





Abstract
Over the past decade there has been an increasing trend to manage many conditions traditionally treated during a hospital admission as outpatients. Evidence is increasing to support this approach in patients with pulmonary embolism (PE). In this article, we review the current status of outpatient management of confirmed PE and present a pragmatic approach for clinical healthcare settings.
Abstract
Outpatient management of pulmonary embolism should be considered in all eligible patients to prevent unnecessary hospital admissions and improve quality of care https://bit.ly/3mo5TX7
Venous thromboembolism, presenting as deep venous thrombosis (DVT) or pulmonary embolism (PE), is one of the three most frequent causes of cardiovascular mortality, including myocardial infarction and stroke [1].
From an epidemiological perspective, the incidence is eight times higher in individuals aged ≥80 years compared with patients in the fifth decade of life. Annual incidence rates for PE range from 39–115 per 100 000 population [2, 3]. Hospital-associated expenditure is rising, with an estimated total expenditure of up to EUR 8.5 billion in the European Union area. The hospital-related costs of PE, in particular, are expected to increase in the years to come, especially in ageing populations [4, 5].
The current PE guidelines suggest a stratification approach to identify patients with low, intermediate and high risk for adverse outcomes [6, 7]. Although identification of low risk patients eligible for early discharge and ambulatory/outpatient management is clinically challenging, it can potentially remove the burden from inpatient care, reduce healthcare costs, and improve patient satisfaction and quality of life [8–10]. Therefore, outpatient diagnostic and treatment pathways should be encouraged in healthcare systems.
Confirming the diagnosis: what next?
Confirmation of PE diagnosis should be followed by risk assessment to identify patients that can be considered for outpatient treatment [6, 7]. These carefully selected patients with low-risk PE are eligible for early discharge and continuation of treatment at home, provided there are proper arrangements in place for outpatient care and anticoagulation treatment [6, 7, 11, 12].
Selection criteria for outpatient management
In general, three main criteria should be fulfilled for a patient to be considered low risk and be discharged from hospital to continue anticoagulation therapy from home [6, 7]. These are:
Minimised risk of PE-related death or complications,
Absence of serious comorbidity, and
Proper care and anticoagulation therapy can be provided by the healthcare and social system on an outpatient basis.
Currently, two sets of clinical scores are recommended [6, 7, 10, 13, 14].
1) Pulmonary Embolism Severity Index (PESI) and its simplified version (sPESI), which aim to identify low-risk patients [15, 16].
2) Hestia criteria that aim to identify patients for early discharge by taking into account general medical factors as well as the patient's family/social support environment [13].
PESI and sPESI
PESI, and its simplified version sPESI, are used in the identification of patients at low risk for 30-day mortality. PESI contains a list of aggravating conditions, while sPESI excludes all patients with cancer from the low 30-day mortality risk group. Neither score requires laboratory variables. PESI criteria are divided in three main categories: demographics (age, sex), comorbidities (cancer, chronic pulmonary disease, chronic heart disease) and clinical findings (pulse rate, systolic blood pressure, respiratory rate, altered mental status, arterial oxyhaemoglobin saturation). Each criterion corresponds to a specific score and the sum adds up to the final PESI score. sPESI criteria are divided in the same three categories, but as a simplified version they only include six criteria as opposed to 11 for the PESI. The six criteria are age, history of cancer, history of chronic cardiopulmonary disease, heart rate (beats per minute), systolic blood pressure (mmHg) and oxygen saturation. Table 1 presents the PESI/sPESI risk stratification scores, associated 30-day mortality and risk of death.
PESI and sPESI scores classification, associated 30-day mortality and risk of death
PESI can help clinicians reach a decision on the management of patients who could be treated as outpatients (classes I and II), while at the same time flagging up high-risk patients that could benefit from higher levels of care. The sPESI was designed to simplify PESI and remove some of its more complicated elements; therefore, it is easier to remember. Noteworthy, it is as accurate as the original PESI [16, 17].
Both scores require an assessment of patients’ social situation before considering outpatient management including the appropriate administration of anticoagulants.
PESI has been validated in a European patient cohort (in Switzerland, France and Belgium) by Donzé et al. [18]. Diagnosis included positive computed tomography (CT), angiography, ventilation/perfusion (V′/Q′) scan or DVT with ultrasound. PESI presented a negative likelihood ratio of 0.2 for mortality and negative predictive value of 99%. It is of note that this study excluded high-risk patients (e.g. those with terminal illness or renal failure). Therefore, in a pragmatic clinical setting presented with a patient with renal failure or severe comorbidities, clinical judgement should be used over the PESI, as these patients were excluded in the validation study.
PESI has been applied in pragmatic clinical settings by Aujesky et al. [10], who conducted an open-label non-inferiority trial in Switzerland, France, Belgium and the USA where patients with PE and low PESI scores (class I/II) were randomly assigned to inpatient or outpatient groups. All patients (171 outpatients, 168 inpatients) received subcutaneous low-molecular weight heparin (LMWH) and then oral anticoagulation. This trial demonstrated non-inferiority of outpatient management for recurrent PE and death as well as for major bleeding up to 14 days.
Hestia criteria
The Hestia criteria were developed for application in haemodynamically stable patients with acute PE [13]. They contain a number of clinical parameters concerning PE severity and comorbidity (Table 2). If all parameters are absent, the Hestia result is negative and home management of PE can be considered. A negative Hestia result is associated with 0% mortality and 2% venous thromboembolism (VTE) recurrence. This tool only helps identify those who are low risk and does not necessarily predict those who are long-term high risk. On these grounds, application of the Hestia criteria can safely triage patients for outpatient management and can be easily applied at the bedside based on history taking and clinical assessment without requiring lengthy laboratory or imaging investigations. They are associated with decreased length of stay, lower healthcare costs and fewer in-hospital complications [13].
Summary of Hestia criteria
The Hestia criteria have been clinically validated in multiple additional studies and their applicability in pragmatic clinical settings has been confirmed [13, 19–21].
Nevertheless, when comparing PESI/sPESI with Hestia criteria, clinicians seem confused as to which one is the most reliable and preferable for application in daily clinical practice. For example, PESI/sPESI does not exclude pregnant women or those with medical or social reasons for hospital admission, but instead excludes the broad group of people with active cancer, which the Hestia criteria do not exclude. We have already mentioned that in the clinical validation of PESI [18], patients with renal failure and terminal illness were excluded, therefore, in a pragmatic clinical setting, clinical judgement should be used over the PESI/sPESI. Consequently, both scoring systems seem to cover different areas and therefore we feel they should both be used for selection of low-risk PE patients suitable for outpatient management. This assertion is supported by the study of Zondag et al. [21], who compared the Hestia and sPESI criteria and suggested that a proportion of patients classified as high risk by sPESI, due to underlying malignant disease, old age or cardiopulmonary comorbidities, can be safely treated as outpatients when the Hestia criteria are applied. This study showed acceptable sensitivity and negative predictive value for both the Hestia and sPESI criteria in a pragmatic clinical setting (Table 3). It also demonstrated that 25% of patients treated safely as outpatients, according to the Hestia criteria, would have been classified as high risk by the sPESI and therefore would not have been offered outpatient treatment if only sPESI was applied. Therefore, applying both prediction models can optimise the number of patients treated safely in the community. Alternatively, according to Kabrhel et al. [22], the absence of a few independent parameters, such as systolic blood pressure <90 mmHg, arterial oxygen saturation <90%, coronary artery disease, heart failure, residual DVT and active malignancy, promotes outpatient management of PE patients. Based on their study, patients lacking these features would not develop clinical decline in a time limit of 5 days after diagnosis and would not need hospital admission for special handling [22]. Therefore, in a challenging situation where PESI and Hestia contradict each other, the absence of serious comorbidities could potentially help in a more practical and pragmatic approach to the decision-making process.
Sensitivity and negative predictive value for Hestia criteria and sPESI stratification models
British Thoracic Society (BTS) guidelines provide further guidance on patients with negative Hestia criteria and right ventricular dilatation reported on echocardiography or CT pulmonary angiography. BTS guidelines recommend measuring N-terminal pro-brain natriuretic peptide and high-sensitivity troponin and should these be negative then the patient can be safely managed as outpatient following senior review [7]. Alternatively, in the case of a positive result, the patient is automatically excluded from the possibility of outpatient treatment and every possible cause of elevation should be considered simultaneously. This explains the reason why troponin, in particular, is among the primary routine examinations on hospital admission.
Outpatient anticoagulation treatment
A confirmed diagnosis of PE indicates immediate initiation of anticoagulation treatment. This could include subcutaneous LMWH, fondaparinux, intravenous unfractionated heparin (UFH) or oral anticoagulation. Fondaparinux shares the same pentasaccharide sequence as UFH and LMWH for binding to antithrombin; however, it does not have an extra chain and as such it is not considered a heparin product [23].
In the case of parenteral anticoagulation, the use of LMWH and fondaparinux is favoured due to a lower risk of bleeding, but the dosage should be adjusted to the patient's creatinine clearance [6, 7]. By contrast, UFH is the anticoagulant of choice in the case of severe renal failure (creatinine clearance <30 mL·min−1) or obesity and is modified according to the partial thromboplastin time (PTT) [23].
As far as oral anticoagulation is concerned, non-vitamin K oral anticoagulants (NOACs) are the gold standard as they cause fewer drug–drug interactions and the dosage is fixed, which minimises the amount of routine laboratory examinations necessary. Patients identified as low risk, using the Hestia criteria, can be treated with a single-drug regimen of NOACs, without prior or simultaneous use of heparin [20]. To the best of our knowledge, there is no clear evidence relating PESI or sPESI scores with specific anticoagulation therapy. Table 4 summarises all NOACs currently approved for PE treatment including their advantages and disadvantages, as well as reversing agents.
NOACs currently recommended for anticoagulation in patients with a confirmed PE diagnosis
Noteworthy, NOACs appear more beneficial in some aspects than classic heparin treatment, such as avoiding frequent injections and repeated monitoring for dose adjustments. Their application offers the possibility of a single oral drug regimen, replacing the use of parenteral treatment and warfarin [24].
Although the use of NOACs/direct oral anticoagulants is well-suited to outpatient treatment, there are some contraindicated cases such as severe renal/ hepatic impairment or antiphospholipid antibody syndrome. In addition, their use is inappropriate during pregnancy or lactation [6]. Vitamin K antagonists (VKA) appear as an alternative to NOACs, but they should be given concurrently with parenteral anticoagulation for at least 5 days and until an international normalised ratio (INR) of 2–3 is reached [11, 12].
Anticoagulant-related bleeding risk
Bleeding risk is evaluated at the beginning of the treatment and should be rechecked periodically, at least once a year in low mortality risk patients that need to receive indefinite anticoagulation treatment [6, 7]. The risk of major bleeding is higher in the first month of anticoagulant treatment and declines over time. Several bleeding risk scores exist to assess modifiable risk factors and facilitate decision making in dosage and duration of the treatment. These scores, namely OBRI (outpatient bleeding risk index), RIETE and HAS-BLED, contain several parameters that are summarised in tables 5 and 6. Among these scores, only the VTE-BLEED score could be validated in patients under anticoagulation therapy with NOACs or VKAs and it presents with a higher predictive value [25–27].
Bleeding risk scores applied prior to commencing anticoagulation treatment
Risk evaluation based on bleeding risk scores
Beam et al. [28] studied 106 patients classified as low-risk based on Hestia criteria, who were treated as outpatients for 21 days with oral rivaroxaban. During this period, no VTE recurrence or major bleeding were reported, leading to the conclusion that bleeding risk scores should not be necessarily performed on patients of low risk for PE when treated with NOACs. However, taking into account that some of these patients may have comorbidities and their disease situation can change quickly, many colleagues apply bleeding risk scoring tools as they provide them with an improved overview of the patient's disease dynamics and future treatment [28].
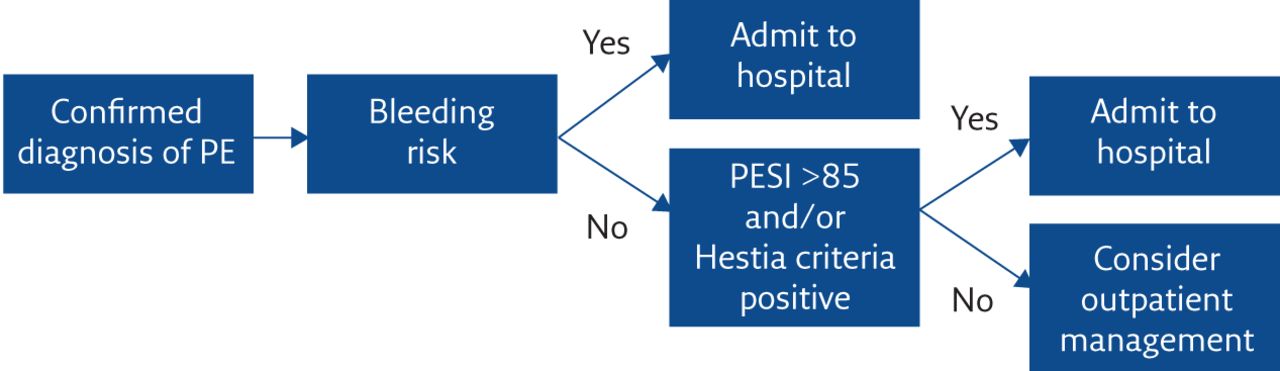
Figure 1 presents a flowchart on the selection criteria, risk assessment, etc. regarding suitability for outpatient management.
{kind=link}
A flowchart for the selection criteria, risk assessment, etc. regarding suitability for outpatient management in confirmed PE.
Treatment duration
Treatment duration has historically been a confusing issue for respiratory trainees attached to dedicated PE clinics or respiratory ambulatory care. Current guidelines avoid the use of the terms “provoked” and “unprovoked PE” that were used to determine the duration of anticoagulation treatment in the past and they recommend that all patients should receive anticoagulation treatment for a minimum of 3 months [6, 7]. The new guidelines determine the duration of anticoagulation treatment based on the presence of reversible (or not) risk factors related to the index episode of PE [6, 7].
Following this 3-month period, a balance should be maintained between the risk of anticoagulant-related bleeding and VTE recurrence risk [6, 7]. In the case of VTE recurrence, three categories can be identified if anticoagulation is discontinued in the presence of risk factors [6, 7, 29].
1) Low-risk (<3% recurrence risk per year): includes patients confined to bed inside a healthcare facility for more than 3 days or those who underwent surgery under general anaesthesia (>30 min) or patients with multiple fractures.
2) Intermediate-risk (3–8% recurrence risk per year): includes patients who underwent minor surgery with general anaesthesia (<30 min), oral contraceptives/oestrogens use, pregnancy, confined to bed out of hospital for more than 3 days with a concomitant acute illness or those having an active autoimmune disease, long haul flight.
3) High-risk (>8% recurrence risk per year): includes patients with active cancer or patients with a previous VTE episode.
Table 7 summarises the recommended duration of anticoagulation treatment tailored to different clinical scenarios.
Recommended duration of anticoagulation treatment depending on the underlying clinical scenario
NOACs are the new gold standard for anticoagulation therapy due to their lower bleeding rates compared with VKAs [6, 30, 31]. Table 8 summarises the recommended NOAC doses in the management of PE.
Recommended dosing for NOACs in the treatment of PE
Patients on extended anticoagulation treatment without underlying malignancy should be followed up in outpatients clinics where their renal, hepatic and bleeding function will be assessed regularly as well as their drug tolerance and adherence [6, 7].
Community anticoagulation services
Secondary care hosts the majority of anticoagulation service monitoring for outpatients. However, delivering these services within secondary care is accompanied by various challenges (e.g. frail patients of limited mobility, uninsured patients, wide geography). Healthcare services need to have close links with primary care and be closer to communities; thereby offering patients more control over their treatment and management plan [32].
The UK, New Zealand, Canada and the USA have successfully trialled anticoagulation monitoring through community pharmacies [32–37]. Pharmacist-led anticoagulation clinics increase patient access to professional advice and testing, and have historically led to improved INR control and self-care [38]. Patient satisfaction has been remarkable and clinical outcomes have been comparable with the ones linked with secondary care [39].
Community care pathways with strong links with secondary multidisciplinary care can be widely applied in other countries to address the challenge of wide geography, frailty and lack of insurance. This will decrease visits to emergency departments and will reduce excessive costs and health resources spent. This model could promote sufficient education, follow-up examinations and close monitoring, thus decreasing disease recurrence and hospital readmissions [40].
Summary
Outpatient anticoagulation management for appropriately selected patients diagnosed with PE constitutes the mainstay approach for low-risk patients and it continues to evolve rapidly [41]. Appropriate selection of eligible patients and assessment of haemorrhagic risk are paramount, and this should be done at the beginning of the patient's treatment, preferably right after the transportation into the accepting healthcare system centre. A systematic approach can identify patients that would benefit from outpatient management and will avoid unnecessary hospital admissions. It would be reasonable for centres to monitor their outcomes and share their experience.
Self-evaluation questions
1) What is the negative predictive value of PESI score?
a) 38%
b) 43%
c) 5%
d) 99%
2) What are the sensitivity and the negative predictive value (NPV) of the sPESI score?
a) 96% sensitivity and 99% NPV
b) 91% sensitivity and 100% NPV
c) 30% sensitivity and 10% NPV
d) 0.5% sensitivity and 20% NPV
3) Which score concerning PE morbidity contains more aggravating factors?
a) PESI
b) sPESI
c) Hestia
4) Which of followings anticoagulants is the current gold standard for outpatient management of PE?
a) NOACs
b) VKA
c) LMWH
d) UFH
5) Which of the following NOACs does not require dose adjustment for PE treatment in patients with renal failure?
a) Apixaban
b) Dabigatran
c) Edoxaban
d) Rivaroxaban
Suggested answers
d.
b.
a.
a.
a.
Footnotes
Conflict of interest: E. Bellou has nothing to disclose.
Conflict of interest: E. Keramida has nothing to disclose.
Conflict of interest: I. Karampinis has nothing to disclose.
Conflict of interest: E. Dimakakos has nothing to disclose.
Conflict of interest: P. Misthos has nothing to disclose.
Conflict of interest: P. Demertzis has nothing to disclose.
Conflict of interest: G. Hardavella has nothing to disclose.
- Received April 16, 2020.
- Accepted September 10, 2020.
- Copyright ©ERS 2020
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










