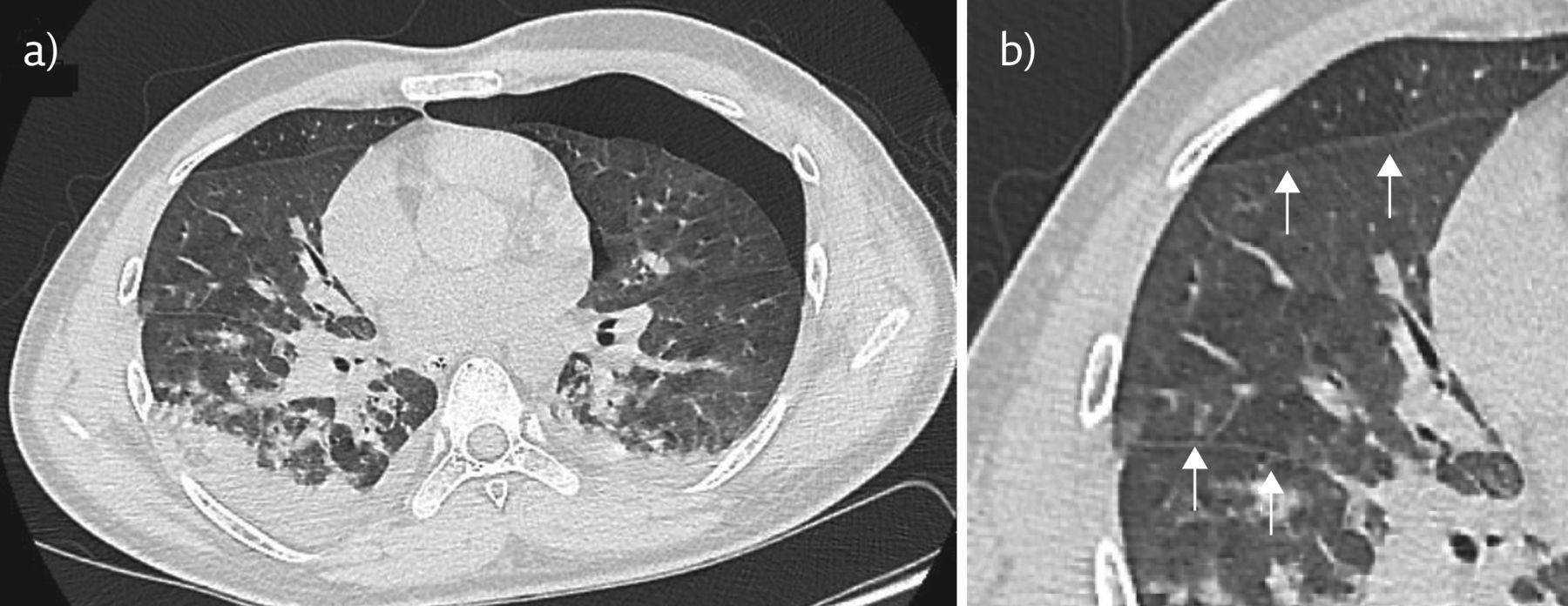
Chest HRCT: a) lung window cross section view; b) zoomed view of interlobular septal thickening (arrows).
Task 2
What is the radiological diagnosis on HRCT?
Answer 2
The HRCT shows focal areas of ground-glass opacity with interlobular septal thickening, suggesting ARDS and confirming the left-sided pneumothorax.
An intercostal chest tube (ICT) with a water seal was inserted and the patient maintained oxygen saturation of ∼91% with inspiratory oxygen fraction 0.65 on mechanical ventilation. Initial laboratory tests revealed haemoglobin 135 g·L−1, white blood cell count 10 800 per µL, platelet count 228 000 per µL and erythrocyte sedimentation rate 84 mm in the first hour.
About 21 h after the trauma, he suddenly developed one episode of generalised tonic–clonic convulsion, after which he experienced altered consciousness. The seizure activity was controlled with standard sedatives and antiepileptics. A magnetic resonance imaging (MRI) scan of the brain was performed (figure 3) as there was no head injury.

Brain MRI (DWI): hyperintense lesion in a) cortical area; and b) periventricular white matter.
Task 3
What are the radiological findings on brain MRI?
Answer 3
There is a “star field” pattern of diffuse, punctate, hyperintense lesions bilaterally in the cortical, periventricular and subcortical deep white matter in the diffusion weighted imaging (DWI) film of the brain MRI brain, which is highly suggestive of cerebral fat embolism.
On the third day of admission, a petechial rash was noticed on the anterior aspect of the chest and upper arms (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Petechial rash on left upper arm.
Task 4
What is your clinical diagnosis based on the information provided?
a) Pulmonary contusion
b) Fat embolism syndrome (FES)
c) Pulmonary embolism
d) Pneumothorax
Answer 4
b) Fat embolism syndrome (FES)
With the classic triad of respiratory, neurological and dermatological signs, and the laboratory and radiological features, the patient was diagnosed with FES, a potentially life-threatening complication of long bone fracture.
The patient was extubated 10 days after admission, and the ICT was removed 2 days later after confirmation of fully expanded chest. After 2 months of hospitalisation receiving supportive care, which included fluid resuscitation, nutrition, oxygen supplementation for correction of hypoxaemia, anticonvulsant medication, deep venous thrombosis prophylaxis, antiulcerant, etc., and specific surgical treatments of his injuries, he was discharged home and made a full recovery. On follow-up after 3 months, no complications were found.
Discussion
Fat embolism to the pulmonary circulation invariably occurs with major trauma, including elective surgical procedures such as intramedullary nailing of long bones; however, these are usually asymptomatic and resolve on their own. However, it may (0.5–11% of cases) [1, 2] progress to a systemic inflammatory cascade affecting multiple organ systems, where morbidity and mortality is high, known as FES.
Diagnosis of FES is, by and large, clinical and is characterised by the triad of hypoxaemia (95%), neurological dysfunction (60%) and petechial rash (33%) [3]. In our case, the initial presentation of post-traumatic dyspnoea and hypoxia along with imaging were indicative of pulmonary contusion with pneumothorax leading to ARDS. However, the development of altered mental status without obvious head injury and subsequent appearance of rash rightly pointed our diagnosis to FES. The classic triad is usually not present in all patient, requiring the presence of at least one major and any four of the minor criteria for diagnosis, as was proposed by Gurd (table 1) [3–6]. The presence of all the features of the classical triad makes our case an interesting one.
Gurd's criteria for diagnosis of FES
Features of FES develop in a subacute manner, usually 12 h after the initial insult, peaking at 48–72 h [7], which was observed in our case. Pulmonary manifestations are the most common initial signs, such as breathlessness, tachypnoea, hypoxaemia and respiratory failure, which were observed in our case. The radiological findings, such as the patchy ground-glass opacities associated with interlobular septal thickening on chest HRCT, were also supportive.
Neurological abnormalities vary greatly, ranging from headache, irritability, confusion to coma, and rarely include seizures and focal findings [8]. They may occur as a consequence of hypoxaemia or cerebral embolism. Generalised seizure in our case is an intriguing observation because this is very rare occurrence in FES [9]. Specific findings on neuroimaging are strongly supportive. CT scans are frequently normal in these patients. However, the characteristic MRI finding is the star field pattern, demonstrating scattered foci of high-intensity restricted diffusion on DWI [6, 8, 10] reflecting acute ischaemia and cytotoxic oedema, as in our case. This is most apparent in the acute phase, from 4 h to the first few days from the time of injury [9].
Skin changes revealed petechial rash, typically over the upper trunk, axillary regions and conjunctiva [4, 6], which was evident in our case.
Although the pathophysiology of FES remains poorly understood, two main theories were proposed. Firstly, increased intramedullary pressure after an injury causes fat droplets to be released into the venous system, which then travel through a shunt such as patent foramen ovale (PFO) or may directly filter through pulmonary capillary bed into the arterial circulation (mechanical theory). Therefore, PFO should be considered an additional risk factor for cerebral fat embolism but is not necessary for the syndrome [8]. In our case, PFO was excluded by transthoracic colour Doppler echocardiography. Another theory (biochemical) is that bone marrow fat metabolised by tissue lipase produces pro-inflammatory free fatty acids, leading to end-organ dysfunction [6]. FES may happen in nontrauma situations like acute pancreatitis, sickle cell disease and lipid infusion [6, 8].
Currently, there is no disease-specific treatment for FES; supportive intensive care is the mainstay of therapy. Heparin and corticosteroids have been proposed as treatments but have not reliably demonstrated improved morbidity or mortality. Early surgical fixation (within 24 h of trauma) carries a lower risk of FES than delayed fixation.
Conclusion
FES is an important cause of morbidity after long bone fracture. Due to its nonspecific presentation, it requires a high index of suspicion to establish diagnosis and provide prompt management to yield a better outcome.
Footnotes
Conflict of interest: S.M.R. Huq has nothing to disclose.
Conflict of interest: A.M. Anam has nothing to disclose.
Conflict of interest: N. Joarder has nothing to disclose.
Conflict of interest: M.M. Islam has nothing to disclose.
Conflict of interest: R. Rabbani has nothing to disclose.
Conflict of interest: A.K. Shaikh has nothing to disclose.
- Copyright ©ERS 2019
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










