





Abstract
A systematic work-up is important in case of hypercapnia. Pay attention to the shape of the flow–volume curve and any abnormal breathing sounds. In case of stridor, vocal cord paralysis should be suspected and, if confirmed, neurological investigations are advised. https://bit.ly/34APMi8
A 55-year-old man was referred to the department of respiratory disease with a polycythaemia. Underlying haematological disease was already excluded. Blood results are shown in table 1. The patient complained of exertional dyspnoea, asthenia and intermittent daytime sleepiness. He did not experience headaches or dizziness. Heteroanamnesis revealed that that patient snored heavily without the presence of apnoeas. He had a history of nephrolithiasis, hypertension and diverticulitis, and he was a former smoker, accumulating a total of 12 pack-years. He did not use alcohol or drugs. His medication consisted of a proton pump inhibitor, an antihistaminic and aspirin.
Laboratory results for the patient
Lung auscultation revealed normal breathing sounds. In particular, no stridor was present in the upright position. There were no signs of cardiac decompensation or cardiac murmurs. The body mass index of the patient was 28 kg·m−2.
A chest radiograph was performed which did not show any significant findings (figure 1). Arterial blood gas analysis (ABG) revealed a severe hypoxaemia with combined hypercapnia (table 2). The normal pH indicates a chronic hypercapnia with metabolic compensation.

Radiograph of the thorax.
ABG analysis of the patient
Task 1
What is the most likely mechanism of hypoxaemia in this patient?
a) Diffusion limitation
b) Shunt
c) Alveolar ventilation (VʹA)/perfusion (Qʹ) mismatch
d) Hypoventilation
Answer 1
d. Hypoventilation.
Table 3 explains the five pathophysiological mechanisms causing hypoxaemia. In this case, two parameters are pivotal to determine the underlying mechanism. First, hypercapnia indicates hypoventilation (figure 2) [1]. The other causes do not explain this finding. Secondly, the alveolar–arterial gradient (A–a gradient) is often essential in the differential diagnosis of hypoxaemia (table 3) [1, 2]. The A–a gradient is the difference between the alveolar oxygen pressure and the arterial oxygen pressure (PAO2–PaO2). PAO2 is calculated using the alveolar gas equation:
(Patm−PH2O)·FIO2−PaCO2/RQ”.
Patm is the atmospheric pressure (at sea level 101.33 kPa), PH2O is the partial pressure of water (∼6 kPa), FIO2 is the fraction of inspired oxygen (0.21), PaCO2 is the arterial carbon dioxide tension and RQ is the respiratory quotient (value is around 0.82 for human diet). The A–a gradient is not a steady state. A physiological A–a gradient exists due to a physiological ventilation–perfusion mismatch and changes based on a patient's age. The expected A–a gradient can be calculated by the formula: Age+10/4 [2, 3].
This patient has a calculated A–a gradient of 1.53 kPa, which is not elevated given the age adjusted reference value of 2 kPa.
The hypercapnia and normal A–a gradient therefore indicate that the cause of his hypoxaemia is hypoventilation.

Relationship between VʹA and partial pressure of oxygen (red line) and carbon dioxide (blue line). PACO2: alveolar carbon dioxide tension. Reproduced from [1], with permission.
Pathophysiological mechanisms and related causes of hypoxaemia
Next, the patient performed lung function tests (figure 3).

Lung function tests of the patient. LLN: lower limit of normal, for spirometry values as the fifth percentile of the distribution of the standard deviation score; VC: vital capacity, FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; TLC: total lung capacity; RV: residual volume; DLCO: diffusing capacity of the lung for carbon monoxide; KCO: transfer coefficient of the lung for carbon monoxide.
Task 2
Which one of the following disorders is most likely to be the cause of hypoventilation in our patient?
a) COPD
b) Variable extrathoracic airway obstruction
c) Neuromuscular disease
d) Drug-induced hypoventilation
e) Obesity hypoventilation syndrome
Answer 2
b. Variable extrathoracic airway obstruction.
The key to this answer is the flow–volume curve of the spirometry. There is an inspiratory airflow plateau while the expiratory part is normal, suggesting a variable extrathoracic airway obstruction [4, 5]. The static and dynamic lung volumes are above the lower limit of normal, excluding COPD and neuromuscular diseases. His body mass index is compatible with overweight but not obesity and he does not use medication which suppresses respiration.
Task 3
Which examination will you request next?
a) Otorhinolaryngological (ORL) examination
b) Cardiac evaluation
c) Measurement of the fraction exhaled nitric oxide
d) Lung scintigraphy
Answer 3
a. ORL examination.
When a flow–volume curve suggests an extrathoracic airway obstruction, an ORL evaluation with endoscopy of the upper airways should be prompted. The sound in the audio fragment is suggestive for an inspiratory stridor, also indicating an obstruction in the upper airway.
A computed tomography scan excluded a mass in the neck or mediastinum as a possible cause of the extrathoracic airway obstruction. During a second visit to the clinic, the patients partner presented a recording of the sleep related sound (see supplementary material audio fragment).
The patient was referred to an ORL specialist. A video fragment of the laryngoscopy is included in the supplementary material.
Because of the daytime sleepiness, the hypercapnia and the nocturnal stridor, the respiratory physician requested a polysomnography (PSG). This revealed a complex sleep apnoea syndrome with an apnoea–hypopnoea index (AHI) of 25.7 events·h−1 sleep. Mainly obstructive hypopnoeas with also a high amount of central apnoeas were registered. Furthermore, it revealed a decreased sleep efficiency with many arousals. The arousal index was 24.1 events·h−1 sleep. His oxygen saturation was remarkably low during the whole registration, with an average saturation of 73.6% (maximum 89.9%, minimum 61.2%). No clear relationship existed between the oxygen saturation and the sleep stages or respiratory events. The oxygen desaturation index (ODI) was 64.1 (figures 4 and 5).

PSG of the patient. a) Registration of the respiratory events and AHI. b) Hypnogram with the different sleep stadia, oxygen saturation and body position. OAHI: obstructive apnoea–hypopnoea index; OAI: obstructive apnoea index; CAHI: central apnoea–hypopnoea index; HYPNO: hypnogram; A: awake; R: REM (rapid eye movement) sleep; 1–4: sleep stage 1–4; SAO2: oxygen saturation; POS: body position; BUK: abdominal position; RUG: back position; LNK: left side position; REC: right side position.
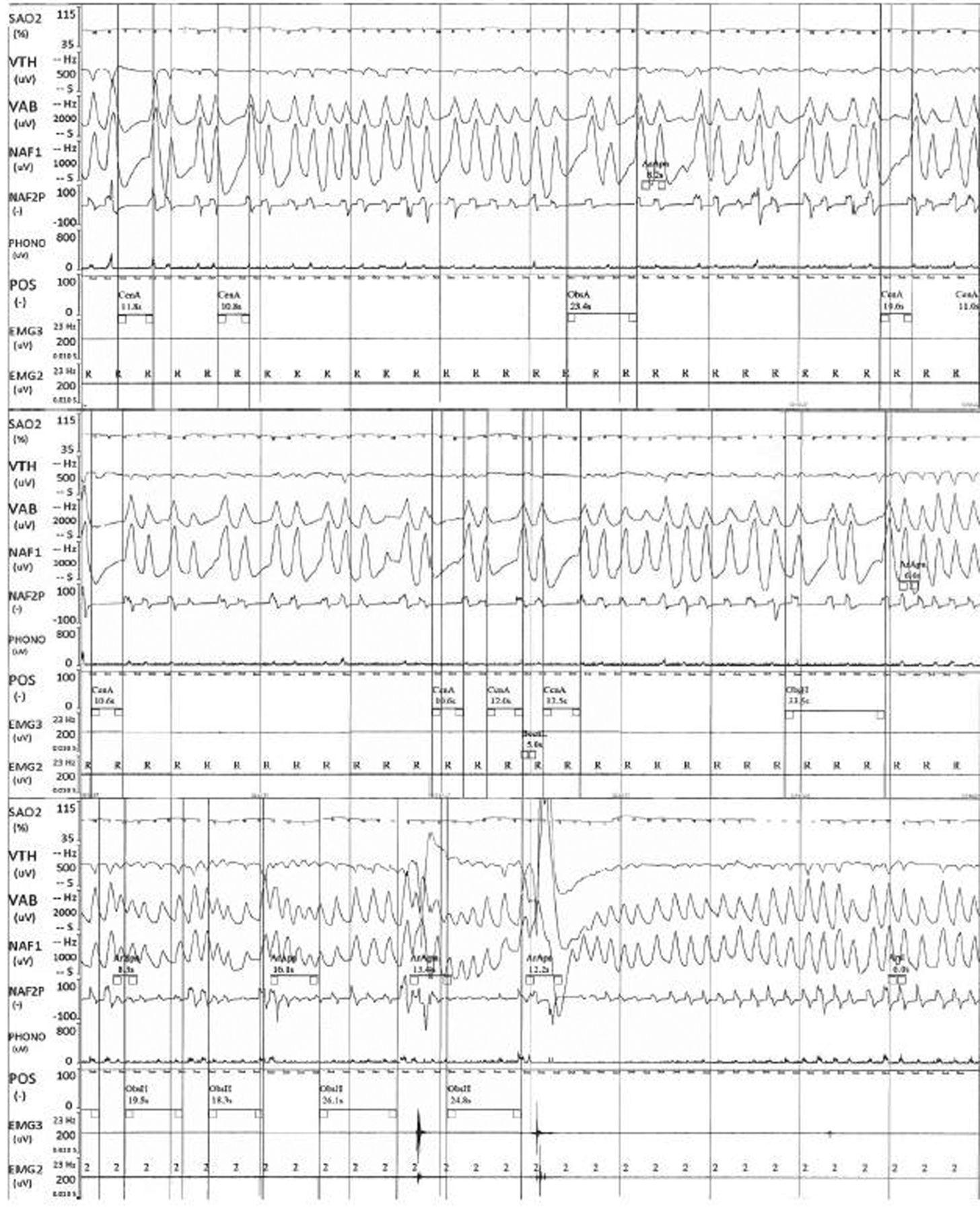
PSG of the patient. Three selected 5-min parts of the PSG record. VTH: thoracal movements; VAB: abdominal movements; NAF1: oronasal flow measured with temperature gradient; NAF2P: oronasal flow measured with pressure gradient; PHONO: sound recording (stridor in this case); EMG: electromyogram of the chin and jaw muscles; CenA: central apnoea; ObsA: obstructive apnoea; ObsH: obstructive hypopnoea; ArApn: arousal after apnoea.
Task 4
What is your next step keeping all of the above results in mind?
a) Starting positive airway pressure therapy without further investigation
b) Steroid therapy
c) Watchful waiting
d) Neurological examination with magnetic resonance imaging (MRI) of the brain and neck
Answer 4
d. Neurological examination with MRI of the brain and neck
Laryngoscopy showed bilateral vocal cord paralysis (VCP) and is probably the cause of the obstructive sleep pattern. However, it does not explain the central apnoeas that were registered. Literature suggests that 20–25% of VCP cases result from a neurological disorder [6, 7]. Thus, further neurological examination is warranted. In patients with sleep apnoea and suspicion of an underlying causative disorder, the diagnosis and treatment of this disorder has priority.
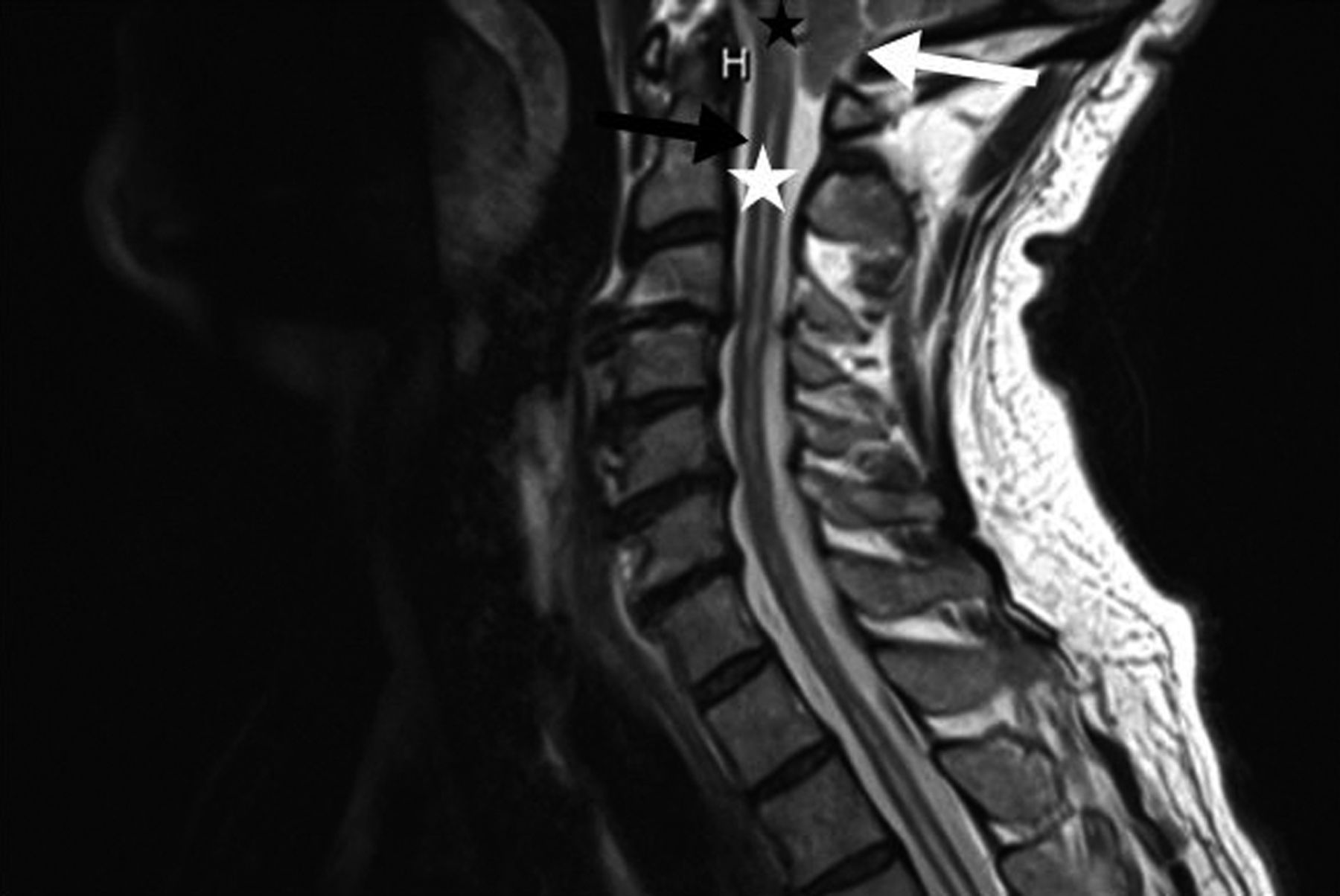
In this case, continuous positive airway pressure (CPAP) therapy was started because of the symptoms, the mixed respiratory failure and the ODI. At the same time, our patient was referred for further neurological analysis. Based on clinical neurological examination and electroneuromyography, motor neurone disease was excluded. Initial brain and cervical MRI appeared normal, but after revision by a second radiologist the sagittal plane of the cervical MRI was protocolled as abnormal with a protrusion of the cerebellar tonsils in the foramen magnum and a syringomyelic cavity involving C2. These findings are pathognomonic for a Chiari malformation type 1 (CM1) (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chiari malformation type I diagnosed by a cervical MRI (sagittal plane, T1 sequence). The white arrow indicates the protrusion of the cerebellar tonsils into the upper spinal canal (black arrow). Black asterisk: medulla oblongata; white asterisk: spinal cord.
The patient was diagnosed with CM1, with a subsequent bilateral VCP combined with a sleep-relating breathing disorder (SRBD). The therapeutic advice from a tertiary centre was to perform a posterior fossa decompression (PFD) followed by an arytenoidectomy.
Task 5
What is your preoperative advice as a pulmonologist to the neurosurgeon?
a) Preoperative therapy with steroids
b) Consult the ORL specialist about placing a tracheostomy preoperatively
c) Post-operative bronchodilatation therapy
d) Post-operative tracheostomy and invasive ventilation
Answer 5
b. Consult the ORL specialist about placing a tracheostomy preoperatively.
Securing the airway by a tracheostomy or other local techniques prior to brain surgery is recommended in patients with a VCP due to CM1. This recommendation is based on data from case series, retrospective studies and expert opinions [7, 8].
After the PFD, the degree and time of improvement of the VCP is variable and not predictable. Available literature shows that only 50% of the cases with bilateral VCP resolves completely after brain surgery. In some cases, the paralysis does even not improve after 1 year. The risk of irreversible damage is higher in adult patients than in children [7, 8]. Thus, these patients have a high risk of acute respiratory failure after extubating if the airway is not secured.
Our patient received decompressive brain surgery first. After extubating, the patient developed acute respiratory failure caused by a combination of residual vocal cord palsy and laryngeal oedema. A tracheostomy was placed immediately, after which his condition was stable. He was then transferred to a tertiary centre for laryngeal surgery.
Discussion
This case represents a rare presentation of CM1, with a chronic mixed respiratory failure, a bilateral VCP and a SRBD.
The exercise related dyspnoea and sleep-related symptoms were the sole presenting signs in our case, whereas in adults, the most common presenting symptoms are headache, vertigo and neurological deficits [9, 10]. Massimi et al. [10] reported cases with CM1 with acute onset events, including respiratory failure within 48 h. They reported seven adult cases (age ranging from 32 to 58 years with a median of 38 years). An additional literature search revealed a further 18 reported cases with acute and chronic hypercapnic respiratory failure.
The underlying pathophysiology of hypercapnic respiratory failure in CM1 is multifactorial. CM1 can cause cranial-nerve dysfunction by a stretch or compressive effect. This can lead to damage to afferent connections from the chemoreceptors in the carotid bodies to the medulla respiratory centres, with subsequent reduced response to hypercapnia [10, 11]. Furthermore, central sleep apnoea (CSA) in patients with CM can lead to hypercapnic respiratory failure. To a lesser extent, airway obstruction (e.g. due to impaired muscle function or VCP) may also contribute to the development of hypercapnia.
In this case, all of the above mechanisms are present. The hypercapnic respiratory failure is mainly caused by the CSA events and central hypoventilation. The airway obstruction and obstructive sleep apnoea (OSA) probably play a minor role considering the moderate level of the AHI.
The association between CM and SRBD has been reported in case reports, retrospective and prospective studies [9, 12–16]. They report a prevalence of SRBD in adults with CM1 ranging from 50 to 75% [9, 12–16]. Mainly OSA and mixed sleep apnoea have been described in these cases. The prevalence of CSA and hypoventilation in these cases is less frequent [9, 13–16]. One study reported a prevalence of 57.6% for OSA and 15.4% for CSA in adults. The frequency of OSA significantly increased in older age groups [13].
Given the high prevalence of SRBD in CM, experts recommend a routine screening with a PSG in these patients, regardless of the presence of symptoms [7, 9, 13]. It is questioned whether all patients with SRBD should be screened for CM with a brain MRI. No recommendations exist on this theme. There are no distinct patterns of sleep apnoea that would suggest a CM1. Possible indications for screening are treatment failure, CSA in children and CSA in adults without other risk factors [9, 13].
The exact cause of OSA and CSA in CM1 is unclear. In our case the OSA was mostly caused by the VCP. Although, hypothetically, a CM1 can directly lead to airway obstruction by compression of cranial nerves 9 and 10. These nerves innervate the pharyngeal and laryngeal muscles. An impaired function will cause an upper airway collapse, especially during sleep when the tone of the upper airway muscles is already physiologically decreased [9]. Several mechanisms are proposed for the origin of central apnoeas: compression of the medulla oblongata could cause a dysfunction of the respiratory centre, possibly through an ischaemic lesion; the afferent signal from the chemoreceptors in the carotid bodies to the medulla could be disturbed due to stretching of nerve 9 [9, 11, 12]. Obstructive sleep events may also trigger central apnoeas. One study showed a predictive value for VCP in CSA [12].
In patients with CM1 and SRBD, the treatment of choice is decompressive brain surgery to relieve the underlying cause [9]. However, in most cases, the SRBD is diagnosed prior to the CM and ventilation therapy is initiated before surgery [17–19].
In our patient CPAP therapy was also started preoperatively before the diagnosis of CM was clear. The decision to initiate ventilation was based on his symptoms and respiratory failure with a high ODI. In retrospect, preoperative ventilation was not needed in our case as his respiratory failure was compensated and the underlying cause could be managed. However, preoperative ventilation should be started in patients with severe symptoms and decompensated respiratory failure as a bridge to surgery. This recommendation is based on case reports and expert opinion [9, 11]. Two case reports demonstrate a superior effect from bilevel positive airway pressure over CPAP in patients with CM with combined CSA and OSA [17, 18].
The response of SRBD on decompressive brain surgery is variable [9]. Several studies have documented definite improvement of sleep apnoea after PFD, objectified with a PSG [12, 13, 17, 18]. However, cases with residual or recurrent sleep apnoea, especially CSA, are reported [12, 19, 20].
Importantly, post-operative awareness for respiratory failure due to residual sleep apnoea and/or residual VCP should be high in patients with CM1.
The post-operative acute respiratory failure in our patient was explained by laryngeal oedema post-intubation in combination with residual VCP. This was documented by an upper airway endoscopy at the intensive care unit. This event illustrates the importance of securing the airway prior to decompressive brain surgery. After a temporal tracheostomy followed by an arytenoidectomy, his symptoms improved. Not only the nocturnal stridor resolved, but also the daytime sleepiness and dyspnoea. A post-operative ABG (table 4) did not show any residual respiratory insufficiency.
A post-operative ABG analysis with tracheostomy
Further research is warranted to determine the optimal timing of surgery and post-operative followup with PSG in patients with CM and SRBD.
Conclusion
This case illustrates a stepwise approach towards patients with chronic hypercapnic respiratory failure. Asking the patient about sleep-related symptoms, breathing sounds and medication use is essential. Evaluation of the flow–volume curve shape is key as it can reveal important information about the airways. VCP is a possible cause of an extrathoracic obstruction and obstructive sleep apnoea. In case of a documented VCP, a neurological cause should be excluded.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary audio EDU-0217-2020.SUPPLEMENT1
Supplementary video EDU-0217-2020.SUPPLEMENT2
Acknowledgments
We thank K. Strobbe, respiratory physician at AZ Nikolaas hospital, Sint Niklaas, Belgium, for providing the polysomnography and helping with its interpretation; A. Otte, respiratory physician at Zuyderland medical center, Heerlen, The Netherlands, for a second revision of the polysomnography; and M. van der Steege, English teacher, for revising the English writing style.
Footnotes
This article has supplementary material available from breathe.ersjournals.com
Conflict of interest: J. Van Woensel has nothing to disclose.
Conflict of interest: P. Goeminne has nothing to disclose.
Conflict of interest: Y. Valcke has nothing to disclose.
- Received August 19, 2020.
- Accepted October 26, 2020.
- Copyright ©ERS 2021
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










