





Abstract
Inflammatory myofibroblastic tumour (IMT) is a rare neoplasm, most commonly described in children and young adults. We present a case of IMT in an elderly man. https://bit.ly/355wf8X
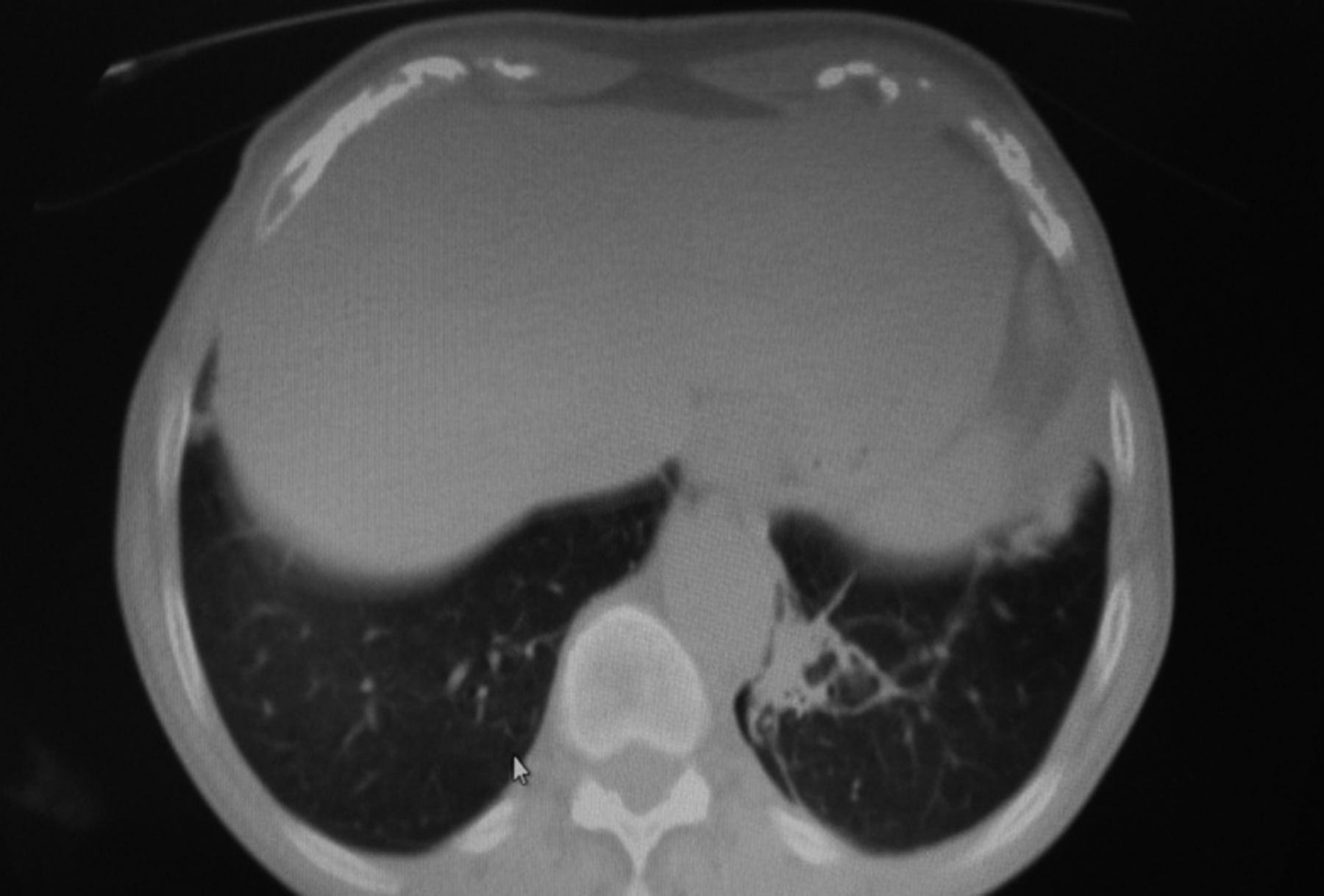
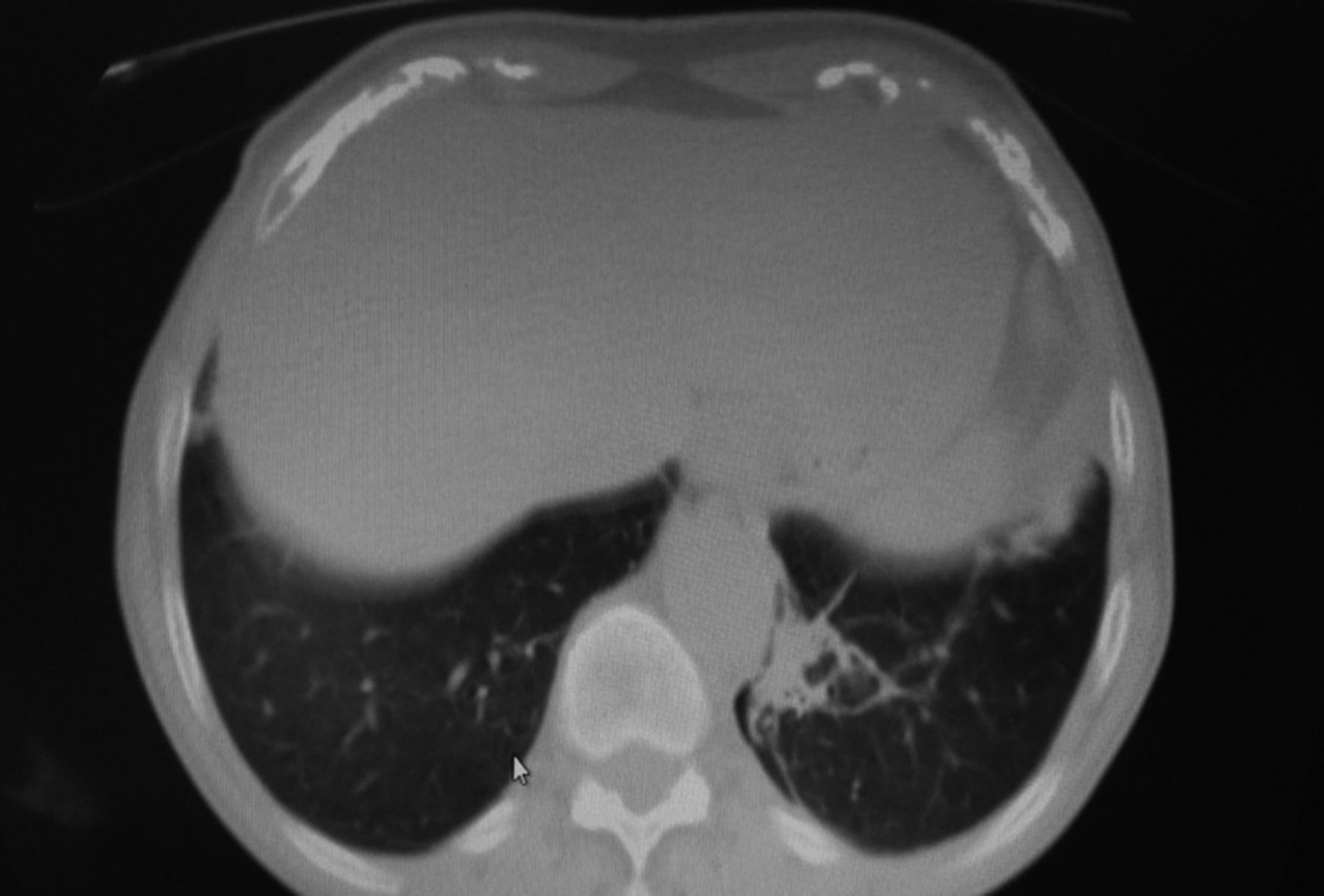
An 81-year-old former smoker, with a history of asthma and surgical treatment of abdominal aortic aneurysm, was admitted to hospital with a 1-month history of fever up to 38.6°C, purulent sputum and left-sided pleuritic chest pain. Chest computed tomography (CT) showed consolidation type infiltrates peripherally in both lungs. Flexible bronchoscopy revealed no endobronchial lesion and cytological and microbiological examination, as well as qualitative analysis of bronchoalveolar lavage (BAL) were non-diagnostic. The cytological examination of BAL revealed: macrophages 85%; lymphocytes 12%; eosinophils 2%; and other neutrophils 1%. Investigations for IgG4-related disease or any other autoimmune disorder were negative. The patient was treated with amoxicillin–clavulanic acid for 10 days before admission. He was treated with ciprofloxacin–clindamycin on admission, but due to clinical and radiological deterioration on chest CT, we administered wide-spectrum antibiotics (meropenem plus vancomycin) without clinically significant response (figure 1).

Chest CT: a) middle lobe, b) lower lobe.
Task 1
Describe radiographical findings on the chest CT (figure 1).
Answer 1
Bilateral lung infiltrates with consolidation appearance.
Task 2
What is your differential diagnosis?
Answer 2
The differential diagnosis includes cryptogenic pneumonia, lymphoma, nonspecific lung infection, IgG4-related disease [1].
Task 3
Which is the final diagnosis?
Answer 3
A transbronchial biopsy of the left lower lobe that was taken through bronchoscopy was not diagnostic, due to the small size of the tissue specimens. Therefore, we performed CT-guided fine needle biopsy (FNB) in segment 10 of basal group of left lower lobe and the histological examination revealed an inflammatory myofibroblastic tumour (IMT), smooth muscle actin (SMA)+, activin receptor-like kinase 1 (ALK-1)+/− (weakly positive in rare cells), Desmin−, CD34−, AE1/AE3−, Ki67+ in rare cells. The histological picture consists of fibrosis, myxomatous degeneration of substrate and a mixture of plasma cells, lymphocytes (small B-cells, CD20+), T-cells and histiocytes (CD68+).
Task 4
What are the available therapeutic options for IMT? What is the duration of disease remission?
Answer 4
Surgical resection is the procedure of choice for both diagnostic and therapeutic reasons and achieves low recurrence rates. However, other treatment options, such as corticosteroids, nonsteroidal anti-inflammatory drugs, chemotherapy or radiotherapy, are alternative strategies in case of nonsurgical procedure. Treatment with nonsteroidal drugs in ALK− tumours seems to be a safe and effective alternative option with promising clinical outcomes that persist even after ceasing therapy. In our case, as soon as we received the histological examination and due to the lack of response to wide-spectrum antibiotics, we switched up to nonsteroidal anti-inflammatory drugs, without an interval period, after antibiotic cessation. Taking into account the patient's advanced age, comorbidities including asthma and recent surgical excision of an aneurysm of abdominal aorta, as well as bilateral lung findings, the patient was considered not eligible to undergo surgical excision or chemotherapy. Due to the multifocal and bilateral localisation of the lesions radiation therapy was excluded. The patient was treated with naproxen 250 mg p.o. twice daily, for 1 month and subsequently with a dose of 250 mg p.o. once daily. Duration of treatment was approximately 2 months, with fever regression and clinical improvement. Follow-up after 2 and 6 months showed definite radiological remission of CT findings, despite cessation of therapy (figures 2 and 3), [2, 3].

Resolution of infiltrates in the right lung.
{kind=link}
{kind=link}
{kind=link}
Radiological improvement in the left lower lobe.
Discussion
IMT is a mesenchymal neoplasm, first described by Bahadori and Liebow [4] in 1973, that accounts for 0.04–1% of all lung neoplasms [5]. The tumour presents with intermediate biological potential, occurring at any anatomic site, with a predilection for the lung, soft tissue and viscera of children and young adults below 40 years old, in both genders [3, 6]. IMT represents the neoplastic subset of the family of inflammatory pseudotumours [2]. It probably occurs as an inflammatory response against infectious factors, trauma or immunological reactions [2, 7]. There is a relationship with respiratory infections including Mycoplasma pneumoniae, Klebsiella, Pseudomonas, Mycobacterium avium complex (MAC), actinomycetes, Epstein–Barr virus (EBV) and human herpesvirus 8 (HHV8) [2]. IMT can behave as a malignant tumour both clinically and radiologically. However, there is no TNM (tumour, node, metastasis) classification available, based on the Classification of Tumors of the Lung, Pleura, Thymus and Heart (2015) [8].
IMT is a distinctive lesion composed of myofibroblastic spindle cells accompanied by an inflammatory infiltrate, usually composed mainly of plasma cells and lymphocytes [8]. Macroscopically, the tumour appears as a well-circumscribed white-yellow nodular mass of firm consistency. Microscopically, it is characterised by polyclonal plasma-cell infiltration, with inflammatory cells presentation, such as leukocytes, histiocytic cells, neutrophils and myofibroblasts, with the latter considered to be the predominant cell type [2].
Symptoms are nonspecific and include fever, cough, shortness of breath, pleuritic chest pain, haemoptysis and weight loss [2, 7]. The treatment of choice remains surgical resection, with rare recurrence after complete excision of the tumour [2, 3, 6, 7, 9]. A collection of case studies showed that survival rates at 5 and 10 years have been reported to be 91% and 77%, respectively [7]. Corticosteroids and nonsteroidal anti-inflammatory drugs have been used with good clinical response, as well tyrosine kinase inhibitors in cases of ALK+ neoplasm and finally, chemotherapy or radiotherapy in selected patients [2, 3, 9].
Imaging findings reflect pathological features and vary from an infiltrating lesion to a well-circumscribed, soft tissue mass. CT features typically include a solitary, peripheral, mass, usually in the lower lobes. Local invasion and primary involvement of the mediastinum and hilar structures are unusual manifestations. CT calcifications within the lesion occur more frequently in children than in adults. They are useful for differential diagnosis if present, but they are usually nonspecific in shape and configuration. Atelectasis and pleural effusion can also occur, but multiple lesions, cavitations and lymphadenopathy are very rare findings [2, 7, 9, 10].
IMT is a low-grade neoplasm, usually affecting the lungs and histologically is distinguished into three types: 1) organising pneumonia pattern, with a mixture of inflammatory cells and fibroblasts; 2) fibrous histiocytic pattern, which is the most common, and is characterised by spindle-shaped myofibroblasts arranged in whorls; and 3) lymphohistiocytic pattern, which is the least common [2]. Immunohistochemistry allows the differential diagnosis from other lymph hyperplastic diseases. Moreover, cytogenetic disorders in the anaplastic kinase lymphoma gene in 2p23, resulting in overexpression of ALK, has been observed in 40% of cases [2, 7, 11]. In our case, based on the histopathological report, rare diseases such as solitary fibre tumour, synovial sarcoma of pleura, fibromatosis and fibrosclerosing lesions were included in differential diagnosis [1].
Noteworthy, IMT and IgG4-related disease can involve virtually every organ, with both disorders characterised by a rich inflammatory infiltrate. Studies have shown that IMTs with a high inflammatory profile are histologically and immunohistochemically indistinguishable from IgG4-related disease [1].
Conclusion
IMT is a rare, benign neoplasm, usually occurring in young people, with more than half of patients under 40 years of age. Besides its benign behaviour, local invasion, recurrence and distant metastases have also been described. The aetiology and pathogenesis remain unclear. Most theories support an exaggerated inflammatory response to a viral or foreign antigen antibody reaction. Many patients are asymptomatic, with the tumour discovered incidentally on a chest radiograph or thoracic CT scan. There are no specific findings on physical or laboratory examinations. Surgical resection is the procedure of choice for both diagnostic and therapeutic reasons and achieves low recurrence rates. However, other treatment options, such as corticosteroids, nonsteroidal anti-inflammatory drugs, chemotherapy or radiotherapy, are alternative strategies in case of nonsurgical procedure. Treatment with nonsteroidal drugs in ALK− tumours seems to be a safe and effective alternative option with promising clinical outcomes that persist even after ceasing therapy.
Footnotes
Conflict of interest: V. Petta has nothing to disclose.
Conflict of interest: A. Zetos has nothing to disclose.
Conflict of interest: D. Bisirtzoglou has nothing to disclose.
Conflict of interest: M. Salomidou has nothing to disclose.
Conflict of interest: C. Marketos has nothing to disclose.
- Received February 9, 2021.
- Accepted June 6, 2021.
- Copyright ©ERS 2021
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










