





Abstract
Knowing the limitations of reference equations is essential to minimising errors in diagnosis and clinical management. Choice of reference sets may impact access to treatment options where lung function based eligibility criteria exist. https://bit.ly/2WdOFDj
Case history
A 69-year-old man with idiopathic pulmonary fibrosis (IPF) is undertaking routine lung function testing prior to clinical review and assessment for consideration of antifibrotics. As he lives in Australia, the pulmonary function eligibility criteria for antifibrotics are forced vital capacity (FVC) ≥50% of predicted and transfer factor of the lung for carbon monoxide (TLCO) ≥30% of predicted in the absence of obstruction [1].
Questions
Does the patient meet the lung function criteria for antifibrotics based on the lung function results in table 1?
Lung function test results
Are the reference equations used appropriate for this patient?
Answers
Table 1 shows the lung function results of spirometry, static lung volumes (SLVs) and TLCO. Results show a restrictive ventilatory defect as evidenced by a reduced total lung capacity (below the lower limit of normal (LLN) or fifth centile) in the presence of no evidence of obstruction on spirometry (forced expiratory volume in 1 s (FEV1)/FVC >LLN or fifth centile). This is in keeping with the patient's known IPF. TLCO unadjusted for haemoglobin, alveolar volume and the transfer coefficient are all reduced (<LLN or fifth centile), revealing gas exchange impairment suggestive of parenchymal or pulmonary vascular disease. When corrected for haemoglobin, gas exchange (TLCOHbcorr) remains impaired.
The patient's FVC is 48% of the predicted value and TLCO uncorrected for haemoglobin is 29% of the predicted value. Based on these results, the patient does not meet the eligibility criteria for antifibrotics. However, TLCOHbcorr is 30% of the predicted value and if used, would meet the TLCO criterion.
The patient's ethnicity is documented on the report as “other/mixed”. This means he does not identify as one of the four ethnic groups assigned in the Global Lung Function Initiative (GLI) spirometry reference sets. The reference sets used (documented at the bottom of the report) (table 1) are stated as GLI spirometry Caucasian [2], GLI SLVs [3] and GLI TLCO [4]. As the patient identifies as a race other than Caucasian or is of mixed race, the selected spirometry reference set is not appropriate for this patient. Furthermore, the GLI SLV and GLI TLCO reference sets are based on Caucasian data and may also be inappropriate for this patient.
Discussion
The selection of appropriate reference sets is critical to interpretation of results. Incorrect selection of reference equations may impact diagnosis and incorrectly inform clinical management options.
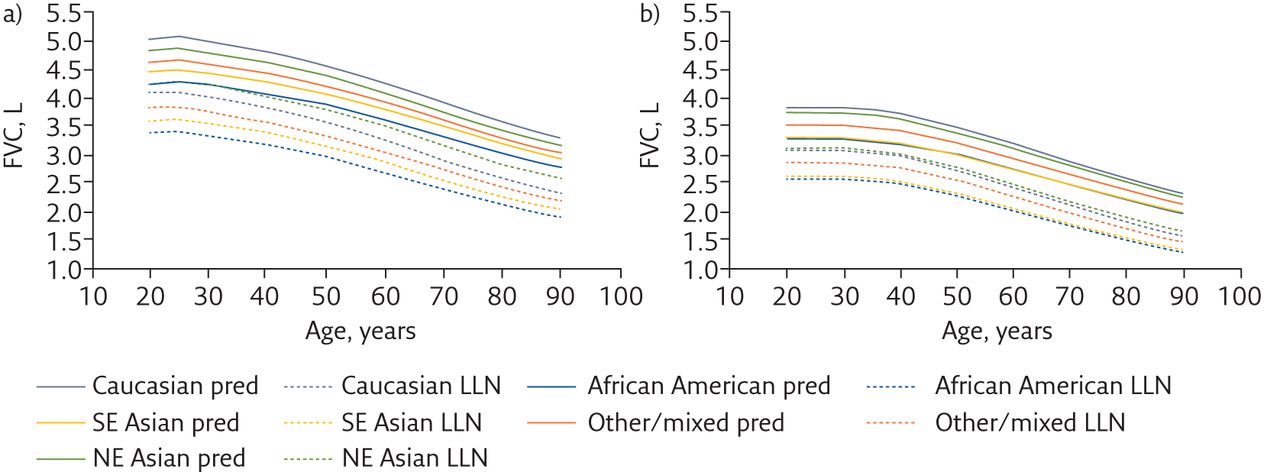
The multiethnic GLI spirometry reference set illustrates differences in lung function based on ethnicity, with Caucasian and North East Asian populations having higher FEV1 and FVC predicted values than South East Asian and African American populations in the study [2]. Figure 1 illustrates the differences. Of note, in the examples shown in figure 1, the North East Asian LLN sits higher than the Caucasian LLN, despite the Caucasian predicted value being higher than the North East Asian predicted value. While this suggests less variation in the North East Asian population used to create the reference equations, it also suggests that using Caucasian reference equations in a North East Asian population may result in underestimation of abnormal findings. Using Caucasian reference values for a person of South East Asian background may result in an abnormal finding simply because the LLN using the Caucasian reference equations is higher than the South East Asian LLN (table 2). Similarly, a person of Caucasian descent may appear to have lung function in the normal range if compared against the South East Asian LLN but be abnormal if compared to the Caucasian LLN.

a) Predicted (pred) FVC and FVC LLN for a 172-cm-tall adult male versus age using the multiethnic GLI equations. b) Pred FVC and FVC LLN for a 163-cm-tall adult female. For both, the “other/mixed” pred FVC and FVC LLN represent the pooled data of the four ethnic groups and sit approximately in the middle of the range of plotted data. Note also that the North East (NE) Asian FVC LLN sits above the Caucasian FVC LLN despite the NE Asian predicted FVC sitting below the Caucasian pred FVC. SE: South East.
Comparison of spirometry results of a 21-year-old, 163-cm-tall female of South East Asian ancestry using GLI South East Asian and Caucasian reference values [2]
In the case presented, the subject has been assigned “other/mixed” for ethnic ancestry as he does not identify with the four defined GLI ethnic groupings or is of mixed ancestry. The GLI “other/mixed” equations represent the combination of the entire data set and hence sit somewhere in the middle of the range (figure 1). Cautionary statements regarding reference equations must be used when “other/mixed” group is selected, as it is unclear whether the reference values are truly representative of the subject's ethnicity and they may be assigned normal or abnormal patterns based on a generalised normal range.
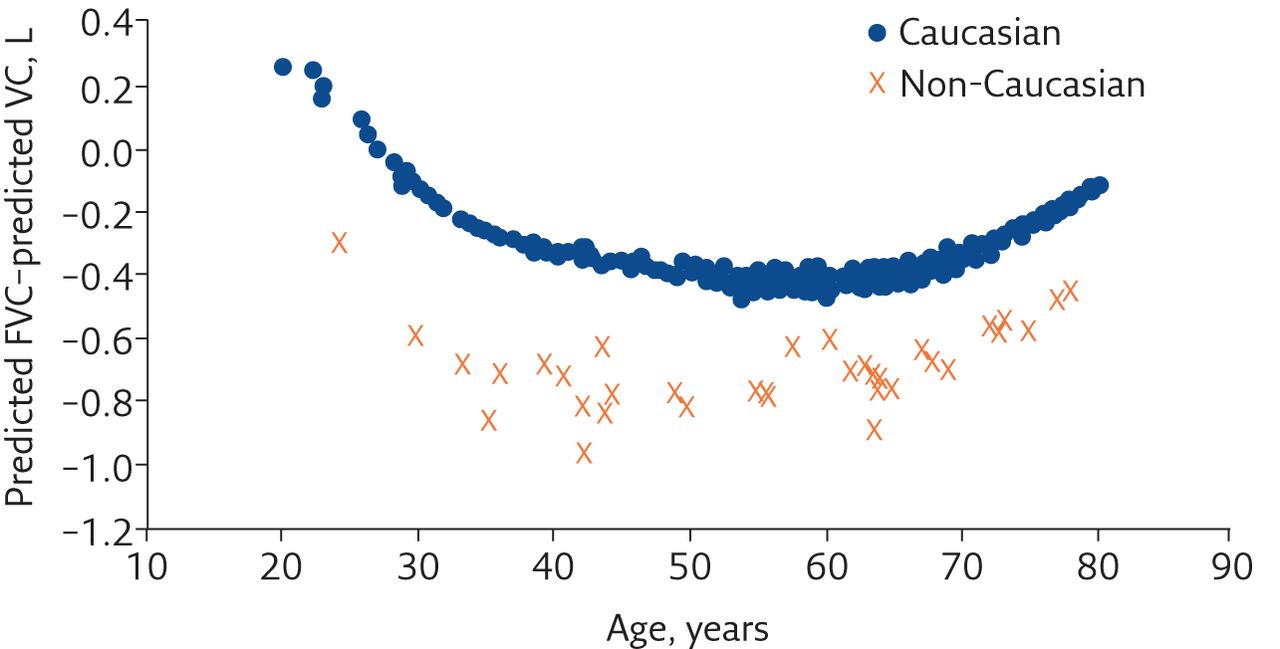
While the GLI spirometry reference set, which has been endorsed for use by many respiratory societies around the world, provides equations for multiple ethnic groups, similar multiethnic reference equations are not available for TLCO or SLV parameters. Whether similar differences in gas exchange and SLV parameters across racial groups exist is still to be determined. However, it is probable that similar findings of racial differences for SLVs exist based on the common parameter of vital capacity (VC). In a normal, healthy cohort without any history of respiratory disease, we expect FVC and VC to be similar. Spirometry data submitted with lung volume data used to create the GLI SLV reference set overall showed small, insignificant deviations from the GLI predicted FVC (mean±sd z-score 0.31±1.00) [3]. Furthermore, equations for VC [3] and FVC [2] were similar [3]. The differences between VC and FVC amplify, however, when using spirometry reference equations other than Caucasian to calculate FVC. Figure 2 shows that the difference between predicted FVC and predicted VC is larger when predicted FVC is calculated using reference equations appropriate to ancestry in a male cohort (n=365) referred to an Australian lung function laboratory for clinical testing (unpublished data). By assigning the “other/mixed” spirometry reference set to the case presented, the predicted FVC and LLN become 3.60 L and 2.72 L respectively, while the predicted VC and LLN are 4.25 L and 3.38 L respectively: a 0.65 L and 0.66 L difference respectively. It is probable that the difference seen between predicted VC and FVC in this case is likely to be reflected in other subdivisions of SLVs too. SLV reference data for ancestry other than Caucasian are sparse and it is unclear how to account for possible differences when using Caucasian reference equations to interpret results of patients with ancestry other than Caucasian. It is incumbent upon reporters of lung function to understand the limitations of the reference sets being used; the use of cautionary statements in reports is strongly recommended where the ancestry of the patient differs from the reference sets used (e.g. reference values used may not be representative of the patient's ethnicity and should be used with caution).

{kind=link}
{kind=link}
In the case presented, the patient has IPF and the medical team are assessing his eligibility to access antifibrotics. Quite apart from the differences in eligibility between jurisdictions around the world, the patient's ability to access the medication may depend on the reference set chosen. Two recent papers have reviewed eligibility for access to antifibrotics based on reference set chosen. Ward et al. [5] looked at the proportion of English and Scottish patients with IPF who were eligible for antifibrotics dependent on reference sets chosen. Eligibility in England and Scotland at the time of the study was FVC ≤80% of predicted. The eligibility criteria did not state which reference values should be used. Approximately 34 out of 98 patients (total n=528) who were ineligible for treatment using the European Community for Steel and Coal reference set [6] to calculate FVC % predicted became eligible when using the Third National Health and Nutrition Examination Survery spirometry reference set [7], and 25 became eligible using the GLI 2012 reference set [2] instead. The second study from Australia, where antifibrotic lung function eligibility criteria is FVC ≥50% predicted and TLCO ≥30% predicted, found variation in eligibility ranged from 74% to 86% dependent on the reference sets chosen [8]. Table 3 shows the variation in FVC % predicted and TLCO % predicted in a selection of commonly used reference sets using the presented case's gender, age and height. Using the GLI spirometry “other/mixed” and TLCO reference equations, the patient (just) meets the lung function eligibility criteria for government-subsidised treatment.
Comparison of FVC and TLCO % predicted (pred) across reference sets for a 69.8-year-old, 171.8-cm-tall male of “other/mixed” ancestry as per the GLI with measured FVC 1.89 L and TLCO 2.45 mmol·min−1·kPa−1
Conclusion
It is essential for persons reporting lung function to know the reference sets being used and understand the limitations reference sets may have. Consideration of the impact of using reference sets that may not be representative of the patient's ethnicity or race is necessary and cautionary statements should be used in lung function reports where this occurs. The choice of reference set may impact the eligibility for patients to access government-subsidised medications where lung function criteria are based on percent of predicted value.
Key points
Knowing the limitations of lung function reference sets and understanding the impact of the limitations are essential to interpretation of lung function data.
The multiethnic GLI spirometry reference equations demonstrate clear differences between groups. It is not clear how to use the Caucasian-based GLI TLCO and SLV reference sets in people not identifying as Caucasian.
Use cautionary statements to identify limitations of reference sets in reports.
Choice of reference sets may impact patients seeking access to treatment with lung function related eligibility criteria.
Self-evaluation questions
Which GLI reference equations provide multiethnic capability?
a) SLV
b) Spirometry
c) TLCO
d) All the above
Which spirometry GLI reference equations apply when the ethnic origin is not known?
a) Caucasian
b) Caucasian×0.88
c) South East Asian
d) African American
e) Other/mixed
The “other/mixed” GLI spirometry reference equations are derived from:
a) Submitted data of individuals who did not identify as Caucasian, North East Asian, South East Asian or African American
b) All the GLI spirometry data combined
c) Caucasian and African American datasets only
d) North East and South East Asian datasets only
Suggested answers
1. b.
2. e.
3. b.
Footnotes
Conflict of interest: B.M. Borg is co-author of a book Interpreting Lung Function Tests: A Step-by-Step Guide for which they receive royalties (Wiley-Blackwell Publishing). B.R. Thompson is co-author of a book Interpreting Lung Function Tests: A Step-by-Step Guide for which they receive royalties (Wiley-Blackwell Publishing).
- Received June 28, 2021.
- Accepted August 11, 2021.
- Copyright ©ERS 2021
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










