





Abstract
Always consider an underlying diagnosis of Aspergillus-related disease when faced with persistent symptoms in an individual with predisposing risk factors (e.g. asthma) http://bit.ly/3aBTQip
A 66-year-old, female, lifelong nonsmoker was referred to the chest clinic on an urgent referral pathway. She presented with dry cough and breathlessness of 6 months duration on a background of intermittent cough for 5 years. She had no sputum production, haemoptysis or weight loss, and maintained a good appetite. The cough was triggered by perfumes/allergens. Her medical history was unremarkable and she denied hay fever or gastro-oesophageal reflux-like symptoms. Family history included asthma and eczema. Her father had been a heavy smoker who died of lung cancer; therefore, there had been passive exposure to smoking.
Physical examination was unremarkable. Routine laboratory tests showed a total IgE level of 240 kU·L−1 (normal range 0.0–81.0 kU·L−1), as well as elevated serum IgE and IgG antibodies to Aspergillus of 1.47 kUA·L−1 (normal range 0.00–0.35 kUA·L−1) and 192 mgA·L−1 (normal range 0.00–39.9 mgA·L−1) respectively, alongside a mild eosinophilia of 0.61×109 per L. Serum galactomannan and skin-prick tests (including Aspergillus) were negative. Spirometry testing was normal with an forced expiratory volume in 1 s (FEV1) of 2.53 L (101% predicted) and a FEV1/forced vital capacity (FVC) ratio of 0.74.
Chest radiography was unremarkable. Due to the persistent symptoms, the patient subsequently underwent computed tomography (CT) scanning of the chest (figure 1).
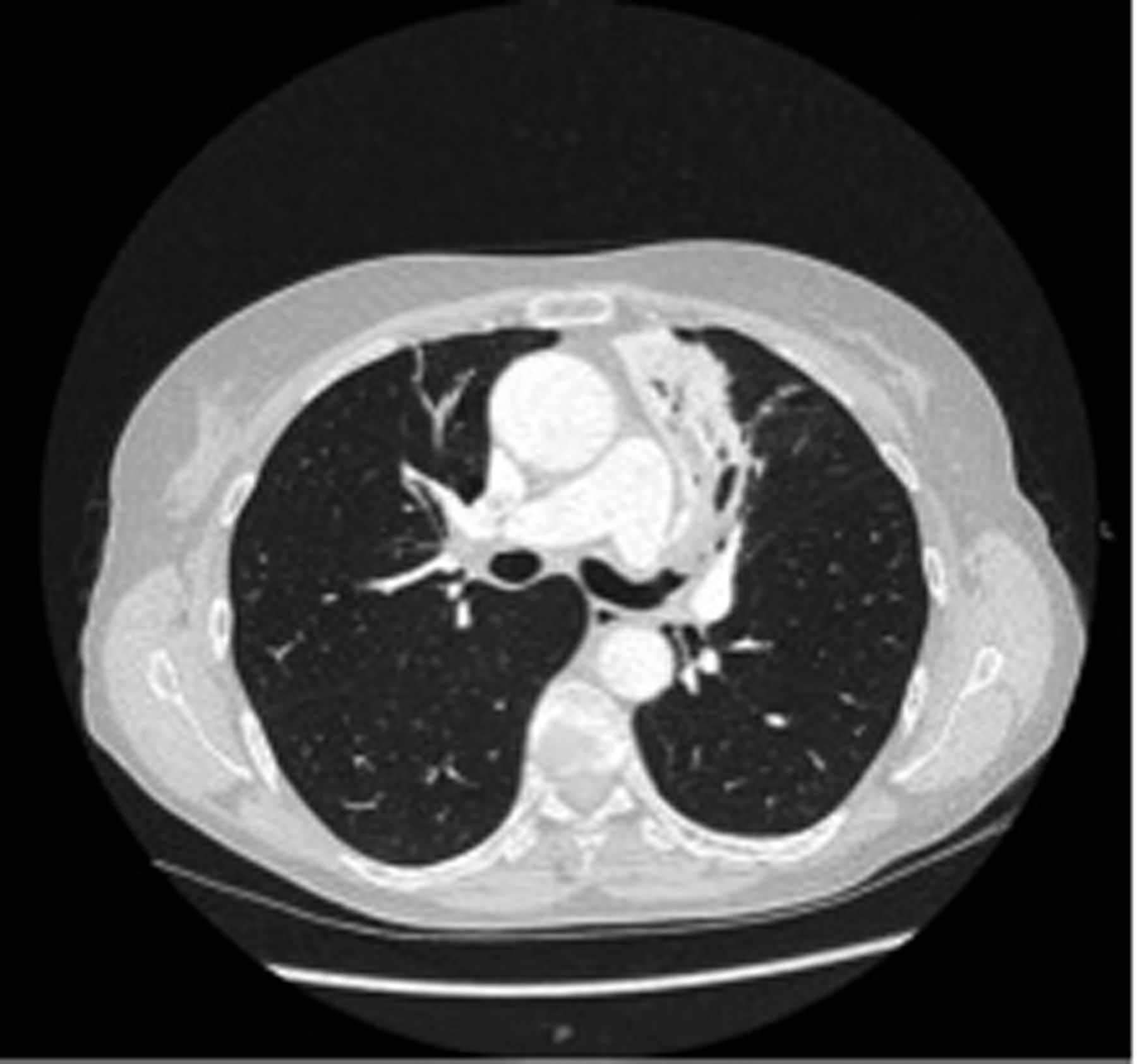
Chest CT image at initial presentation.
Task 1
Describe the CT findings seen in figure 1.
What are the differential diagnoses based on the CT scan?
What investigations would you propose next?
Answer 1
Atelectasis with consolidation and plugged airways in the left upper lobe
Inflammatory/infective consolidation, malignancy (endobronchial tumour) and mucous plugging
Sputum microbiology including acid-fast bacilli (AFB) and fungi, and bronchoscopy for brushings and/or bronchoalveolar lavage (BAL)
Sputum microbiology including AFB was negative. The patient underwent a bronchoscopy where thick secretions obscuring the lingula were identified and suctioned. BAL was performed, which showed scanty growth of Aspergillus fumigatus, and cytology confirmed Aspergillus hyphae and neutrophils with some macrophages. BAL cultures for AFB and fungi were negative.
The patient was reviewed clinically 1 month after initial review and appeared stable; the cough had improved. At this time, as there was clinical improvement and no sinister pathology at bronchoscopy, she was referred to the chest physiotherapists for sputum clearance. A repeat chest CT scan was planned in 3 months time to follow up the atelectasis and the accompanying consolidation following chest physiotherapy (therapeutic disobstruction).
3 months later, the repeat CT scan confirmed complete resolution of the previous lung abnormalities. Although repeat blood tests showed a raised Aspergillus IgE of 0.41 kUA·L−1 and Aspergillus IgG at 158 mgA·L−1, they were both lower than the initial presentation values. On clinical review, the patient was completely asymptomatic and following multidisciplinary discussions, she was subsequently discharged from routine chest clinic review.
2 months after discharge from the chest clinic, she reattended with recurrence of her respiratory symptoms, including breathlessness and a productive cough with discoloured sputum. Physical examination remained unremarkable. Lung function tests had consequently deteriorated from initial values and now showed an obstructive pattern with a reduced FEV1 of 1.60 L (65% predicted) and a reduced FEV1/FVC ratio of 0.56, without reversibility.
Chest radiography showed a recurrence of left upper lobe consolidation. Repeat CT of the chest (figure 2) and bronchoscopy (figure 3) were undertaken.
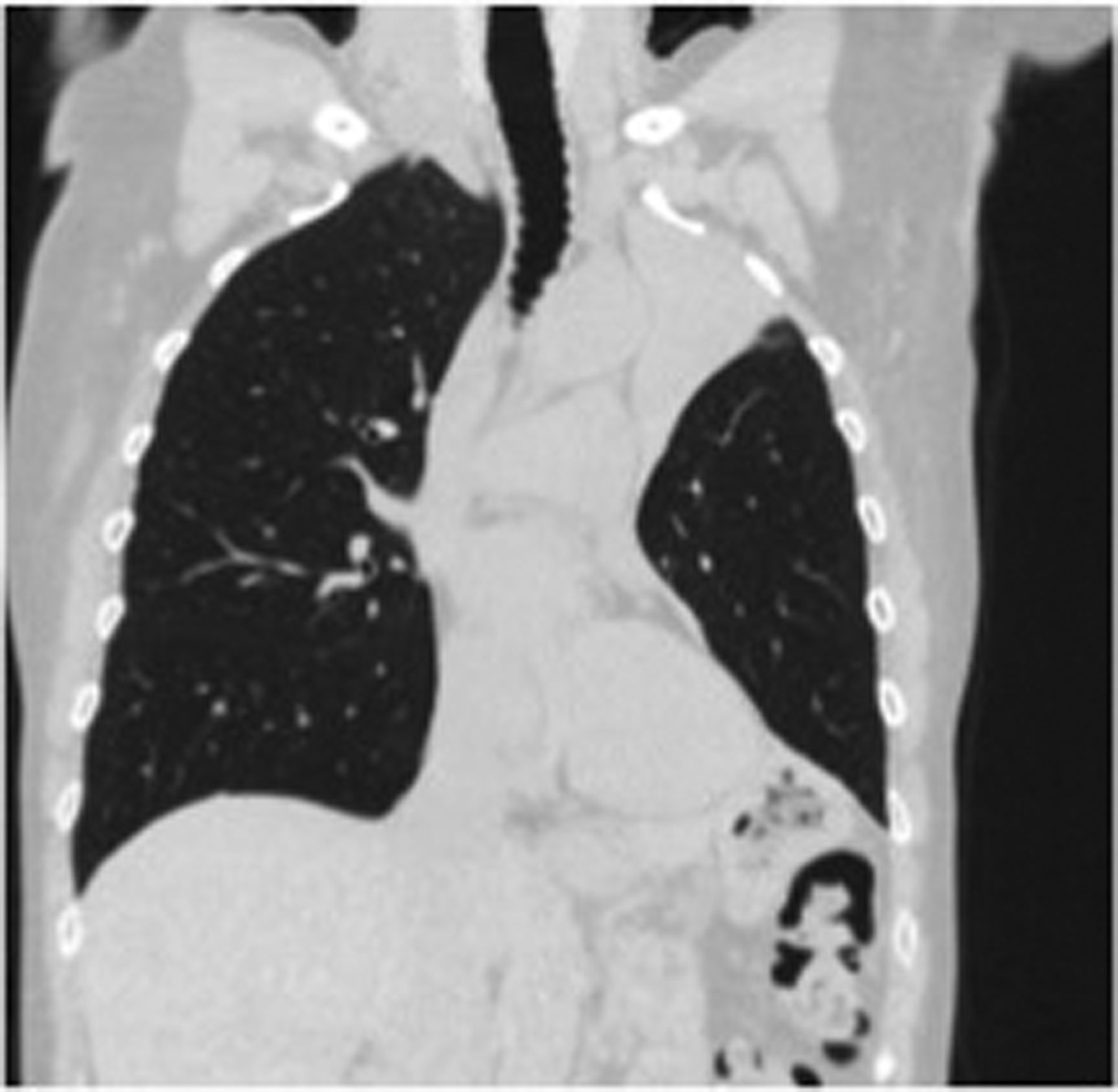
Repeat chest CT image.

Bronchoscopic image.
Answer 2
Left upper lobe collapse with raised hemidiaphragm and no obstructing lesions
Extensive mucous plugging blocking the entire left upper lobe and the lingula
Repeat BAL showed branching fungal hyphae and A. fumigatus on culture. Endobronchial tissue culture was negative. The patient was noted to have persistent mild peripheral eosinophilia (0.75×109 per L), Aspergillus IgE was 1.67 kUA·L−1, Aspergillus IgG was 202 mgA·L−1 and total IgE had risen further to 498 kU·L−1.
Task 3
What is the final diagnosis?
How would you manage this patient?
Answer 3
Allergic bronchopulmonary aspergillosis (ABPA)
Prednisolone reducing regime starting at 30 mg once a day
Our patient was started on a weaning regime of high-dose oral prednisolone and her symptoms subsequently improved. Currently, she remains asymptomatic solely with a beclometasone (steroid) inhaler and regular chest physiotherapy.
Discussion
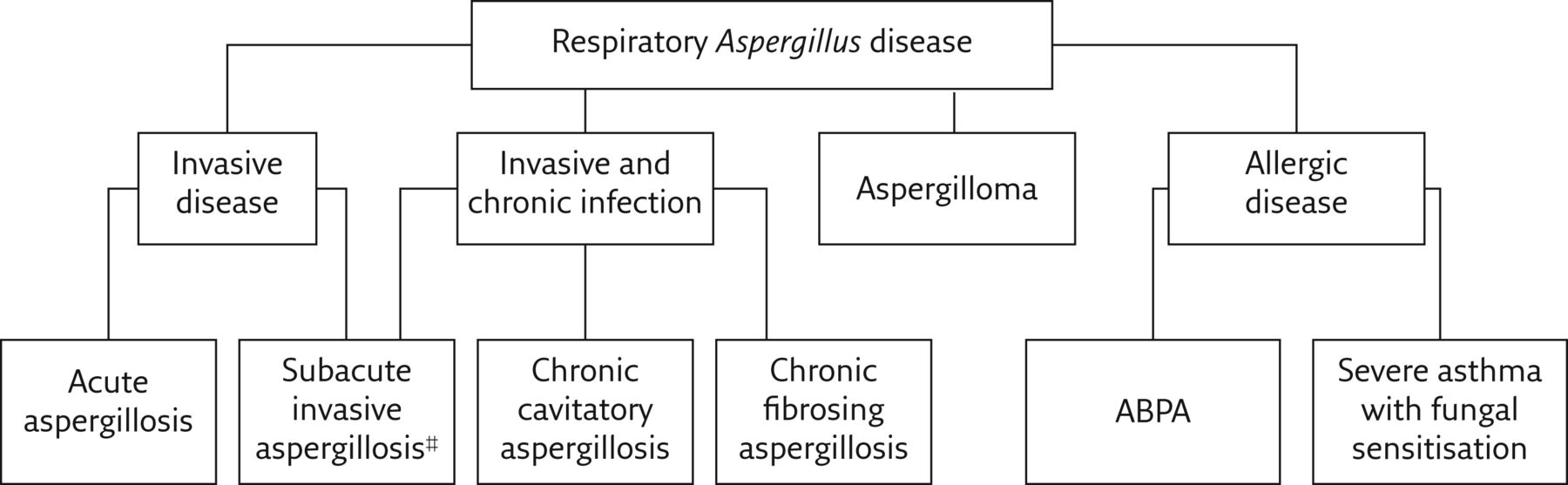
ABPA is a hypersensitivity reaction to inhaled fungi following colonisation of the bronchi. A. fumigatus is the most common fungus causing this condition (80–90% of cases) [1, 2] and is widely present in the environment. It can be encountered in everyday life including on damp surfaces and in vegetation. When an individual is exposed to the fungus, the underlying condition of the lung and the immunological state of the individual determine the outcome of disease. Thus, the development of ABPA is more common in individuals affected by asthma, cystic fibrosis and other chronic diseases of the lung where there is an aberrant immunological response [1–3]. Common symptoms experienced include those associated with bronchospasm: cough, wheeze and shortness of breath. Aspergillus can lead to a variety of clinical pathologies, which range from infections to allergic disease as outlined in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Aspergillus pathologies. #: also known as chronic necrotising aspergillosis.
Investigations for ABPA start with basic chest radiography, sputum culture and lung function tests, which may point towards a nonspecific obstructive pattern of disease. Chest radiography findings can be variable; from mild pulmonary infiltrates, to mucoid impaction, to central bronchiectasis [1, 4, 5].
If ABPA is suspected, investigations should focus on assessing for an allergic response. This is done by checking serum eosinophil levels, which are often significantly raised, as well as skin-prick testing indicating sensitisation to Aspergillus [1, 4] and serological tests. More focused serological tests include serum-specific IgE and IgG to A. fumigatus.
Comprehensive investigations, including cross-sectional imaging and bronchoscopy for BAL, can also be considered [4, 6]. This may enable culture and sensitivity testing to allow targeted antimicrobial therapy if the disease is not adequately managed with corticosteroids. CT imaging can also identify secondary complications such as bronchiectasis and chronic pulmonary aspergillosis, as well as playing a key role in monitoring the response to treatment [5].
A set of diagnostic criteria was first published in 1977 by Rosenberg, Patterson and colleagues in Chicago, which focused on a primary criterion set of seven factors [7]. More recently, in 2013, the modified International Society for Human and Animal Mycology (ISHAM) working group criteria for diagnosis of ABPA was developed as outlined in table 1 [8].
Modified ISHAM criteria for diagnosis of ABPA
Notably, our patient did not meet the ISHAM criteria for ABPA due to her total IgE count being below the 1000-IU·mL−1 threshold at 498 IU·mL−1.
In cystic fibrosis patients, the threshold for suspicion of ABPA is lower and the criteria include IgE >500 IU·mL−1 alongside clinical deterioration (e.g. increased cough, wheeze, increased sputum production and decrease in spirometric lung function) [3].
The focus of treatment is to counter the inflammatory response in the lungs and this is primarily done with systemic corticosteroids [4, 9]. Antifungal agents may be used as steroid-sparing agents and require a long course; on occasion >6 months [10–12]. Case series have shown that the use of targeted monoclonal anti-IgE therapy with omalizumab [5] and anti-interleukin 5 therapy with mepolizumab can be effective in recalcitrant cases (often cystic fibrosis patients) [13]. Further evidence on efficacy and safety in the form of randomised controlled trials is required [11].
If untreated, ABPA can lead to disabling and progressive symptoms, bronchiectasis and lobar collapse, and it has been suggested that the chronic lung damage caused may provide favourable conditions for aspergilloma formation [5].
ABPA primarily follows a relapsing–remitting course with individuals experiencing repeated flare-ups even after completing comprehensive, long treatment courses. The aim is for disease control rather than curative intent [4]. Monitoring is therefore essential and may include interval imaging and repeated lung function testing, and serum IgE levels can be indicative of allergic “activity”.
Conclusion
In this case, the diagnosis of ABPA preceded that of any known lung condition; an unusual order of events. It illustrates the need to start with baseline and basic lung function investigations, alongside comprehensive personal and family history, when dealing with any case where symptoms persist and no diagnosis has yet been made. It also highlights the importance of repeating investigations in the case of persistent symptomatology, which may have been unremarkable at the time of initial presentation. Moreover, it reinforces the need for monitoring in high-risk patients who are deemed to be stable.
ABPA should therefore be considered in all patients with underlying lung disease or a history of atopy who present with persistent symptoms, and in individuals with asthma who experience poor disease control and difficulty tapering off corticosteroids.
The relapsing–remitting course can be frustrating for both patient and physician; therefore, patient education is essential to enable them to understand and comply with lengthy treatment courses.
Footnotes
Conflict of interest: N. Fox has nothing to disclose.
Conflict of interest: S. Ranmuthu has nothing to disclose.
Conflict of interest: J. Periselneris has nothing to disclose.
Conflict of interest: G. Hardavella has nothing to disclose.
- Received August 20, 2019.
- Accepted March 2, 2020.
- Copyright ©ERS 2020
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










