





Abstract
With recent therapeutic advances in care, people with cystic fibrosis (CF) are living longer and healthier lives. Development of the cystic fibrosis transmembrane conductance regulator (CFTR) modulator therapies has led to improved function of the CFTR protein resulting in improved lung function, decreased rates of pulmonary exacerbations and improved nutritional status for the majority of people with CF. Given improved quality and quantity of life, more people with CF are considering becoming pregnant than ever before. Since the first reported pregnancy in a woman with CF in 1960, the management of pregnancy in CF has been of increased interest and is an active field of research.
In this review, we aim to discuss the management of pregnancy in CF. We discuss the optimisation of preconception health, management of maintenance CF therapies, and use of CFTR modulators during pregnancy and lactation. We also describe the management of pulmonary exacerbations during pregnancy as well as the unique management of pregnancy in a post-transplant patient with CF.
Educational aims
To describe considerations for optimisation of preconception health.
To describe the management of chronic CF therapies including CFTR modulators during pregnancy and lactation.
To describe treatment of an acute pulmonary exacerbation during pregnancy.
To describe the management of pregnancy in individuals with CF following organ transplantation.
Abstract
With recent therapeutic advances in care, more people with CF are pursuing pregnancy. Managing pregnancy in CF focuses on preconception health with judicious use of chronic maintenance therapies and CFTR modulators throughout pregnancy and lactation. https://bit.ly/3qLDSNa
Introduction
Cystic fibrosis (CF) is an autosomal recessive genetic disorder characterised by absence or dysfunction of the cystic fibrosis transmembrane conductance regulator (CFTR) gene. It affects more than 80 000 people worldwide [1]. CF results in pulmonary and extrapulmonary manifestations, which decrease both the quality and quantity of life for people with CF [2]. With the development of CFTR modulator therapies, improved function of the CFTR protein is made possible. Widespread use of CFTR modulators has resulted in improved lung function, nutritional status, pulmonary exacerbations, need for hospitalisation secondary to CF-related complications and overall survival [3–7]. Individuals ≥18 years of age now make up more than half of the global CF population [2, 8, 9], and more people with CF are considering pregnancy than ever before.
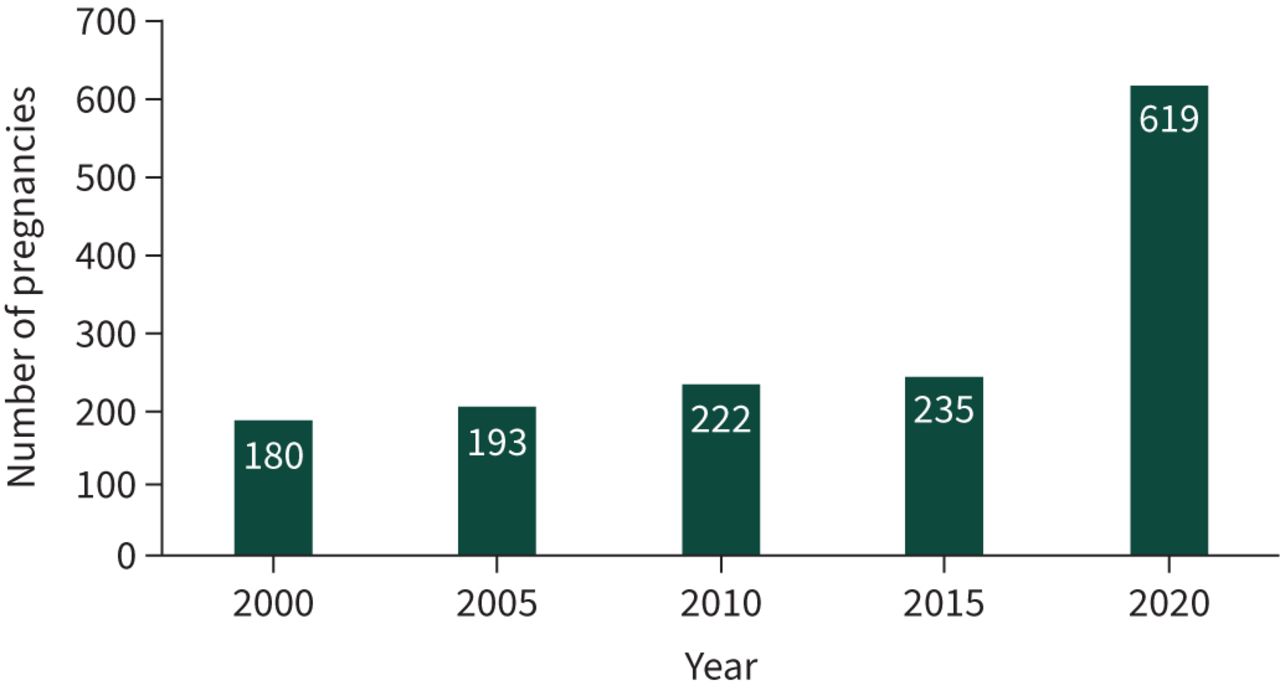
Since the first reported pregnancy in a woman with CF was reported in 1960 [10], therapeutic advances in care have made it possible for people with CF to have healthy and successful pregnancies. With approval of CFTR modulators for the majority of people with CF in 2019, there has been a substantial increase in the number of pregnancies observed in people with CF. In the USA, Cystic Fibrosis Foundation Patient Registry (CFFPR) data have shown annual rates of pregnancy to be between 200 and 310 from 2010 to 2019. In 2020, however, this number nearly doubled with a total of 619 pregnancies reported (figure 1) [2]. The number of pregnancies in people with CF across the world is expected to rise with widespread use of CFTR modulators. Thus, there is increased interest in the management of pregnancy in people with CF. The European Respiratory Society (ERS)/Thoracic Society of Australia and New Zealand (TSANZ) published a consensus statement on the management of pregnancy in people with CF as well as other chronic airways disease [11]. More recently, a multidisciplinary panel of CF clinicians and women with CF published recommendations on pre-pregnancy, intrapartum and post-pregnancy care for people with CF [3]. Additionally, the maternal–fetal effects of CFTR modulators as well as understanding real-world pregnancy care in CF are areas of active research.

{kind=link}
Number of pregnancies reported in the US Cystic Fibrosis Foundation (CFF) Patient Registry in women aged 14–45 years. Reproduced from [2] with permission. Source of data: cystic fibrosis patients under care at CFF-accredited care centres in the USA, who consented to have their data entered.
In this review, we aim to discuss the management of pregnancy in CF. We discuss the optimisation of preconception health, management of maintenance CF therapies, and use of CFTR modulators during pregnancy and lactation. We also describe the management of pulmonary exacerbations during pregnancy as well as the unique management of pregnancy in a post-transplant patient with CF.
Fertility in women with CF
Many, but not all, women with CF are able to conceive without medical intervention. While the rate of subfertility is 5–15% in the general population, researchers have shown the rate of subfertility to be as high as 35% in a cohort of women with CF, with pancreatic insufficiency and advanced maternal age being risk factors [12]. In addition to the overall impact of CF on a woman's health and nutritional status, CFTR may directly influence female fertility. The CFTR protein acts as both a chloride and bicarbonate channel and thus affects both the hydration and pH of secretions not only in the airways and gastrointestinal tract but also in the female reproductive tract, including vagina, cervix, uterus and fallopian tubes. Normal CFTR function leads to thin, watery secretions in the reproductive tract to facilitate passage of sperm through the cervix and uterus and the alkaline pH impacts capacitation (or activation) of sperm to allow fertilisation of the egg. CFTR modulator therapy may be able to directly reverse some of these barriers to conception in CF [1].
Preconception considerations
With the increasing number of pregnancies being observed in people with CF, discussions regarding pregnancy and parenthood should begin early and occur often. Similar to the management of pregnancy in other chronic illnesses, preconception discussions in people with CF should begin during early adolescence in the paediatric CF care setting and continue into adulthood to allow time for optimisation of preconception health [13, 14]. An integral aspect of preconception health includes genetic testing. Carrier screening should be offered to potential reproductive partners to identify the risk of having an infant born with CF. Next-generation genetic sequencing provides a comprehensive CFTR gene mutation evaluation and is recommended for all potential reproductive partners of people with CF [3, 15]. If the reproductive partner is identified as a carrier, a referral to genetic counselling is recommended to discuss further reproductive options as well as additional diagnostic testing [3].
Nutritional status, glucose control and pulmonary function are important aspects to optimise in people with CF to mitigate maternal and infant morbidity, and often require a multidisciplinary team of CF clinicians and high-risk obstetric expertise. Pancreatic insufficiency, a common extrapulmonary manifestation of CF that impacts up to 85% of individuals, can result in poor nutritional status and weight loss secondary to malabsorption [16]. Poor nutritional status is associated with premature and low birth weight infants [17, 18]. Nutrition optimisation through diet, vitamin repletion and pancreatic enzyme replacement therapies should be a priority in the preconception period. A body mass index (BMI) of at least 22 kg·m−2 is the ideal goal prior to conception [3, 19]. Furthermore, up to 50% of people with CF of gestational capacity have CF-related diabetes (CFRD) [3]. Hyperglycaemia preconception is associated with an increased risk of fetal malformations and hyperglycaemia during pregnancy has been associated with fetal macrosomia, neonatal hypoglycaemia and hyperbilirubinaemia as well as increased caesarean delivery [2, 20]. The mainstay of treatment for CFRD is subcutaneous insulin as oral agents have been shown to be less effective [3]. Thus, adequate glucose control with insulin should be achieved prior to conception as well as throughout the duration of pregnancy with target haemoglobin A1c (HbA1c) of <6.5% at the time of conception and <6.0% during pregnancy [21, 22]. To screen for CFRD prior to pregnancy, woman with CF should have a 75-g oral glucose tolerance test (OGTT) done when pregnancy is confirmed unless they have had a OGTT within the prior 6 months. Gestational diabetes is more common in women with CF, occurring in 10–36% of pregnancies versus in <10% of pregnancies in the general population. Care guidelines for CFRD, which include guidance for pregnant women with and without CFRD, recommend that OGTT should be performed at 12–16 weeks and at 24–28 weeks of pregnancy to screen for development of gestational diabetes [23].
Pulmonary function, as measured by forced expiratory volume in 1 s (FEV1) % predicted, is a commonly used marker of lung health for people with CF. Preconception discussions surrounding the potential impact of pregnancy on lung function, and therefore on both maternal and infant health are needed. Disease severity and the implications for maternal and neonatal outcomes has also been a focus of recent research. When stratified by disease severity, individuals with moderate-to-severe disease (defined as FEV1 ≤60% predicted and/or BMI ≤21 kg·m−2 prior to pregnancy) experience more disease-related complications throughout pregnancy [24]. In addition, studies have shown that more severe disease is associated with a higher risk of preterm delivery, need for caesarean delivery, as well as low fetal birthweight [24, 25]. While lung function may improve with use of CFTR modulators in the preconception period, use of modulator therapies has allowed even those with very severe lung disease to conceive [5], thus potential complications associated with advanced lung disease and pregnancy continue to be important to discuss. Therapies aimed at maintaining lung health, such as inhaled mucolytics and antibiotics during the preconception period should be a priority. In addition, it is important to discuss the potential impact of pregnancy on maternal lung health, including discussion of potential increased morbidity such as more frequent need for acute intervention, prior to conception. Historical reports of the impact of pregnancy on lung function vary. In some historical small, single-centre studies, and in a nested-cohort study and a registry study in which pregnant people had higher baseline lung function than that of those who did not become pregnant, there was no significant difference in lung function in pregnant people with CF when compared from baseline to post-partum follow-up visits [26–29]. However, in a modern cohort, Jain et al. [30] examined the impact of pregnancy on lung function, including the interplay of moderately and highly effective CFTR modulators. The results demonstrated a small (∼2%), but statistically significant decline in FEV1 % predicted in pregnant people not using modulators or using moderately effective modulators that was mitigated by use of highly effective modulators. Future analyses will focus on differences in baseline health status, modulator use by trimester and modulator withdrawal in this cohort [30].
Medication management during pregnancy
Maintenance CF therapies
Chronic maintenance therapies are effective in optimising pulmonary as well as extrapulmonary health in people with CF. The decision to continue or halt chronic CF therapies during pregnancy and lactation requires an open discussion in order to weigh the possible implications for the mother as well as for the developing fetus and infant, respectively. Table 1 lists the most commonly prescribed chronic CF therapies during pregnancy and lactation. Communication of the risks and benefits of using a drug during pregnancy and lactation must incorporate recommendations based on the pregnancy and lactation labelling rule established in 2015 (which eliminated previously utilised pregnancy letter categories A, B, C, D and X). With this ruling, informed discussion between clinicians and patients is required to properly consider 1) the impact of the maternal risk of continuing therapies versus no therapy with 2) the fetal risk of uncontrolled maternal disease and 3) the known and unknown risks of therapy on the neonate [31]. Because pregnant women are almost always excluded from clinical trials of new therapies, much of the data currently used for these discussions is based mostly on animal reproduction models rather than human data; future trials must address this issue as more women with chronic disease pursue pregnancy.
Maintenance CF therapies used during pregnancy and lactation
A mainstay of chronic treatment for people with CF is airway clearance applied to improve the impaired ciliary clearance that is pathognomonic with the condition. The two most common pharmacological agents that have been proven to improve mucus clearance are dornase alfa and inhaled hypertonic saline. Dornase alfa is a mucolytic and hypertonic saline osmotically thins mucus; both are typically used as chronic maintenance therapies. Recommendations for use of chronic CF therapies during pregnancy and lactation have been previously published, and both dornase alfa and hypertonic saline are believed to have little to no systemic absorption and thus cause little to no risk to fetal development. With little concern from pulmonologists or obstetricians, both agents are widely used throughout all trimesters of pregnancy and lactation in people with CF [11].
Inhaled antibiotics are also guideline-recommended and commonly prescribed maintenance therapies used to treat persistent airway infection in people with CF. Current recommendations suggest use of inhaled antibiotics for those people with moderate-to-severe lung dysfunction with a history of Pseudomonas aeruginosa infection [32]. Tobramycin, aztreonam, levofloxacin and colistimethate sodium are common anti-pseudomonal inhaled antibiotics used. While intravenous administration of tobramycin and colistimethate are not recommended for routine use during pregnancy, the inhaled route for all four agents is thought to have minimal systemic absorption and can be continued during pregnancy if needed to maintain clinical stability [11, 32].
The macrolide antibiotic, azithromycin, is another chronic oral maintenance therapy used in people with CF due to its immunomodulator effects, and data support azithromycin as having no risk to low risk to the fetus or infant, respectively [33]. While azithromycin is classified as “probably safe” to continue throughout pregnancy and lactation [11], widespread use is not as common. We showed that less than 50% of CF providers surveyed were extremely comfortable continuing azithromycin during pregnancy [34]. Lack of prospective studies on chronic azithromycin use in pregnancy in people with CF may explain this finding along with previous reports of a very low risk of an increase in congenital malformations with acute use. If azithromycin is discontinued, discussion regarding the potential low risk to the fetus in addition to the unknown risk to the mother is suggested.
Chronic therapies needed to maintain nutritional and digestive health in CF include fat-soluble vitamin supplements and pancreatic enzyme replacement therapies (PERT). Combined vitamin supplements composed of vitamins A, D, E and K are commonly prescribed. There are no data to suggest teratogenicity with these vitamins at usual repletion doses, but data do suggest that doses of >25 000 IU per day of vitamin A may be potentially teratogenic [11]. Folate supplementation is recommended as per usual pregnancy guidelines. PERT, composed of lipases, proteases and amylases, is compatible in pregnancy and lactation. Greater than 95% of CF clinicians were extremely comfortable continuing PERT throughout pregnancy when surveyed, and these therapies are widely used by pregnant people with CF worldwide [34].
CFTR modulators
With the US Food and Drug Administration (FDA) approval of ivacaftor (IVA) in 2012, lumacaftor/ivacaftor (LUM/IVA) in 2015, tezacaftor/ivacaftor (TEZ/IVA) in 2018, and elexacaftor/tezacaftor/ivacaftor (ETI) in 2019, CFTR modulator use is expected to continue to expand globally. With more widespread use of CFTR modulators, continued use during pregnancy and lactation has been a clinical and research topic of interest. Data from animal reproductive models have not shown fetal harm when individual modulator components are administered at normal human doses [35–38]. Numerous case reports of mothers with CF taking CFTR modulators have been published and summarised [1]. Infant complications attributed to CFTR modulators across the cases were minimal, but it is worth noting that one infant exposed to LUM/IVA in utero and during lactation had transient elevations in serum bilirubin and aspartate transaminase during lactation (but not at birth) without associated elevations in the mother. LUM/IVA drug levels were obtained in this case from maternal plasma, infant blood, and cord blood as well as breast milk. Researchers showed that LUM and IVA both crossed the placenta, and that LUM drug levels were higher in cord blood compared with maternal samples [1].
While data regarding CFTR modulator use in pregnancy were previously limited to animal models or case reports, emerging evidence from human studies has shown that CFTR modulator use throughout pregnancy and lactation has overall been well-tolerated. Nash et al. [4] conducted an international retrospective study of mothers with CF who used IVA, LUM/IVA or TEZ/IVA during pregnancy. Nine out of 61 women who discontinued CFTR modulators experienced a clinical decline with cessation of modulator therapies prompting re-initiation of therapy with subsequent improvement in clinical status. There were three first-trimester miscarriages reported in mothers on modulators, which translated to a lower rate than that in mothers of similar age without CF [4]. While there were two potential maternal complications rated as related to LUM/IVA by the treating clinician (one pulmonary exacerbation and one case of acute myelocytic leukaemia, a disease not known to be associated with LUM/IVA use), there were no complications in infants exposed to modulators in utero or during lactation that were deemed related to modulator use. With the more recent approval of ETI, continued use of ETI during pregnancy and lactation has also been evaluated. Taylor-Cousar and Jain [5] evaluated 45 pregnancies for which ETI was used for all or part of the pregnancy. Six mothers with CF discontinued ETI due to concern about the unknown risk to the fetus, with five of the mothers having to reinitiate therapy secondary to clinical deterioration. Miscarriage rates in this study were also comparable to that in the general population. Two potential maternal complications related to ETI use were reported. However, no infant complications were thought by treating clinicians to be definitely associated with maternal ETI use, and there were no infant complications in those who were exposed to breast milk from mothers using ETI [5]. As more women with CF have access to ETI globally and the adult population with CF continues to grow, additional data are needed to understand the maternal–fetal effects of ETI and to develop evidence-based recommendations for continued use during pregnancy and lactation. To address this need, R. Jain and J.L. Taylor-Cousar are leading a prospective, multicentre study, Maternal and Fetal Outcomes in the Era of Modulators (MAYFLOWERS), that is currently enrolling pregnant participants (ClinicalTrials.gov identifier: NCT04828382).
Pulmonary exacerbation treatment
Despite recent advances in therapies, pulmonary exacerbations, characterised by acute worsening of pulmonary symptoms and/or a decrease in lung function warranting antibiotic treatment, occur in people with CF and are associated with increased morbidity, decreased quality of life and ultimately, decreased survival [39]. As pregnancy rates in women with CF have increased over time, researchers have evaluated pulmonary exacerbations in pregnancy. While some retrospective data show no differences in pulmonary exacerbation rates between pregnant and non-pregnant women with CF, data from the Epidemiologic Study of CF demonstrated that pregnancy was associated with increased antibiotic use as well as increased outpatient and inpatient hospital visits which were likely multifactorial [40]. Furthermore, researchers have shown when stratified by disease severity, individuals with more severe disease require more days of intravenous antibiotics compared to those with mild disease [24]. Closer surveillance for pulmonary exacerbation treatment as well as for non-CF related obstetric complications could explain these finding, although it is unknown whether hormonal fluctuations or other physiological changes of pregnancy contributed.
General approaches for pulmonary exacerbation treatment in people with CF consists of optimising airway clearance as well as use of oral or i.v. antibiotics against the individual's current or most recently cultured respiratory pathogens. Although contemporary standardised guidelines do not exist for pulmonary exacerbation treatment, oral antibiotics are generally used for mild symptoms while i.v. antibiotics are used for moderate-to-severe symptoms and in those who are critically ill [39]. We showed that CF clinicians prefer to treat a mild pulmonary exacerbation with oral antibiotics and a severe pulmonary exacerbation with two i.v. antibiotics, which aligns with practice patterns in non-pregnant people with CF [34, 39]. Systemic antibiotic use in pregnancy is challenging due to placental transfer and risk for associated teratogenesis. See table 2 for considerations when prescribing the most commonly used antibiotics in pulmonary exacerbation treatment. Staphylococcus aureus and P. aeruginosa are the two most prevalent pathogens in people with CF, and antibiotic directed therapy against these two agents are commonly required [2, 8, 9]. Systemic antibiotics typically used in CF to target methicillin-susceptible S. aureus (MSSA) include the classes of penicillins and cephalosporins, both of which are compatible to use throughout pregnancy and lactation [11]. Treatment of methicillin-resistant S. aureus (MRSA) in non-pregnant people with CF includes trimethoprim/sulfamethoxazole, vancomycin or linezolid. While trimethoprim/sulfamethoxazole is a commonly prescribed oral option for non-pregnant patients with CF, this medication is avoided during pregnancy due to potential harmful effects of both components. Specifically, trimethoprim may impair folic acid metabolism and sulfonamide has been associated with fetal haemolytic anaemia and neonatal hyperbilirubinaemia and is contraindicated in pregnancy [11]. Thus, the two most widely used antimicrobials include i.v. vancomycin and oral and/or i.v. linezolid. Human studies of vancomycin have been limited in use during the first trimester, but no teratogenic effects have been associated with its use. Thus, vancomycin is considered “probably safe” during the first trimester and is compatible throughout the remainder of pregnancy and lactation [11]. Linezolid is another option to treat MRSA if allergies or intolerance prevent use of vancomycin. While animal reproductive models have not shown any teratogenic effects of linezolid use during pregnancy, there is a lack of human controlled studies and data have been limited to published and post-marketing case reports. Thus, use during pregnancy is suggested if the potential benefits outweigh the risks. Furthermore, linezolid is present in human breast milk, and while there are no data evaluating use of linezolid in lactation, data have shown that the two most commonly reported adverse events in infants receiving linezolid are diarrhoea and vomiting. It is recommended that if systemic linezolid is required during lactation, infants exposed are monitored for diarrhoea and vomiting throughout the duration of therapy [41, 42].
Common antibiotics used for treatment of a pulmonary exacerbation in people with CF
The standard approach for systemic treatment of P. aeruginosa in non-pregnant people with CF has been use of two antipseudomonal agents to increase intrapulmonary activity and minimise development of resistance of pathogens [39]. Fluoroquinolones including levofloxacin and ciprofloxacin, are commonly used oral antibiotics used to treat P. aeruginosa. Their use has been typically avoided in pregnancy given concern for cartilage damage in animal studies. However, recent studies have shown low risk of teratogenesis in human data and fluoroquinolones are considered “possibly safe” during pregnancy and lactation, and ciprofloxacin is the preferred agent to use if clinically indicated [11]. Aminoglycosides are typically used in conjunction with another antipseudomonal agent including β-lactams, cephalosporins and carbapenems. Aminoglycoside use throughout pregnancy is not recommended unless the mother has failed alternative therapies or is critically ill. β-lactams and cephalosporins are compatible throughout pregnancy and lactation and are widely used. However, there are limited data on the use of carbapenems during pregnancy. Case reports of meropenem are limited to the second and third trimester and suggest no increased risk. Thus, meropenem is considered “possibly safe” during the first trimester and “probably safe” during the remainder of pregnancy and lactation [11]. However, treating clinicians should be aware that women with CF have been shown to be more likely to develop severe pre-eclampsia, and carbapenems lower the seizure threshold [43]. The complexities of dual antipseudomonal treatment in pregnancy highlight whether monotherapy or dual therapy should be considered the standard of care. Prior studies addressing this question in non-pregnant people with CF have shown insufficient evidence to recommend one strategy over another [39]. Thus, monotherapy may be the appropriate strategy in pregnancy in someone with mild lung disease who is not critically ill, while dual therapy is reserved for those individuals with moderate-to-severe lung disease or who are critically ill. Continuous assessment will be needed with a low threshold to revise the strategy based on the mother's symptoms and response to treatment. Furthermore, use of inhaled antibiotics during pulmonary exacerbation management has not been evaluated in pregnancy and there has not been sufficient evidence to recommend for or against use in management in non-pregnant people with CF [39]. Inhaled antibiotic therapies during pregnancy may be another alternative given the minimal systemic absorption and minimal risk of inhaled therapies. Although use of highly effective CFTR modulator therapy has substantially reduced the occurrence of pulmonary exacerbations in people with CF, it has not eliminated them [6]. Therefore, future studies evaluating pulmonary exacerbation management during pregnancy in CF should be considered to help guide best practices for pulmonary exacerbation management during pregnancy.
Lactation
CF clinicians reported that over half of the individuals under their care with CF chose to breastfeed after delivery [34]. Lactation impacts both the mother and infant, and clinicians must routinely assess lactation status in the post-partum period. Lactation impacts the nutritional status of the mother, and generally an additional 500 kilocalories per day is recommended for lactating mothers in the non-CF population [44]. Caloric needs will be higher in people with CF who are lactating due to increased caloric expenditure associated with pancreatic insufficiency and CFRD [45]. Thus, careful assessment of the nutritional status and weight in the post-partum period are required in order to balance the benefit of lactation for the infant with potential accelerated weight loss of the mother. Weight loss in some people with CF has been rapid in the post-partum period resulting in return of pre-pregnancy weight within the first 6 weeks [3]. While this rapid weight loss does not occur for all people with CF, weight and BMI need to be monitored closely to optimise post-partum health. In addition, many medications commonly prescribed in CF are excreted in breast milk. Discussing the maternal and infant risks of continuing CF therapies that may be transmitted to the infant through breast milk, such as antimicrobials and CFTR modulators, is necessary. The majority of antibiotics are considered “probably safe” or compatible during lactation. Regarding CFTR modulators, data have shown that each individual modulator component is present in breast milk [35–38]. While no complications have been noted in infants exposed to CFTR modulators during lactation, animal models have demonstrated the occurrence of neonatal cataracts in juvenile rats exposed to IVA [4, 5]. Thus, it is recommended that infants exposed to IVA alone or in combination (LUM/IVA, TEZ/IVA or ETI) in utero or during breastfeeding receive ophthalmologic screening examinations for neonatal cataract evaluation. Furthermore, based on the known metabolism of CFTR modulators in the liver, reflexive or routine evaluation of infant liver function tests should be considered for infants exposed to modulators during breastfeeding.
Management of pregnancy in individuals with CF following organ transplantation
A small subset of those with CF are individuals who have undergone organ transplantation, most commonly bilateral lung transplant [2]. Most transplant centres counsel against post-transplant pregnancy because maternal and fetal complications associated with pregnancy after a lung transplantation are unfortunately high. This high rate of adverse outcomes was reported in a registry analysis in 2012 using data from the US National Transplantation Pregnancy Registry [46]. Investigators found that in 30 pregnancies (12 of whom had CF), the incidence of preterm birth was 60%, and there were 11 infant complications and two neonatal deaths [46]. There was a higher rate of rejection during pregnancy in those with CF (25% in CF versus 11% in those without CF), but there was a lower rate of spontaneous abortion in CF (25% in CF versus 33% in those without CF). Mean gestational age was similar in all groups, but mean birth weight was lower in CF (1980 g in CF versus 2349 g in those without CF). From a study using the Transplant Pregnancy Registry International, 7% of 51 post-transplant pregnancies resulted in graft loss within 2 years of pregnancy [47]. This immune phenomenon may occur spontaneously or due to providers and recipients decreasing immunosuppressive medications to protect the fetus, or rarely due to antibody-mediated rejection from human leukocyte antigen (HLA) sensitisation [48]. As noted above, many lung transplant centres request that recipients avoid pregnancy all together. Other centres recommend waiting at least 2 years after transplantation in order to safely achieve the lowest possible doses of immunosuppressive medicines prior to pregnancy, because immunosuppressive agents such as mycophenolate mofetil are not recommended during pregnancy due to potential fetal toxicity. Although successful pregnancies in transplant recipients may be possible, discussing reproductive goals and family-building options in the pre-transplant evaluation is warranted. Adoption and surrogacy may be alternative options if parenthood is desired in this population.
Conclusion
Pregnancy rates in people with CF are increasing as people are living longer and healthier lives, and we anticipate that these numbers will continue to increase with more widespread use of ETI and new therapeutic advances. With optimisation of preconception health and judicious use of chronic maintenance therapies and antibiotics for the treatment of acute pulmonary exacerbations, people with CF can have successful pregnancies with healthy infants. However, in the setting of markedly higher pregnancy rates in people with a wide range of baseline disease, prospective data collection to more clearly delineate risk factors for adverse maternal and fetal outcomes, including the use or withdrawal of modulators is needed. Generation of such data is crucial to aid clinicians in the provision of evidence-based recommendations to individuals with CF as they pursue all the avenues afforded by the likelihood of longevity.
Key points
More people with CF are becoming pregnant in the era of widespread CFTR modulator use.
Discussions surrounding pregnancy and parenthood in people with CF should occur early to allow for optimisation of preconception health.
Chronic maintenance therapies including inhaled mucolytics, pancreatic enzymes and fat-soluble vitamins are widely used throughout all trimesters of pregnancy and lactation in people with CF.
CFTR modulator use throughout pregnancy and lactation has generally been well-tolerated, but requires further study.
Self-evaluation questions
You are discussing preconception health with a 24-year-old woman with CF with a baseline FEV1 of 90% predicted (mild CF lung disease) and known pancreatic insufficiency on PERT. Her current BMI is 20 kg·m−2 and she asks what her BMI should be prior to conception. What is the current minimum recommended BMI that should be met for people with CF prior to conception?
a) 18 kg·m−2
b) 20 kg·m−2
c) 22 kg·m−2
d) 24 kg·m−2
A 30-year-old woman with CF with a baseline FEV1 of 69% predicted (moderate CF lung disease) is 2 weeks post-partum. She informs you that she has an increase in cough and sputum production and a drop in her FEV1 to 63% predicted. Her most recent sputum culture grew MRSA. In addition to reinforcing continued airway clearance with dornase alfa and hypertonic saline, you decided to start oral antibiotic therapy for treatment of a mild pulmonary exacerbation. She has an allergy to trimethoprim/sulfamethoxazole and is started on oral linezolid twice daily. She would like to continue breastfeeding during her treatment. It is recommended that if systemic linezolid is required during lactation, infants exposed be monitored for which of the following potential side-effects throughout the duration of therapy?
a) Skin rash
b) Diarrhoea and vomiting
c) Cough
d) Bruising
A 27-year-old woman with CF with a baseline FEV1 of 75% predicted (mild CF lung disease) presents to clinic for a routine follow-up. She has been on the CFTR modulator ETI for the past 18 months and is currently 15 weeks pregnant. She has continued on CFTR modulator therapy throughout pregnancy and plans to breastfeed after she delivers. She would like to continue her CFTR modulator throughout lactation and asks if there are any adverse events that should be monitored in the infant if she chooses to breastfeed. Based on prior data, which of the following recommendations would you suggest be carried out for infants exposed to CFTR modulators in utero and during breastfeeding? Please select all that apply.
a) Liver function tests
b) Complete blood count
c) Cataract evaluation
d) Immunoglobulin levels
A 32-year-old woman with CF with a baseline FEV1 of 55% predicted (moderate CF lung disease) is 24 weeks pregnant and is reporting dyspnoea, increased cough, sputum production and decreased oral intake. Her home spirometer shows an FEV1 of 35% predicted. She presents to the emergency department for evaluation. Her vital signs are notable for an oral temperature of 37.5 °C and respiratory rate of 22 breaths per min; her blood pressure is 110/70 mmHg and her pulse oximetry on room air is 85% and requires 4 L via nasal cannulae to maintain oxygen saturations >92%. She is on the CFTR modulator TEZ/IVA and is on pancreatic replacement for a history of pancreatic insufficiency. Her most recent sputum culture has grown P. aeruginosa. What is the next step in management?
a) Start an oral fluoroquinolone
b) Start intravenous aminoglycoside monotherapy
c) Start intravenous vancomycin
d) Start intravenous aminoglycoside and a beta-lactam
Suggested answers
c.
b.
a and c.
d.
Footnotes
Conflict of interest: K. Montemayor receives grant support from the Cystic Fibrosis Foundation (MONTEMQ020).
Conflict of interest: E. Tullis has received grants to her institution from Vertex Pharmaceuticals Incorporated, AbbVie, Corbus Pharmaceuticals, Inc, Celtaxsys, Spyryx and Bayer; has received fees from Vertex Pharmaceuticals Incorporated and Proteostasis for consultation on clinical research design, participation on advisory boards, and speaking engagements; all unrelated to this work.
Conflict of interest: R. Jain receives grant support from the Cystic Fibrosis Foundation (JAIN19Y3, JAIN21Y3). R. Jain receives grants to her institution from Vertex Pharmaceutical, Sound Pharma, Armata, Genentech, and Insmed and fees for consulting from Gilead and Boehringer Ingelheim.
Conflict of interest: J.L. Taylor-Cousar has received grants from the CF Foundation related to this work as well as for work unrelated to the manuscript. Unrelated to this work, she has received grants to her institution from Vertex Pharmaceuticals Incorporated, Gilead, N30, Celtaxsys, Proteostasis, and Bayer; has received fees from Vertex Pharmaceuticals Incorporated related to consultation on clinical research design, participation on advisory boards, and speaking engagements; has received speaking fees from Celtaxsys; and has served on advisory boards and/or provided clinical trial design consultation for Novartis, Genentech, Gilead, Protalix, Santhera, 4DMT, AbbVie and Proteostasis. She serves on a DMC for AbbVie. She serves as an advisor to the CFF Board of Trustees, and on the CF Foundation's Clinical Research Executive Committee, Clinical Research Advisory Board, and as chair of the CF TDN's Women's Health Research-Working Group, on the scientific advisory board for Emily's Entourage, and on the ATS Respiratory Health Awards Working Group and on the Scientific Grant Review and Clinical Problems Assembly Programming Committees.
- Received January 11, 2022.
- Accepted March 22, 2022.
- Copyright ©ERS 2022
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










