





Abstract
Sleep disturbances are common in pregnancy and affect sleep quality. The maternal body is going through constant physical and physiological changes to adapt to the growing fetus. Sleep disorders may manifest at any point during pregnancy; some may result in adverse maternal or fetal outcomes. A strong clinical suspicion is crucial to identify sleep disorders in pregnancy and their management should be evaluated with a multidisciplinary team approach. In this review, we provide an overview of changes in sleep during pregnancy and summarise the key features of common sleep disorders in pregnancy, including practical tips on their management.
Educational aims
To provide an overview of common sleep disorders in pregnancy and their management options.
To highlight the impact of the physiological changes in pregnancy on sleep.
To outline the type of sleep studies available to investigate sleep disorders in pregnancy.
Abstract
Sleep disturbances are common in pregnancy and may result in adverse maternal or fetal outcomes. A strong clinical suspicion is crucial to identify sleep disorders in pregnancy and their management requires an effective multidisciplinary team approach. https://bit.ly/3vwBF9V
Introduction
Sleep is an essential process that helps to maintain physical and psychological health. During sleep, additional loads are imposed onto the respiratory muscle pump, and these may be amplified during pregnancy due to the hormonal, physiological, anatomical and psychological changes that occur. In this review article, we will provide an overview of physiological changes that occur during pregnancy that may affect sleep, and then summarise the epidemiology, pathophysiology and management of common sleep disorders in pregnancy.
Sleep disturbance in pregnancy
Subjective sleep disturbance, poor sleep quality, insufficient night-time sleep, daytime sleepiness and night-time awakenings, are reported in up to 76.3% of pregnant women, with the prevalence rising to 83.5% after 8 months of gestation, according to an online questionnaire of 2427 pregnant women [1]. Sleep disturbance may arise throughout pregnancy, in both early and later stages, and is a dynamic process [2]. Indeed, observational data from a large Danish cohort identified that 38% of pregnant women reported at least one sleep complaint in the first 16 weeks of gestation, with waking up too early observed to be the most common complaint [3]. Researchers have studied women from pre-pregnancy to post-partum and found significant changes in polysomnographic patterns including total sleep time, wake after sleep onset, and sleep efficiency. By the 12th week of gestation, sleep duration lengthens; however, sleep quality deteriorates compared with the first trimester. Pregnant women reported their sleep to be subjectively of poorer quality, with increased wake after sleep onset [4, 5]. The Pittsburgh Sleep Quality index (PSQI) is a self-rated questionnaire, commonly used to assess sleep quality and patterns of sleep. A global PSQI of five or more indicates poor sleep quality [6]. A meta-analysis of the prevalence of poor sleep quality during pregnancy indicated a rising PSQI between the second and third trimester [7].
Hormonal and physiological changes in pregnancy
Maternal oestrogen and progesterone increase substantially from the beginning of the pregnancy and may affect the sleep cycle. Their effect on maternal sleep is complex and animal models have displayed their influence on rapid eye movement (REM) and non-REM sleep [8, 9]. Apart from hormones, gastro-oesophageal reflux is recognised in up to 75% of pregnant women [10]. This may also contribute to sleep disruption and is thought to be related to oesophageal dysmotility, increased gastric compression from the fetus, reduced gastro-oesophageal sphincter pressure and high maternal oestrogen level [11]. Frequent nocturnal micturition can lead to fragmented sleep and this can be explained by renal hyperfiltration, decreased bladder capacity from external compression and an increased urine volume from salt accumulation [11]. One study showed frequent visits to the toilet was the most common cause of sleep disruption during pregnancy [12]. Nausea, vomiting, musculoskeletal pain and inability to adopt a habitual sleeping posture could also lead to frequent nocturnal arousals. There is ongoing research into potential inflammatory biomarkers associated with sleep architecture and maternal–fetal outcomes, and this remains an area for research purposes only.
Tools used in sleep assessment
Sleep quality may be evaluated using subjective and objective measurements. Questionnaires commonly employed in both clinical practice and research include the Epworth Sleepiness Scale (ESS), the STOP-BANG questionnaire, the Berlin questionnaire, the PSQI, the Insomnia Severity Index (ISI), the International Restless Legs Syndrome Rating Scale and the Global Sleep Assessment Questionnaire. The ESS is commonly used to assess daytime somnolence and is routinely used as part of the assessment of sleep disordered breathing (SDB). A score of 11 or more indicates excessive daytime sleepiness (EDS) [13]. The STOP-BANG questionnaire is designed to screen for obstructive sleep apnoea (OSA) in adults. The Berlin questionnaire consists of 10 questions and is a brief and validated screening tool designed to identify individuals who are at high risk for sleep apnoea [14]. As previously discussed, the PSQI is a self-evaluated questionnaire to assess sleep quality and disturbances over the past month. The ISI consists of seven questions. It assesses the nature, severity and impact of insomnia and may be used to monitor treatment response. The International Restless Legs Syndrome Rating Scale is used to assess severity and treatment response in patients with restless legs syndrome (RLS). The Global Sleep Assessment Questionnaire comprises 11 items and is used to screen for multiple sleep disorders in the general population in a single questionnaire.
Table 1 describes the objective tests available for sleep measurements. A video polysomnography is the gold standard to evaluate sleep and it involves application of different leads, sensors, electrodes, microphone, and a camera. It provides the most information about an individual's sleep, but its use is limited by high cost and lack of availability. Therefore, other simpler sleep studies are often used instead and some of these studies can be performed in the patient's home.
Types of sleep studies
Sleep disorders in pregnancy
Sleep disordered breathing
SDB is an umbrella term that encompasses a range of conditions in which abnormal respiratory events occur during sleep. The most common forms of SDB that occur during pregnancy include snoring, OSA and obesity hypoventilation syndrome (OHS).
Epidemiology
Snoring is more frequently reported by pregnant women than in non-pregnant women, and increases in prevalence from 11% in the first trimester to 16% by the third trimester [2, 15]. The exact prevalence of OSA in pregnancy is unknown, but is likely underestimated. The apnoea–hypopnoea index (AHI) measures the number of apnoeas or hypopnoeas recorded per hour during a respiratory polygraphy study. The diagnosis of OSA requires polysomnographic evidence of an AHI of at least 5 events per hour. A prospective study that analysed 3705 pregnant women with home respiratory polygraphy identified that 4% had an AHI ≥5 events·h−1 in early pregnancy. This increased to 8% by mid pregnancy [16]. A cohort study by Pien et al. [17] found that 11% pregnant women had an AHI ≥5 events·h−1 in the first trimester, increasing to 28% by the third trimester. They also reported an upward trend of AHI from 2.07 events·h−1 to 3.74 events·h−1 by the third trimester of pregnancy. Women that developed OSA had a higher body mass index (BMI) at baseline [17]. Louis et al. [18] studied 175 clinically obese pregnant women with portable polysomnography; they found 15% had an AHI of ≥5 events·h−1 and this group of patients had a higher mean BMI. Finally, a study of 155 pregnant women with a mean baseline BMI of 29 kg·m−2 found the ESS significantly increased from 8.6 in the first trimester to 10.2 in the month of delivery [19]. These studies demonstrate that the development of OSA is closely linked to gestational age and maternal weight. OHS is a recognised form of SDB. However, prospective clinical trial data evaluating the prevalence and management of OHS in pregnancy are currently lacking. It should be suspected in the obese adult with daytime hypercapnia (partial pressure of carbon dioxide >6 kPa).
Pathophysiology
Pregnancy leads to a range of physiological, anatomical and hormonal changes, some of which may protect against SDB, whilst others can increase the risk of SDB developing. Anatomical changes that occur include narrowing of the upper airway secondary to nasopharyngeal oedema from increased oestrogen and weight gain [11]. These changes can lead to increased airflow resistance and a higher Mallampati score [20]. The Mallampati score is a grading scale based on the visualisation of oropharynx structure; a higher score predicts an increased risk of OSA.
Respiratory physiological changes that occur during pregnancy are largely a consequence of the impact of the gravid uterus on the diaphragm. As a sequel of an increase in the anterior–posterior diameter of the chest and an elevated diaphragm from a raised intra-abdominal volume, the expiratory reserve volume and functional residual capacity decrease progressively during pregnancy [21]. This impairs the force-generating capacity of the diaphragm, which is further exacerbated in the supine position due to caudal displacement of abdominal contents [22].
Maternal progesterone, which rises during pregnancy, is a respiratory stimulant and may help to reduce the risk of SDB. Progesterone has been demonstrated to increase alveolar ventilation by increasing the central ventilatory chemoreceptor sensitivity to carbon dioxide [23]. Conversely, a prospective, randomised, cross-over study by Driver et al. [24] observed that increased neural respiratory drive during the luteal phrase of menstruation may predispose to a reduced upper airway resistance secondary to upper airway collapse. This correlated with the findings of another study, which demonstrated a greater electromyogram activity of genioglossus muscle (a dilator muscle) during the luteal phrase [25].
SDB and maternal and fetal outcomes
OSA in the general population is associated with adverse cardiovascular outcomes including stroke, ischaemic heart disease, hypertension, cardiac arrhythmia, and cardiovascular mortality [26]. In addition, mounting evidence illustrates an association between the presence of SDB and adverse maternal outcomes. A 2010 cross-sectional survey of 1000 American immediate post-partum women showed a positive correlation between symptoms of SDB (snoring, gasping, or choking episodes) and gestational hypertension, gestational diabetes, and increased risk of unplanned caesarean section. Pregnant women that experienced frequent gasping had the highest adjusted odds ratio of 3.6 [27]. Pre-eclampsia has also been shown to be more prevalent in snoring pregnant women [28]. In relation to fetal outcomes of maternal SDB, historical studies have observed a lower infant Apgar score at birth and reduced fetal weight for gestational age [27, 28]. A 2018 meta-analysis supported the presence of an association between SDB and pre-term birth, but did not identify any significant difference in fetal birth weight and Apgar score [29]. Finally, in a prospective observational cohort study of 175 obese pregnant women with OSA, there was an increased risk of neonatal intensive care admission with an adjusted odds ratio of 3.4 [18].
Screening
Screening pregnant women may be helpful to detect SDB, enabling treatment to be instigated, and thereby reduce the risk of associated adverse maternal and fetal outcomes. The area under the curve (AUC) is a measurement of the accuracy of a diagnostic test in separating the group being tested into those with and without the disease in question. An area of 1.0 represents a perfect test and a score closer to 1.0 represents a test with higher discrimination. In the Sleep Disordered Breathing Substudy, 3705 nulliparous pregnant women completed questionnaires at 6–13 weeks’ gestation and 22–29 weeks’ gestation and underwent two six-channel sleep studies. The AUCs of maternal age, BMI and self-reported frequent snoring were 0.81 to 0.87 [30]. Izci-Balserak et al. [31] examined a smaller cohort of pregnant women and found AUCs >0.80 for BMI, maternal age, and presence of tongue enlargement. These findings suggest that these parameters may be useful predictors of the presence of OSA in pregnancy. The validity of existing screening tools in pregnancy have also been explored. Tantrakul et al. [32] reviewed the STOP-BANG and Berlin questionnaires and the overall AUCs were 0.75 and 0.72, respectively. However, their performance reduced dramatically in the first trimester with AUCs of 0.71 and 0.49, respectively [32]. The results showed these questionnaires may be less useful in predicting OSA in early pregnancy. As a result, pregnant women reporting EDS and snoring should be evaluated for possible SDB.
Diagnosis and management of SDB in pregnancy
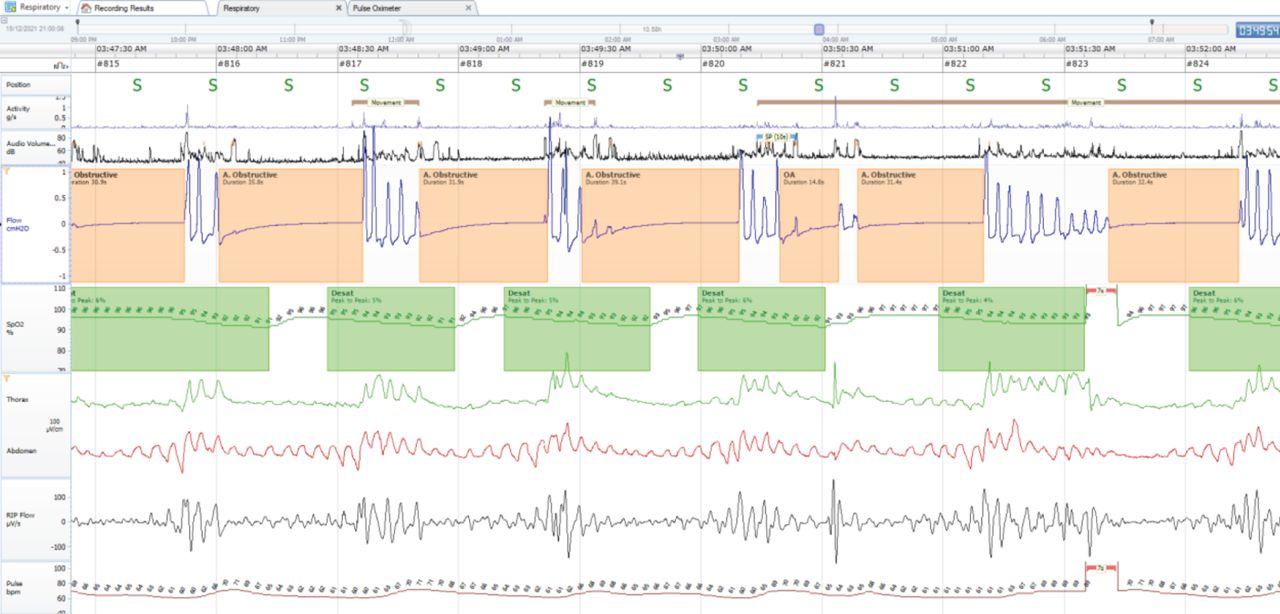
Where there is a clinical suspicion of SDB in pregnancy, a focused history is crucial. This should involve enquiry into the presence of nocturnal symptoms of snoring, witnessed apnoea, dry mouth, nocturnal choking episodes, morning headaches, reflux, nocturia and frequent awakening, as well as daytime symptoms of hypersomnolence, fatigue, non-restorative sleep, cognitive dysfunction and headaches [33]. Some of these symptoms are reliant on reporting from bed partners and regrettably, only a minority of patients attend the sleep clinic with their bed partners, which can affect the validity of the sleep history. Snoring is also underreported in women; a prospective cohort study of 1913 patients showed that 36.5% of women who reported themselves as non-snorers had severe snoring, while only 11.7% of men underreported themselves [34]. The aforementioned validated questionnaires, such as the ESS, may be useful to quantify a baseline score and track changes over time. Objective measurements are then required to confirm the diagnosis. The gold standard test is polysomnography, however, respiratory polygraphy is more commonly available and can accurately provide information on AHI to support a diagnosis of OSA. Figure 1 shows an example of respiratory polygraphy in a patient with OSA. Sleep studies are safe to perform during pregnancy and should be carried out when one suspects SDB. If OHS is suspected, an arterial blood gas should be performed to identify the presence of daytime hypercapnia. This may be followed by overnight measurement of transcutaneous carbon dioxide.

{kind=link}
Example of respiratory polygraphy in a patient with obstructive sleep apnoea. Episodes of obstructive events followed by hypopnoea events.
There are currently no clinical trial data or published guidelines describing the management of SDB in pregnancy. Clinicians should therefore follow the treatment options recommended in adult guidelines, with the exception of recommending weight loss, which should not be advised during pregnancy. Instead, clinicians should support maintenance of physical activity and a healthy diet. Mandibular advancement splints are effective interventions to improve mild sleep apnoea and snoring. These devices consist of plates that apply to both the upper and lower teeth, they move the mandible forward, and thereby improve upper airway patency. However, as discussed earlier, the variable upper airway changes during pregnancy could affect their efficacy and there is limited research on their use in pregnancy. Positional therapy may be considered in positional OSA [35]. A study of 148 third-trimester pregnant women showed this cohort spent 47% of their sleeping time in the supine position and this was associated with a 60% increase in AHI in comparison to non-supine position [36]. Positional therapy prevents the patient from sleeping in the supine position, either using a physical device, such as a specially designed pillow or semirigid backpack, or with a supine vibration alarm device. This approach is only suitable for patients with a higher AHI in the supine position. The UK National Institute for Health and Care Excellence (NICE) guideline on OSA in over 16-year-olds recommended continuous positive airway pressure (CPAP) as first-line therapy in adults with symptomatic mild OSA or adults with moderate and severe OSA [37]. To date, there are no randomised controlled trials evaluating the efficacy of CPAP in maternal OSA. A small study by Poyares et al. [38] showed an improvement in blood pressure with CPAP therapy in the first trimester.
In summary, pregnant women may develop a range of SDB including snoring, OSA or OHS during pregnancy. These are associated with adverse maternal and fetal outcomes, and so should be screened for routinely throughout pregnancy. Data specific to pregnant subjects are limited; therefore if SDB is detected, standard international guidelines should be adhered to, including positional treatment and CPAP.
Insomnia
Insomnia is common and highly prevalent. An epidemiological study of 3073 adults in 2020 reported 14% of adults without insomnia developed insomnia at 5-year follow-up, with higher incidence observed in women (18%) than in men (10%) [39]. A prospective cohort study suggested 38% of pregnant women have insomnia and this rose to 54% by the third trimester of pregnancy [40]. Insomnia has both psychological and physical implications, with associations with depression, anxiety, coronary artery disease and hypertension all reported [41, 42]. Risk factors for pregnancy-associated insomnia that have been identified in prospective studies include pre-gestational insomnia, obesity and depressive symptoms [43, 44].
A diagnosis of insomnia is made using criteria from the International Classification of Sleep Disorders [45]. Information is gathered from patients’ descriptions of difficulty initiating and maintaining sleep despite adequate opportunity and circumstances for sleep, with consequent daytime implications including fatigue, somnolence, poor concentration, memory impairment and/or mood disturbance. There are two forms of insomnias: acute/short-term insomnia presents with symptoms for less than 3 months, whereas patients with chronic insomnia complain of symptoms for at least 3 months. Evaluation should include use of prescribed and over-the-counter drugs, together with an exploration of nicotine, caffeine and alcohol intake, and sleep hygiene practices. The ISI, developed by Morin in 1993, has been widely used to screen and evaluate treatment response [46]. It involves seven domains and assesses the severity of difficulties with sleep onset, sleep maintenance, early awakening and the impact of insomnia on the individual. Okun et al. [47] compared the ISI with a self-reported sleep diary, wrist actigraphy and the PSQI in pregnant women. They found a variable sensitivity but a specificity of more than 85% in most of the domains [47]. Sleep diaries are the mainstay of both diagnosis and treatment, and should be completed daily by patients before review by the treating clinician. Actigraphy is also used in some centres to assess wakefulness by measuring body movement and light exposure, although this is certainly not required for the diagnosis.
The European Sleep Research Society has produced a guideline for the treatment of chronic insomnia in adults [48]. Although the guideline does not focus on insomnia in pregnancy, its recommendations may be safely applied in this group. These include education on good sleep hygiene and the use of cognitive behavioural therapy for insomnia (CBT-I). Good sleep hygiene includes developing a consistent sleep/wake schedule, ensuring a disruption-free sleeping environment, avoiding daytime naps, undertaking regular exercise, and developing a relaxing pre-sleep routine. CBT-I comprises strategies to aid relaxation and reduce cognitive arousal, as well as behavioural strategies, including sleep restriction and stimulus control therapy. Computerised CBT-I employs the same techniques as CBT-I but is delivered as a self-help guide via the internet. A single-site randomised controlled trial that studied 91 third trimester pregnant women showed a significant reduction in the ISI and PSQI after women underwent a full programme of CBT-I [49].
Benzodiazepines and non-benzodiazepines “Z” drugs (zopiclone and zolpidem) are commonly used in treating non-pregnant patients with acute insomnia. Their use in pregnancy is limited due to potential teratogenicity, and fetal withdrawal symptoms. Huitfeldt et al. [50] reviewed data from a large population-based cohort study of 114 234 pregnancies and found the exposure of these drugs were associated with lower birth weight, lower gestational age at delivery and higher risk of pre-term delivery. Their use should therefore be evaluated on a case-by-case basis and neonatal risk should be balanced against the risk of untreated maternal symptoms. Pharmacological therapy should in general be avoided and should only be used after thorough assessment, including careful review of sleep hygiene practices and exclusion of other common sleep disorders, such as restless legs and/or SDB.
Sleep-related movement disorders
Restless legs syndrome and periodic limb movements
RLS is defined as the irresistible urge to move the limbs (usually the legs) in response to an unpleasant sensation and typically relieved by movement. The diagnostic criteria are outlined in the International Classification of Sleep Disorders [45]. This sensation usually occurs at night, prior to sleep onset. The term secondary RLS is used when RLS is linked with another condition or comorbidity, which include pregnancy, iron deficiency, end-stage renal disease and frequent blood donations. An observational study that involved 642 pregnant women revealed 26% were affected by RLS during their pregnancy, and the symptoms were worse as pregnancy progressed and resolved rapidly post-partum [51].
RLS may coexist with periodic limb movement in sleep (PLMS), which manifests as repetitive stereotyped movements, usually consisting of rhythmic toe extension with dorsiflexion of the ankle and flexion of the knee. RLS and PLMS may affect sleep quality by triggering nocturnal awakening, early morning awakening, decreased sleep duration and EDS [52]. The pathophysiology of pregnancy-related RLS is yet to be fully established. Associations with iron and folate deficiencies, dopamine insufficiency and hormonal changes with altered oestrogen, progesterone and prolactin levels have been proposed [51, 53]. Family history and multiparity are recognised risk factors [54]. Severity of RLS can be monitored subjectively by using the International Restless Legs Syndrome Severity Scale (IRLSS): a higher score indicates worse symptoms.
Treatment of pregnancy-related RLS is typically short-term as most symptoms resolve after delivery. Non-pharmacological measures, including good sleep hygiene, smoking avoidance, reduction of caffeine/alcohol consumption and regular exercise, are recommended. Similar to non-pregnant patients, a careful medication review should be performed, and dopamine antagonists, antipsychotics and sedating-antihistamine should be avoided where possible. NICE recommends walking and stretching affected limbs, application of heat with heat pads/hot bath, relaxation exercises and massaging affected limbs to relieve attacks of RLS, and these measures can be safely implemented in pregnancy [55]. A randomised controlled trial showed a reduction in IRLSS in the group that used a foot-massager, heat therapy and a foot-massager with heat therapy, when compared with no intervention [56]. The first-line preventative pharmacological option is oral iron supplementation if serum ferritin level is <75 μg·L−1. Intravenous iron replacement may be considered for refractory pregnancy-related RLS during the second or third trimester of pregnancy if there is failure of oral iron and serum ferritin level is <30 μg·L−1 [57]. For refractory pregnancy-related RLS, there is limited evidence and safety data to support the use of the standard pharmacological therapies in idiopathic RLS, namely non-ergot-derived dopamine agonists (e.g. pramipexole, ropinirole, rotigotine patch), alpha-2-delta ligands (e.g. pregabalin, gabapentin), opioids (e.g. codeine, tramadol, oxycodone) and benzodiazepines (e.g. clonazepam).
Sleep-related leg cramps
Sleep-related leg cramps (SRLC) manifests as a sudden, involuntary painful muscle contraction in the foot or legs that occur during sleep lasting from seconds to minutes. They are usually relieved by flexion of the affected muscle groups. SRLC can be idiopathic or secondary to drugs, peripheral vascular disease, liver cirrhosis, neurological conditions and metabolic disturbances such as hypokalaemia, hypocalcaemia or hypomagnesaemia. SRLC is recognised as one of the common mimics of RLS; other recognised mimics are positional discomfort, venous stasis, leg oedema and neuropathies [57]. The pathophysiology of SRLC is unclear; regular alcohol consumption of at least once a week or spinal disinhibition have been postulated [58, 59]. It can occur in up to 30% of pregnancies, although the reason for this increased prevalence in pregnancy remains undefined [60]. There is scant evidence for the efficacy of pharmacological therapy in treating SRLC; results following the use of magnesium salts and multivitamin supplements are conflicting [61, 62]. Stretching and massaging the muscles during a cramp may help, and regular calf-stretching exercises may help to reduce cramp frequency.
Narcolepsy
Narcolepsy is a primary central disorder of hypersomnolence with two phenotypes. Narcolepsy type 1 is characterised by chronic EDS, cataplexy, sleep-onset REM sleep episodes (SOREMs) and cerebrospinal hypocretin deficiency. Narcolepsy type 2 is characterised by EDS, SOREMs without cataplexy or decrease in cerebrospinal hypocretin [45]. There are two peaks of onset, with a first peak occurring at 14.7 years and a second peak occurring at 35 years [63]. Therefore, although the conditions are rare, clinicians should be alert to the possibility of a de novo onset in pregnancy.
The pathophysiology of narcolepsy involves loss of hypocretin-producing neuropeptide in the hypothalamus due to a probable autoimmune mechanism [64]. To confirm the diagnosis, patients should undergo full polysomnography to exclude coexisting intrinsic sleep disorders, and a multiple sleep latency test (MSLT). An MSLT must be performed the morning after a full polysomnogram to be valid. Patients are asked to take four to five scheduled naps over 2-h intervals and the time it takes for patients to fall asleep is measured, as well as the occurrence of REM sleep in any of the nap opportunities. An MSLT finding of a mean sleep latency of <8 min and >1 SOREMs supports a diagnosis of narcolepsy. Measurement of hypocretin level in the cerebrospinal fluid is the most sensitive and specific test for narcolepsy type 1.
Significance of narcolepsy in pregnancy
A retrospective cohort study showed caesarean section was performed more frequently in pregnant women with narcolepsy type 1 than narcolepsy type 2 and, in this cohort, 10% of subjects with narcolepsy type 1 experienced cataplexy during delivery [65]. A retrospective case–control study of fetal outcomes in narcolepsy type 1 showed the Apgar score, length and weight of the newborns were within normal range but newborns from mothers with narcolepsy type 1 had a significantly higher weight. The author also reported a higher incidence of gestational diabetes reported in pregnant subjects with narcolepsy type 1 [66].
Management of narcolepsy in pregnancy
Treatment of narcolepsy in pregnancy is challenging and these individuals should be managed by specialist sleep teams, working closely with obstetric colleagues. The general approach is similar to that employed in the general population and includes scheduled naps, regular physical activities, sleep hygiene and self-help groups/web-based resources. “Narcolepsy UK” is a charity that provides abundant online resources and a telephone helpline for patients and carers. The drug safety profiles of the commercial pharmacotherapy are limited. A survey completed by 34 clinicians worldwide in 2011 showed a majority of the clinicians stopped the narcolepsy medications at the time of conception and during pregnancy due to presumptive teratogenic risks [67].
The 2021 European guideline and expert statement on the management of narcolepsy in adults and children recommends the cessation of all drugs to treat narcolepsy before any planned pregnancy because of the teratogenic potential of all drugs used in the treatment of narcolepsy [68]. The guideline acknowledges that such discontinuation will nearly always have an adverse effect on symptom control, which can be particularly challenging prior to successful conception. If total discontinuation of drug therapy is thought not practicable, the authors recommend treatment is limited to monotherapy [68]. The use of medications to treat EDS and cataplexy in pregnancy should therefore be planned by expert clinicians, working in multi-professional teams, including sleep specialists and obstetricians, and should be reviewed on an individual basis. Medications should only be prescribed if the benefits outweigh the risks. Unfortunately, a survey of 182 pregnant women with narcolepsy indicated medication counselling was often poorly performed, 37% did not receive any counselling about risk and benefits of pharmacotherapy during pregnancy and 41% stopped their medications during pregnancy [69].
Modafinil is a wakefulness promoting stimulant and is prescribed to reduce EDS. The UK Medicines and Healthcare products Regulatory Agency (MHRA) issued a safety alert in 2020 due to the potential for increased risk of congenital malformation, such as congenital heart defects, hypospadias and orofacial clefts, with modafinil. The MHRA advise against the use of modafinil in pregnancy and recommends a 2-month washout period prior to planned conception [70]. Damkier and Broe [71] evaluated Danish national health registries on first trimester exposure to modafinil and showed an adjusted odds ratio of 2.7 when compared to unexposed pregnancies. Wake promoting stimulants are also widely prescribed in attention deficit hyperactivity disorders and studies have been conducted to explore the safety profile of these medications in this cohort. Huybrechts et al. [72] showed methylphenidate use in pregnancy was associated with an adjusted relative risk of 1.28 for cardiac malformations. Sleep specialists should review the available literature to provide the best available evidence to patients. This illustrates the importance of close liaison between sleep specialists, the obstetric team and pharmacy colleagues in the management of pregnant women with narcolepsy.
Parasomnia
Parasomnias are sleep disorders characterised by abnormal complex physical or behavioural events that occur at sleep onset, within or during arousals from sleep. The International Classification of Sleep Disorders has divided parasomnias into three groups: non-REM related, REM related and other [45]. The epidemiology of parasomnia in pregnancy is uncertain. In a prospective study, pregnant women reported more disturbing dreams and three times more pregnant women reported nightmares occurring more than once a week, compared with non-pregnant women [73]. A prospective study conducted by Nielsen and Paquette [74] suggested a mixed prevalence of dream-associated behaviours such as movement in bed whilst asleep, sleep talking, hypnogely and sleep terror in null gravida, pregnant and post-partum women. Hedman et al. [75] described parasomnias such as sleep talking, sleep walking, nightmares and hypnagogic hallucination declined as pregnancy advanced in their study cohort of 325 pregnant women.
Much like the management of other sleep disorders, the initial management of parasomnia involves exclusion of coexisting comorbid sleeping disorders and recognition of precipitating factors. There is scant data on the use of pharmacological therapy in parasomnia during pregnancy. Benzodiazepines and antidepressants are the mainstays of treatment in non-pregnant patients with parasomnia; however, their use is limited by the absence of sufficient safety data in pregnancy.
Conclusion
Sleep disorders are common in pregnancy and are associated with important maternal and fetal consequences. In general, sleep quality worsens during pregnancy. The incidence of SDB, snoring, insomnia and RLS all increase as pregnancy advances. Sleep disruption can arise from early pregnancy; hence, sleep should be evaluated throughout antenatal care. The care of pregnant women with sleep disorders should be delivered in a multidisciplinary manner, involving obstetricians, pharmacists, sleep physicians and general practitioners.
Key points
Sleep disruption is common during pregnancy and can have important implications for maternal and fetal health: clinicians should be alert to symptoms of common sleep disorders in this group.
Pregnant women with advanced maternal age, higher BMI, and self-reported frequent snoring should be assessed for sleep disordered breathing.
Restless legs syndrome is common during pregnancy and serum ferritin level should be measured and iron replacement provided where ferritin is <75 μg·L−1.
There is limited research and data on the management of sleep disorders in pregnancy. Clinicians should assess and manage these patients with care and in a multidisciplinary setting.
Self-evaluation questions
Which of the following are recognised treatments for the management of RLS? (choose all that apply)
a) Iron supplementation if serum ferritin is <75 μg·L−1
b) Avoidance of caffeine and nicotine
c) Regular light exercise
d) Benzodiazepines
In 2020, the MHRA issued a drug safety alert related to pregnancy, for which of the following drugs?
a) Levodopa
b) Ropinirole
c) Modafinil
d) Solriamfetol
e) Sodium oxybate
The functional residual capacity decreases in pregnancy.
a) True
b) False
Which of the following is the recommended first-line treatment for moderate, symptomatic OSA?
a) Mandibular advancement splints
b) Positional therapy
c) Continuous positive airway pressure
d) Surgery
Suggested answers
a, b, c.
c.
a.
c.
Footnotes
Conflict of interest: Nothing to disclose.
- Received January 10, 2022.
- Accepted April 13, 2022.
- Copyright ©ERS 2022
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










