





Abstract
What is the diagnosis of this woman with multiple respiratory infections in the previous year and a recent onset of progressive dyspnoea and wheezing? https://bit.ly/3bLgw2A
A 57-year-old Portuguese woman was referred to our hospital for a second opinion due to multiple respiratory infections in the previous year with a recent onset of progressive dyspnoea and wheezing. She indicated there had been no weight loss during this period. She was a former smoker of 15 pack-years who quit 20 years ago. The patient had a medical history of atrial fibrillation and breast cancer that was treated with radiotherapy. These both occurred in the same year, 5 years prior. Moreover, the patient specified that she had “asthma-like” symptoms during childhood. The patient was working as a lawyer and was medicated with bisoprolol 5 mg and montelukast 10 mg, both medications once a day. On examination, wheezes were auscultated in all lung fields, especially in the right upper lobe. Her oxygen saturation was 96% on room air and the chest radiograph revealed no abnormalities (figure 1).

Posteroanterior chest radiograph.
Task 1
What would be your next approach?
a) Initiate oral corticosteroids
b) Initiate bronchodilator therapy
c) Request blood and functional lung tests
d) Request a computed tomography (CT) scan
Answer 1
c.
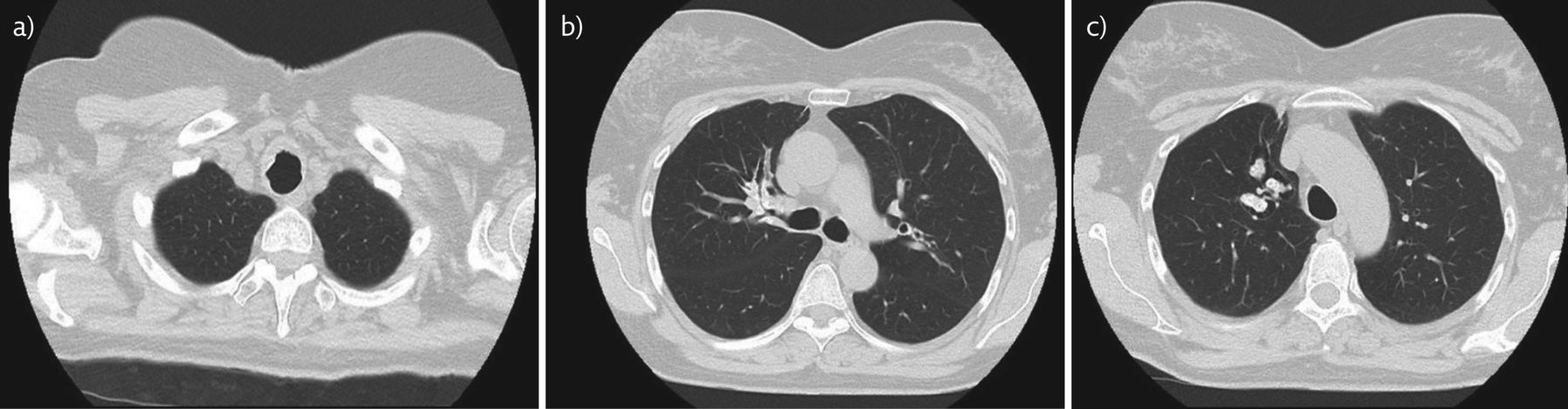
We performed a functional lung test and no obstruction was found, despite a positive bronchodilator response with a ratio of forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) of 74.25, FVC of 2.49 L (80.3%) and FEV1 of 1.95 L (73.8%) (which increased to 2.33 L (88.4%) after bronchodilation challenge with 400 μg of salbutamol). The blood tests were normal. She was initiated on inhaled fluticasone furoate plus vilanterol (200/25 μg) once a day. On our follow-up, 1 month after our first consultation, the patient demonstrated only a slight improvement in dyspnoea, and wheezes were still detected in all lung fields. Another trial was made, this time with budesonide and formoterol (160/4.5 μg), twice a day, with the same poor outcome. The patient presented symptom relief from a 5-day trial of prednisolone 40 mg. Further investigation was undertaken in order to clarify the poor clinical response to bronchodilation despite the good results found in the functional lung test. Her thoracic CT scan can be seen in figure 2.
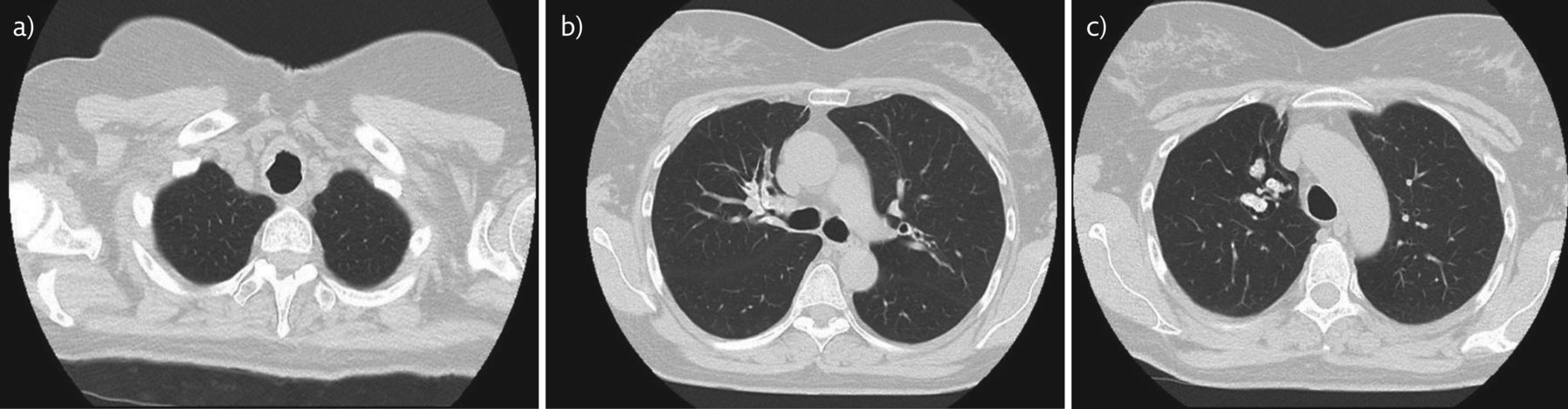
CT scan with a) narrowing of the lumina of the trachea, b) narrowing of the right upper lobe entrance, and c) calcified “finger-in-glove opacities” pattern.
Task 2
Based on the history and chest CT scan, which of the following diagnoses would you investigate?
a) Allergic bronchopulmonary aspergillosis (ABPA)
b) Tracheobronchial amyloidosis (TBA)
c) Tracheobronchopathia osteochondroplastica
d) All the above
Answer 2
d.
The CT scan demonstrated cylindrical and varicose bronchiectasis in the right upper lobe, filled with mucoid impaction and a “finger-in-glove opacities” pattern with diffuse calcifications. These CT scan findings, combined with the patient's history of recurring infections, wheeze and a good response to corticosteroids, were suggestive of ABPA. The CT scan also revealed diffused bronchial thickening mainly in the right upper lobe and in the anterior upper third of the trachea, so the differential diagnoses of TBA and tracheobronchopathia osteochondroplastica were also considered.
Task 3
What would be your next step in the investigation of ABPA?
a) Specific blood test plus prick test
b) Bronchoscopy
c) Initiate corticosteroid
d) Initiate corticosteroid plus antifungal medication
Answer 3
a.
There is a lack of consensus on the minimum criteria, either major or minor, required for the diagnosis of ABPA. To overcome this issue, the International Society for Human and Animal Mycology (ISHAM) established a working group in 2011. This group has proposed revised criteria for the diagnosis of ABPA and recognised bronchial asthma and cystic fibrosis as predisposing conditions. The two obligatory criteria are 1) a positive immediate (type I) cutaneous hypersensitivity to Aspergillus antigen or elevated IgE levels against Aspergillus fumigatus, and 2) elevated total IgE levels (>1000 IU·mL−1). Both criteria should be present to make an ABPA diagnosis. The minor criteria include at least two out of the following three: 1) presence of precipitating or IgG antibodies to A. fumigatus, 2) radiographic features in the lungs consistent with ABPA, and 3) peripheral blood eosinophilia (>500 cells·μL−1) in a steroid naïve patient [1, 2].
The role of A. fumigatus real-time PCR in bronchoalveolar lavage is still unclear. In our patient, total IgE blood levels were normal and antigen plus “prick test” for A. fumigatus was negative. Thus, we excluded the diagnosis of ABPA. To proceed with the investigation of the differential diagnoses proposed (TBA and tracheobronchopathia osteochondroplastica) a bronchofibroscopy was performed (figure 3). The examination showed deposits of a yellow material in the anterior wall of the trachea, mainly in the upper third. The same yellow material was found scattered along the airways, causing obstruction of the lumen in the right upper lobe entrance. Bronchoalveolar lavage was sent to bacterial, mycobacterial and mycological culture. All were negative. The tracheobronchial biopsy revealed infiltration of the submucosa with an amorphous hyaline material.

a) Infiltration of the trachea submucosa with yellow material and b) obstruction of the right upper lobe entrance with the same material.
Task 4
In order to complete the diagnosis, which histological stain would you use for this biopsy?
a) Acid fast
b) Periodic acid–Schiff
c) Congo red
d) Sudan black B
Answer 4
c.
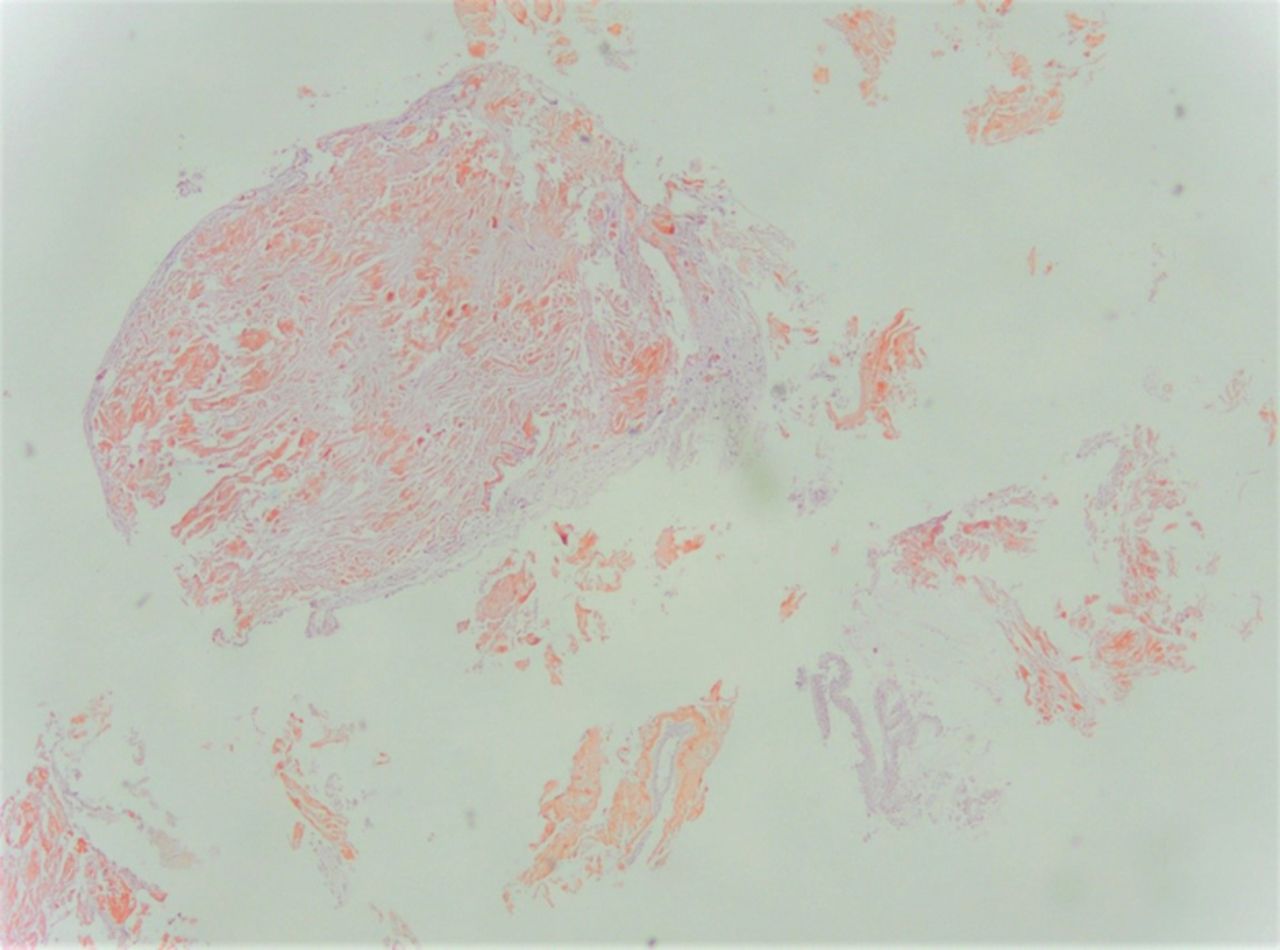
Congo red-stained slides demonstrated amyloid deposits (figure 4). An extensive workup was made to rule out systemic amyloidosis. First, the echocardiogram showed no signs of infiltrative disease and no other organ dysfunction was found, besides the lungs. Secondly, serum protein electrophoresis with immunofixation electrophoresis (IFE) and a 24-h urine collection with urine protein electrophoresis and IFE were normal. Finally, a bone marrow biopsy and myelogram showed no evidence of amyloidosis. These findings were discussed in a multidisciplinary meeting between an internist, a pulmonologist and a haematologist, and the patient was diagnosed with primary localised TBA.
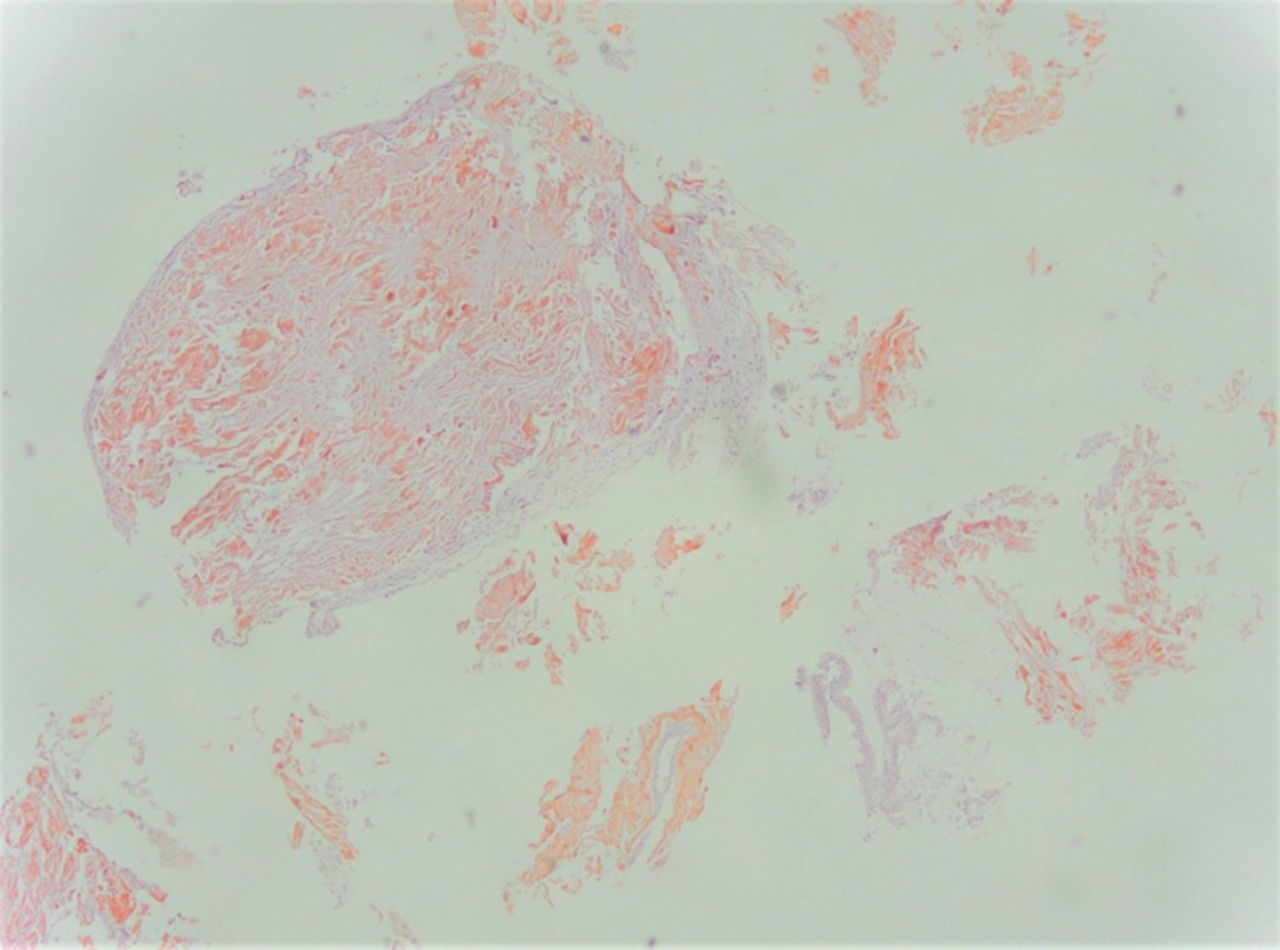
Benign bronchial mucosa with deposition of amorphous hyaline material that stains with Congo red, compatible with amyloidosis.
Task 5
Which treatment would you consider?
a) Conservative treatment with close monitoring
b) Oral colchicine
c) Prednisone and melphalan
d) Bronchoscopic debulking and laser ablation
Answer 5
d.
The patient underwent bronchoscopic debulking and endobronchial ablation by neodymium-doped yttrium aluminium garnet (Nd:YAG) laser. Major amyloid plaques in the trachea were removed. Due to location with difficult access for a rigid bronchoscope, the lesions at the right upper lobe entrance were just partially treated. The patient also started on high doses of budesonide and formoterol inhaled therapy. 1 month after the intervention, the patient exhibited improvement and functional testing revealed an improvement in basal FEV1 results to 2.15 L (82.2%).
After 1 year of close outpatient follow-up with routine bronchoscopies, the patient remains with minor symptoms, controlled only with inhaled therapy, and there has been no need for further oral corticosteroids.
Discussion
Amyloidosis is characterised by the deposition in extracellular and/or intracellular tissues of abnormal proteins in a fibrillar form: the amyloid. These amyloid deposits may cause organ dysfunction [3]. Amyloidosis can be acquired or hereditary, primary or secondary, localised or systemic. The diagnosis of localised primary pulmonary amyloidosis is extremely rare and requires the exclusion of systemic amyloidosis, which accounts for up to 80% of pulmonary amyloid lesions. This form of lung amyloidosis may affect the parenchyma either as a diffuse, interstitial or nodular pattern; the tracheobronchial tree with submucosal plaques, as in our case; or as luminal tumour-like masses [4]. Although a rare disorder, primary TBA is the most common localised form of respiratory amyloidosis. According to the literature, only 0.5% of all symptomatic tracheobronchial lesions are amyloid lesions [3].
Patients with TBA can be asymptomatic or present with symptoms like progressive dyspnoea, cough and wheezing, mimicking other respiratory conditions [5, 6]. This can delay the diagnosis and/or lead to misdiagnosis with other common conditions like asthma or pneumonia. Patients with upper tracheal disease may develop upper airway obstruction, while distal tracheal or main bronchial disease may cause lobar collapse or recurrent airway and parenchymal infections [5]. Our patient had both upper and distal disease, which helps to explain her initial complaints of progressive dyspnoea, recurrent lung infections and wheezing.
Due to the high risk of developing airway obstruction with respiratory failure, the life expectancy for primary TBA is <10 years, with overall survival rate at 4–6 years of 31–43% [7]. These data underscore the importance of an early diagnosis. In individuals with amyloidosis, a CT scan can reveal smooth or irregular nodular thickening of the tracheal wall and bronchi, which can be accompanied by calcified nodules in the submucosa. Therefore, a chest CT scan has proven to be the imaging examination of choice for the evaluation of TBA. As illustrated in this case, the chest radiograph can be normal. The differential diagnoses of diffuse tracheobronchial diseases include granulomatosis with polyangiitis, tracheobronchial papillomatosis, infectious involvement, relapsing polychondritis and tracheopathia osteochondroplastica (table 1) [8, 9].
Key differences between tracheobronchial diseases
Currently, there is no established treatment for endobronchial amyloidosis and clinical trials are needed. Treatment depends upon the patient's symptoms and degree of obstruction. For patients who are symptomatic due to airway obstruction, bronchoscopic debulking and laser ablation are the mainstay of treatment [10]. Amyloid lesions are sensitive to laser photocoagulation. Carbon dioxide laser therapy is usually preferred in upper lesions (supraglottic and glottic), while Nd:YAG is indicated for tracheobronchial deposits.
External beam radiotherapy (EBRT) has been used in a few cases of endobronchial amyloidosis with success. The rationale for this therapy is that plasma cells producing amyloid protein seem to be photosensitive. EBRT could be useful in patients not suitable for bronchoscopic intervention. Cryotherapy has also been used, with a successful result in one case [3].
As far as pharmacological options are concerned, oral colchicine, along with prednisone and melphalan, are usually preferred for the treatment of systemic amyloidosis. Colchicine inhibits the microtubular system during the metaphase and decreases monocyte and neutrophil chemotaxis creating an anti-inflammatory effect. Unfortunately, there is a difference in the pathogenesis of systemic and local amyloidosis, and the good results with systemic disease cannot be extrapolated to TBA treatment. Despite that, there are some case reports on the use of colchicine for the treatment of TBA with variable results. In 2016, Morales et al. [11] reported a successful case of TBA treated with colchicine alone.
Bronchodilation therapy is used off label in some cases [3], with the assumption that a local bronchodilation action will reduce stenosis caused by amyloid plaques and provide symptom relief. This effect can be seen in the functional lung tests performed by our patient, with a positive bronchodilator response to salbutamol. We added inhaled corticosteroid (budesonide) to a long-acting β2-agonist (formoterol), with the intention of adding an anti-inflammatory local action in addition to bronchodilation to overcome the partial stenosis that remained, after intervention, in the right upper lobe entrance. More studies are required to establish an efficient pharmacological approach to TBA.
Footnotes
Conflict of interest: B. de Aguiar Mendes has nothing to disclose.
Conflict of interest: J.D. Santos has nothing to disclose.
Conflict of interest: C.L. Figueiredo has nothing to disclose.
Conflict of interest: M. Calheiros Cabral has nothing to disclose.
Conflict of interest: R.L. Santos Gerardo has nothing to disclose.
Conflict of interest: M.A. Mineiro has nothing to disclose.
Conflict of interest: J.A.D. Cardoso has nothing to disclose.
- Received March 2, 2021.
- Accepted May 19, 2021.
- Copyright ©ERS 2021
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.











{kind=link}
{kind=link}
{kind=link}
{kind=link}