





Abstract
An anomalous spirometric pattern can initiate a diagnostic path leading to the finding of a congenital vascular malformation. The flow–volume curve may hide a nonrespiratory pathology. Spirometry is not just asthma or COPD. http://bit.ly/30iHRCp
Case report
A 37-year-old woman, who is a mother of a 5-year-old girl, presented to our outpatient pulmonary clinic because of cough and yellowish expectorate for 20 days. She was a former smoker of 10 cigarettes a day for 20 years (10 pack-years) and worked as agricultural day labourer. Since the age of 25 years, the patient reported one or two episodes of lower respiratory tract infection (LTRI) during the winter months that resolved within a few days of antibiotic and mucolytic treatment. The persistence of cough and expectorate of the last LTRI let the general practitioner to seek a respiratory specialist respiratory consultation with spirometry.
She denied exertional dyspnoea and other symptoms. Moreover, skin prick tests for airborne allergens were moderately positive for Dermatophagoides pteronyssinus and Dermatophagoides farinae mites, but there was no history of rhinitis and of any other disease.
The physical examination of the chest was within normal limits, with no additional respiratory or cardiac sounds. Oxygen saturation by pulse oximetry was 96% on room air, blood pressure 120/80 mmHg and heart rate 65 beats per min with a regular rhythm.
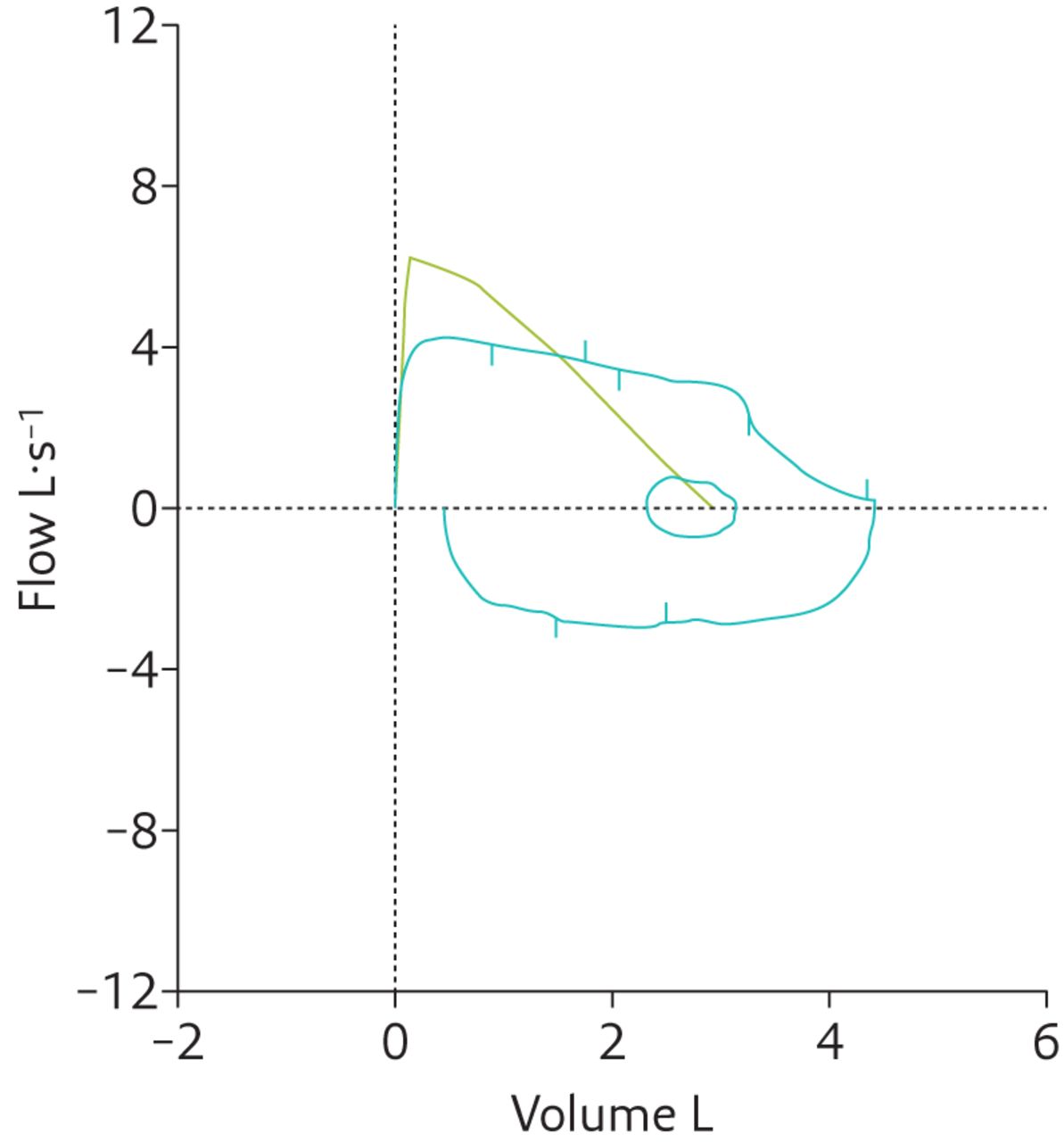
Slow and forced ventilatory manoeuvres were executed without difficulty and with the patient's full cooperation, despite her cough (figure 1).

Spirometry, flow–volume curve. Red arrow: volume–time curve; blue arrow: flow–volume loop; black circles: normal limits of the expiratory part of the flow–volume curve.
Task 1
The spirometric loop could be attributable to:
variable obstruction of extrathoracic airways
variable obstruction of intrathoracic airways
fixed airway obstruction
COPD
Answer 1
c. fixed airway obstruction. This pattern is due to some pathologies of the larynx and trachea that determine a reduction of both the expiratory and inspiratory flows. A repeatable plateau at a similar flow in both the expiratory and inspiratory sections of the flow–volume curve can be observed (figure 1). As regards quantitative evaluation, expiratory and inspiratory flow parameters (peak expiratory flow (PEF), peak inspiratory flow, forced expiratory flow at 50% of forced vital capacity (FVC) and forced inspiratory flow at 50% FVC) showed a significant and homogeneous reduction. Forced inspiratory volume in 1 s (FIV1)/forced expiratory volume in 1 s (FEV1) ratio and maximal expiratory flow at 50% FVC (MEF50%)/maximal inspiratory flow at 50% FVC (MIF50%) ratio are generally ∼1. FVC and FEV1 were in normal range (table 1).
Spirometry: best and reference values
Considering the clinical suspicion, we requested an ear, nose and throat (ENT) assessment with rhinolaryngoscopy, and a standard chest radiograph. Moreover, we asked the patient about previous chest radiography and ENT evaluations. She denied having undergone these examinations in the past. The endoscopic examination of the upper airways did not show any anatomical abnormalities. Figure 2 shows chest radiograph in posterior–anterior projection.

Chest radiograph.
Task 2
Which of the following findings can you observe on the chest radiograph?
Nothing abnormal
Stenosis of the lower third of the trachea, absence of the first left cardiac arch and right upper paratracheal abnormal mediastinal widening
Isolated tracheal stenosis
Answer 2
b. The chest radiograph evidences a stenosis of the lower third of trachea in addition to an upper right mediastinal widening and absence of the first arch of the left cardiac contour.
Task 3
What would be your further investigations for a patient with these features?
Echocardiogram
Chest computed tomography (CT) with contrast agent
Chest magnetic resonance imaging (MRI)
Fibreoptic bronchoscopy
Answer 3
b. Chest CT with a contrast agent is the investigation of choice because it allows a proper and combined assessment of trachea and mediastinal structures.

Contrast-enhanced chest CT (mediastinal window): a) axial scan; b) coronal scan. RAA: right aortic arch; LBCA: left brachiocephalic artery; Tr: trachea.
Task 4
What do you see on the chest CT images?
Right aortic arch (RAA), mirror image branching of the arch vessels
Isolated narrowing of the trachea
Kommerell's diverticulum at descendent portion of the aortic arch.
Aortic ring made of aortic arch at the front on the right, left brachiocephalic artery (LBCA) at the front on the left, Kommerell's diverticulum at the back on the left; tracheal stenosis.
Answer 4
CT scan revealed a RAA, mirror image branching of the arch vessels, Kommerell's diverticulum at the descendent portion of the aortic arch and narrowing of the trachea just 4 cm above the carina with triangular shape in the axial projection. The narrowing was due to an aortic ring made of the RAA at the front on the right, LBCA at the front on the left and Kommerell's diverticulum at the back on the left (figure 4). This finding suggested a fully closed vascular ring.

Contrast-enhanced chest CT (mediastinal window) chest: a) axial scan, diameter of diverticulum; b) coronal scan, tracheal diameter. KD: Kommerell's diverticulum.
Chest CT with contrast was performed using a Toshiba Aquilion 64-slice scanner with the following parameters: 120 kV, 300 mA and rotation time 0.5s. Figure 3 shows two mediastinal scans, an axial and a coronal one.
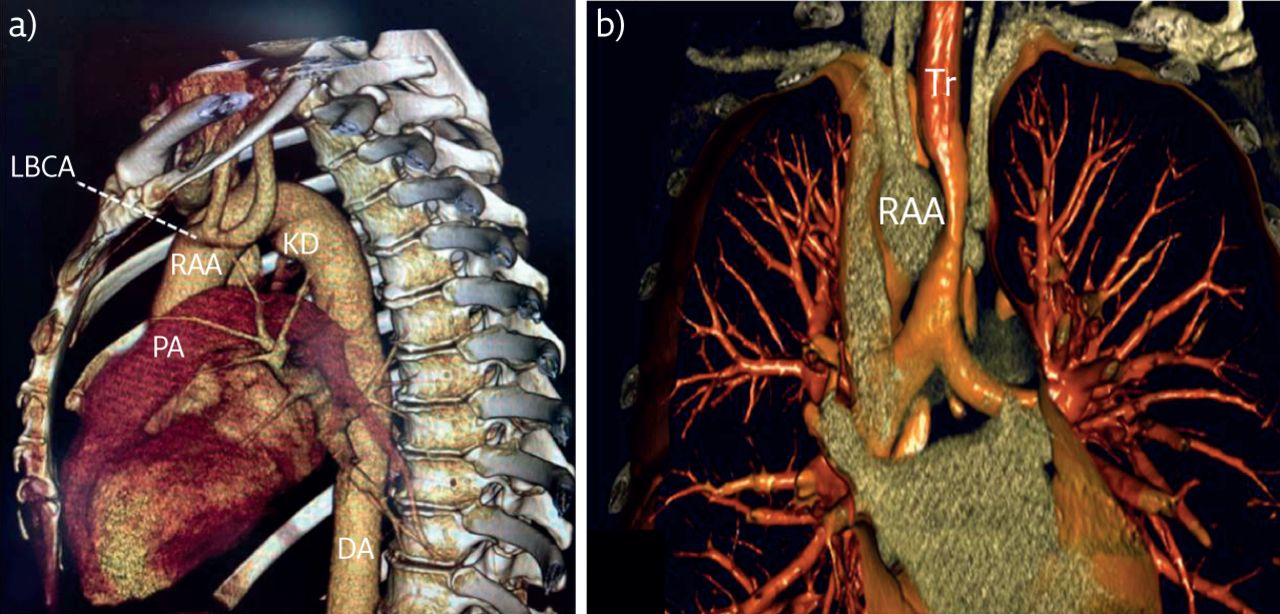
Contrast-enhanced CT was enough to make a diagnosis of fixed airway obstruction due to tracheal stenosis secondary to a fully closed vascular ring. The relationship between the vascular structures of the ring and the trachea is well visualised by the volume-rendering three-dimensional reconstruction (figure 5).

Volume-rendering three-dimensional reconstruction: a) sagittal view of aorta and Kommerel's diverticulum (KD); b) coronal view of tracheal stenosis due to vascular ring. PA: pulmonary artery; Tr: trachea.
After this finding, the patient underwent colour Doppler echocardiography, which was normal, and biochemistry examinations, which only showed increased total cholesterol (248 mg·dL−1), of low-density lipoprotein–cholesterol (163 mg·dL−1) and triglycerides (178 mg·dL−1).
The spirometric examination repeated 1 month later, when bronchitic symptoms had fully disappeared, confirmed the same pattern as the first observation (figure 6 and table 2).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Spirometry, flow-volume curve 1 month later at follow-up visit. Green: normal limits of the expiratory part of the flow–volume curve; blue: flow–volume curve of the patient.
Spirometry 1 month later at follow-up visit: best and reference values
Regarding therapeutic management, given the absence of disabling chronic symptoms due to the compression of trachea and oesophagus and, more specifically, the absence of wheezing, dyspnoea and dysphagia, we preferred a conservative approach with a multidisciplinary annual clinical–instrumental monitoring involving the pneumologist, cardiologist and radiologist.
Discussion
Spirometry is not simply an examination to measure breath; a qualitative assessment of the shape of the flow–volume curve by itself can suggest diseases involving the respiratory system but originating from other organs [1, 2]. We describe a case of central airway obstruction due to a congenital malformation of the thoracic aorta.
Upper and central airway obstruction, i.e. between pharynx and main bronchi, is an infrequent but potentially life-threatening condition. Its course may be acute, with the risk of death in a short time, or chronic, often diagnosed only after a long time when reaching a significant degree of anatomical obstruction or in cases of respiratory tract infections, as in our case [3]. The diagnosis of upper airway obstruction with a chronic course may also be delayed due to the similar clinical presentation to asthma and COPD.
The first suspicion could come from a careful assessment of the flow–volume curve. At least three maximal and repeatable forced inspiratory and forced expiratory flow–volume curves are necessary to assess the presence of central or upper airway obstruction [4].
There are three types of spirometric pattern suggesting upper and central airway obstruction: the extrathoracic variable obstruction, the intrathoracic variable obstruction and the fixed airway obstruction [4, 5]. In the first type, there is only a flattening of the inspiratory part of the curve due to a constant flow reduction; in the second, we have only a flattening of the expiratory part of the curve; in the third one, a flattening of both inspiratory and expiratory portions of the loop can be detected, as in our case. The type of curve depends on two features:
the behaviour of the lesion during inspiration and expiration, with the lumen narrowing only during one ventilatory phase (variable inspiratory or expiratory obstruction) or both (fixed obstruction).
the intra- and extra-airway pressures fluctuation during the forced manoeuvre [5].
In addition to the qualitative evaluation of the loop, the presence of upper and central airway obstruction may be detected by several quantitative methods: FIV1/FEV1 ratio; FEV1/PEF ratio; MEF50%/MIF50% ratio; MIF50% <100 L·min−1; and FEV1/forced expiratory volume in 0.5 s (FEV0.5) >1.5 [6–8].
The FIV1/FEV1 ratio is not seriously affected by a variability of effort, and is a satisfactory measurement to define upper and central airway obstruction. FIV1 and FEV1 are nearly the same in fixed airway obstruction, and therefore, the ratio is close to 1. In variable extrathoracic airway obstruction, FEV1>FIV1 and thus, the ratio is <1. Conversely, in intrathoracic variable obstruction, FEV1 is considerably lower than the FIV1 and therefore the ratio is >1. FIV1/FEV1 >1 may be also seen in patients with COPD and chronic asthma.
A FEV1/PEF ratio >10 suggests central or upper airway obstruction may be present. According to Miller and Hyatt [7], MEF50%/MIF50% is helpful in recognising fixed (MEF50%/MIF50% ∼1), variable extrathoracic (MEF50%/MIF50% >1) and variable intrathoracic (MEF50%/MIF50% <0.3) airway obstruction.
Moreover, upper and central airway obstruction may be suspected if MIF50% <100 L·min−1 and FEV1/FEV0.5 >1.5.
Regarding airway resistance, the specific airway resistance loop has an S-deformation (closed) in patients with upper airway obstruction[9]. Moreover, impairment of respiration can be assumed if, in an adult, airway resistance during spontaneous breathing is >6 cmH2O·L−1·s−1 during inspiration and/or expiration [10].
However, to date no single “gold standard” technique is currently used in routine clinical practice, and visual and quantitative diagnostic criteria have low sensitivity; therefore, clinicians should refer suspected cases for further diagnostic evaluation even in the presence of normal spirometry [11, 12].
Malformations of the aortic arch account for 1–3% of congenital cardiopathies [13]. Among the most frequent are the double aortic arch and the RAA, with multiple branching subtypes of the main vessels and the eventual association with congenital cardiopathies [14, 15]. During embryogenesis, the RAA develops from the abnormal regression of the left aortic arch. However, in the event where both left and right arches persist, one has the abnormal double aortic arch. The incidence of the RAA in radiological examinations is estimated to be 0.05–0.1% [16]. Different classifications of congenital abnormalities of aortic arches have been suggested. Edwards' classification, from 1948, distinguishes three main types: type I, with paired aortic main branches on either side; type II, with an aberrant left subclavian artery and Kommerell's diverticulum; and type III, with a single left subclavian artery arising from the pulmonary artery via a ductus arteriosus [13]. A right-sided arch is associated with various congenital cardiac anomalies, such as the tetralogy of Fallot, pulmonary stenosis, tricuspid atresia and truncus arteriosus. These are present in 5–10% of type II, and in 75–85% of type I and type III [17].
Kommerell's diverticulum is a saccular aneurysmal dilation more often associated with an aberrant left or right subclavian artery [18, 19]. From an embryological perspective, it originates from the residual distal portion of the interrupted fourth aortic arch [17]. The most important impact of the diverticulum is in terms of its encumbrance effect. Three types of diverticulum have been identified: type I, associated with left aortic arch and aberrant right subclavian artery; type II, associated with right aortic arch and aberrant left subclavian artery; and type III, located at the junction between aorta and ductus arteriosus [13, 17]. The ligamentum arteriosus (ligamentum Botalli) is a small ligament that is the remnant of the fetal ductus arteriosus. It links the descending aortic arch with the bifurcation of the pulmonary artery or the proximal tract of the left pulmonary artery. Except for rare cases of calcification, it is not usually found on CT scans of the chest but can be identified in surgical anatomy [20]. The abnormalities of aortic arch and its branches, Kommerell's diverticulum, and the ligamentum arteriosus can lead to the formation of complete or incomplete vascular rings. In incomplete rings, the nearby portion of trachea and oesophagus are displaced towards the side opposite to the arch. In contrast, complete vascular rings compress the trachea and oesophagus, thus causing a narrowing of the lumen but no dislocation. The most common types of complete vascular rings relate to congenital malformations of the double aortic arch and of the RAA with ligamentum arteriosus [21, 22]. In this second type, the left subclavian artery is typically aberrant. Instead, complete vascular rings caused by a right aortic arch with mirror image of the branching of originating arteries are very rare [23–25]. In this type of malformation, the left subclavian artery originates from a normal location, as in the clinical case reported herewith.
Aorta malformations are generally diagnosed in infants. In adults, they are typically asymptomatic, but they can show symptoms in people aged >40 years when the stiffness of the aortic arch increases because of atherosclerosis, with increased compression of the trachea and oesophagus. Possible symptoms are dysphagia, cough, heavy breathing and recurrent respiratory infections [26]. In symptomatic patients, the first examination is chest radiography. If the vascular ring is complete, the trachea does not get dislocated on the opposite side but keeps its normal site because of the presence of the ligamentum arteriosus or remnant fibrous arch. On the lateral view, one can observe an increased density behind the trachea, a focal narrowing of the trachea or an anterior curvature of the lower portion of trachea, rather than of the normal posterior curvature. The definition of the anatomy of the vascular ring and the relationship with the surrounding structures requires CT or contrast-enhanced MRI, but CT is preferable given that it allows a more accurate characterisation of the airways [15].
In the presence of respiratory symptoms, the patient should be directed to the pneumologist for spirometry. The pattern observable in the event of a complete vascular ring is that of a fixed obstruction, as shown in our case. Echocardiography could be used for the assessment of the aorta and the exclusion of simultaneous congenital cardiac malformations. Additionally, in some cases, it could be useful to perform fibreoptic bronchoscopy for a better assessment of the degree of tracheal stenosis.
Available treatment is based on surgery and it is indicated only in clinically significative cases. It consists of cutting the ligamentum arteriosus, which compresses the trachea and the oesophagus, while the Kommerell's diverticulum has to be resected at its origin [27–29].
Conclusions
Physicians involved in the management of spirometry should be aware of vascular anomalies that could cause tracheal stenosis. In our case report, we have described a tracheal stenosis with fixed airway obstruction on spirometry due to a complete vascular ring, composed of a RAA with a mirror image of the originating arterial branches (type I of Edwards' classification) on the front and concomitant type III Kommerell's diverticulum on the back. Vice versa, it is advised that the echocardiographic finding of a congenital aortic malformation by a cardiologist should be followed by spirometric evaluation.
Footnotes
Conflict of interest: G. Castellana has nothing to disclose.
Conflict of interest: R. Castellana has nothing to disclose.
Conflict of interest: R. Castellana has nothing to disclose.
Conflict of interest: C.Castellana has nothing to disclose.
Conflict of interest: P. Verde has nothing to disclose.
Conflict of interest: G. Castellana has nothing to disclose.
- Copyright ©ERS 2020
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










