





Abstract
Parasomnias have significant quality-of-life, prognostic and potentially forensic implications for patients and their bed-partners. Identifying key clinical features will accelerate diagnosis and appropriate management for these patients. Parasomnias are undesirable physical events or experiences that arise out of, or during, sleep. They can include movements, behaviours, emotions, perceptions, dreams or autonomic nervous system activity. While more common during childhood, they can persist into, or present de novo, during adulthood. Parasomnias can arise out of non-rapid eye movement (NREM) sleep, as in confusional arousals, sleepwalking, sleep terrors or sleep-related eating disorder, or out of REM sleep, as in REM behaviour disorder, recurrent isolated sleep paralysis or nightmare disorder. Sleep-related hypermotor epilepsy is an important differential diagnosis to consider in patients presenting with a parasomnia. A thorough clinical history, including a collateral history if available, is crucial to identify characteristic clinical features. Video polysomnography is useful to identify macro- and micro-sleep architectural features, characteristic behavioural events, and any concomitant sleep pathologies. Treatment of parasomnias involves a combined approach of pharmacological and non-pharmacological intervention, including safety measures, sleep hygiene and medicines such as clonazepam or melatonin to improve sleep consolidation and reduce behavioural activity. As parasomnias can not only be disruptive for the patient and their bed-partner but have important prognostic or forensic consequences, an understanding of their pathophysiology, clinical features and management is valuable for any respiratory physician who may encounter them.
Educational aims
To understand the common features of NREM and REM parasomnias.
To differentiate between the causes of motor behaviours during sleep.
To discuss the treatment approach for NREM and REM parasomnias.
Abstract
Parasomnias have significant quality-of-life, prognostic and potentially forensic implications for patients and their bed-partners. Identifying key clinical features will accelerate diagnosis and appropriate management for these patients. https://bit.ly/3no6rhp
Introduction
Parasomnias are undesirable physical events or experiences that occur during entry into sleep, within sleep, or during arousal from sleep [1]. They encompass abnormal sleep-related movements, behaviours, emotions, perceptions, dreams, and autonomic nervous system activity. Historical depictions of parasomnias in film and literature are characterised by a general sense of mystery and complex psychology. Lady Macbeth manifested her suppressed fears into mobility and soliloquy; Lucy Westenra in Bram Stoker's Dracula sleepwalks and finds herself vulnerable to external dangers; Cesare, the somnambulist in the 1920 film The Cabinet of Dr Caligari, commits murder while asleep and under someone else's control, echoing some of the legal and forensic discussions concerning parasomnias today.
Parasomnias are more common in children but can present at any age. Broadly, parasomnias can be divided into behaviours associated with non-rapid eye movement (NREM) or rapid eye movement (REM) sleep. NREM parasomnias arise primarily (but not exclusively) out of slow wave, or stage N3, sleep, and include disorders of arousal (DOAs) such as confusional arousals, sleepwalking and sleep terrors. REM behaviour disorder (RBD) is the archetypal REM parasomnia, but this category also includes recurrent isolated sleep paralysis and nightmare disorder (table 1). NREM and REM parasomnias can coexist in parasomnia overlap disorder (POD) and may be confounded by other sleep disorders such as obstructive sleep apnoea (OSA). “Normal” parasomnias are benign but can nonetheless be distressing for patients and their bedpartners; these include hypnic jerks (or “sleep starts”) and their likely sensory variant exploding head syndrome, sleep paralysis, isolated hypnagogic or hypnopompic hallucinations and sleep talking. Abnormal events, as we will outline in this review, may represent rather more significant disease, and require further investigation. Thus, a basic understanding of parasomnias, their underlying pathophysiology and treatment options is valuable to any physician who encounters sleep disorders. The aim of this review is to provide an up-to-date summary of adult NREM and REM parasomnias for the respiratory physician.
International Classification of Sleep Disorders, third edition (ICSD-3) classification of parasomnias
Pathophysiology
NREM parasomnias
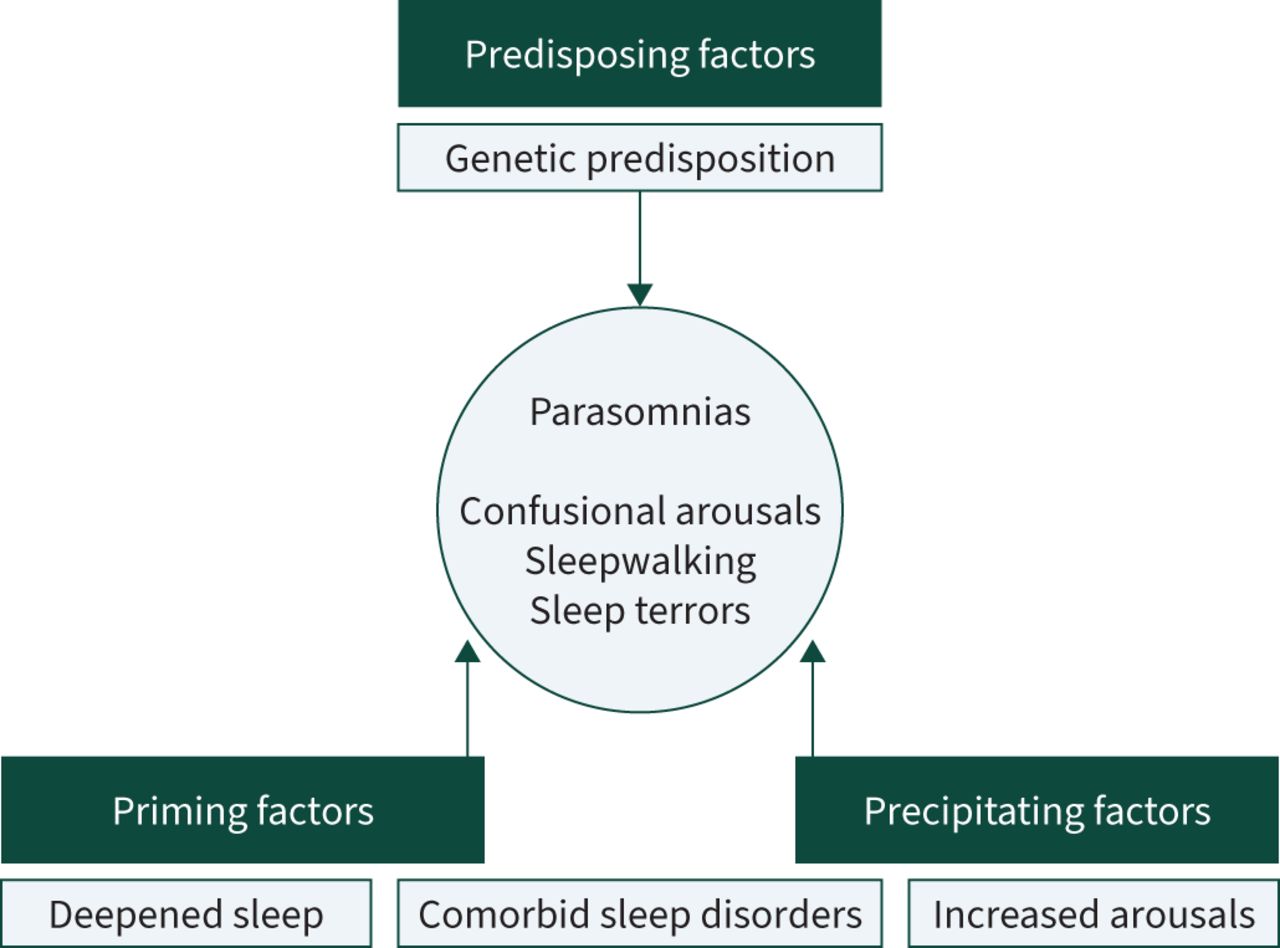
NREM parasomnias are understood to be the result of a combination of predisposing, priming and precipitating factors (figure 1). The threshold for parasomnias can be initially lowered by genetic susceptibility. Sleepwalking in a first degree relative increases the risk of sleepwalking by tenfold [2]. More recent evidence has found that NREM parasomnias, irrespective of type, are associated with the human leukocyte antigen (HLA) DQB1 genotype, found in up to 41% of a mixed group with DOAs [3], although it has also been found in up to 13% of normal individuals [4]. However, the sensitivity and specificity for HLA testing in NREM parasomnias are low, and the clinical implications of HLA positivity are poorly understood. Nonetheless, a strong family history of NREM parasomnias does indirectly provide evidence for an increased risk of NREM parasomnias.
{kind=link}
A pathophysiological model of disorders of arousal.
A genetic susceptibility is generally not enough to trigger a parasomnia, and individuals often need to be “primed” by factors that: 1) deepen slow wave sleep, increasing arousal threshold; 2) fragment sleep, increasing the likelihood of an arousal; or 3) more likely both, thereby introducing a sleep-state dissociation causing behaviour with a lack of awareness. This is evidenced by single-photon computed tomography (CT) and stereo-electroencephalogram (EEG) case reports demonstrating wakefulness and sleep in different parts of the brain during parasomnia activity [5]. Examples of priming factors would include any “background” influence on sleep, such as sleep schedule disruption, pre-existing medical or sleep disorders such as OSA, or substances like alcohol or drugs. Sedative and hypnotic drugs are particularly associated with parasomnias, with evidence for higher rates of sleepwalking in benzodiazepines and/or Z-drugs, in particular zolpidem [6, 7]. Other medicines associated with NREM parasomnias include antidepressants [8], β-blockers [9] and lithium [10].
Finally, a precipitating factor can provide a “tipping point” to a parasomnia, with a final stimulus destabilising slow wave sleep and triggering a partial arousal manifesting as parasomnia activity. This stimulus could be external, such as noise/light intrusion or the disturbance of a bed partner, or internal, such as a distended bladder. There is overlap in the existing literature as to whether comorbid sleep disorders, such as OSA or periodic limb movements during sleep (PLMS), are precipitating or priming factors, but what is clear is that their effect on sleep fragmentation can both increase sleep urge and trigger arousals, increasing the risk of parasomnias [5, 11].
REM parasomnias
RBD can be classified as primary (isolated) or secondary. Isolated (previously often referred to as idiopathic) RBD frequently represents a heralding symptom, lasting potentially years as a prodromal state for a neurodegenerative diagnosis with α-synuclein neuropathology, such as Parkinson's disease, dementia with Lewy bodies and multisystem atrophy. Boeve et al. [12] found synucleinopathies in 93% of a group of 172 patients with RBD, 87 of whom had started with isolated RBD. A more recent multicentre trial in 2019 with 1280 patients diagnosed with isolated RBD found a conversion rate to a neurodegenerative syndrome of 6.3% a year, and 73.5% at 12 years [13]. Other secondary causes of RBD include immune-mediated disease (narcolepsy, or as part of a more widespread disruption of sleep architecture as seen in anti-voltage-gated potassium channel limbic encephalitis), focal brainstem lesions (e.g. stroke or multiple sclerosis), alcohol or drugs (most commonly antidepressants or drugs with serotonergic or anticholinergic effects), and trauma [14].
During normal sleep, motor activity is suppressed during REM sleep by activation of the locus subcoeruleus in the pons, stimulating the medulla to block spinal lower motor neurons by hyperpolarising them via the inhibitory neurotransmitters glycine and γ-aminobutyric acid (GABA). Consequently, while the exact nature of the lesion in isolated RBD is unclear, dysfunction in the locus subcoeruleus and this pontine–medullary pathway is likely the cause of the loss of REM atonia and precipitation of dream enactment during REM sleep [14].
Clinical phenotypes
NREM parasomnias
NREM parasomnias are common in childhood, but most are self-limiting and spontaneously resolve as the nervous system matures into adulthood [15, 16]. However, NREM parasomnias can persist or present de novo in adulthood, although the reasons for this variable onset are poorly understood. Prevalence rates are limited by reporting bias, as studies in the general population rely on questionnaire data that are open to misinterpretation by respondents, as well as possible lack of awareness in the absence of a bed partner.
NREM parasomnias are mostly categorised as DOAs, whereby behaviours are observed after a partial arousal primarily from slow wave sleep, due to a combination of factors that provoke repeated arousal (table 2) [1]. These are characterised by absent or inappropriate responsiveness, limited or no cognition or dream reporting, and partial or complete amnesia for the episode [17]. DOAs traditionally include confusional arousals, sleepwalking and sleep terrors. Sleep-related eating disorder (SRED) and sexsomnia are currently also classified by the International Classification of Sleep Disorders, third edition (ICSD-3) as NREM parasomnias. NREM parasomnias frequently (but not always) occur during the first half of the sleep period when NREM sleep predominates, primarily arising from N3 sleep (80%) compared with N2 sleep (20%), and tend not to occur repeatedly during the same night, in contrast to sleep-related epilepsy [18].
ICSD-3 criteria for NREM parasomnias
Confusional arousals
The estimated prevalence of confusional arousals is 17% in childhood and 6.9% in adulthood [19]. They are characterised by disoriented behaviour following an arousal from sleep [1] and are the most common parasomnia events captured on polysomnography (PSG), regardless of the presenting phenotype [20]. Episodes often last less than a minute but can be prolonged, particularly in the setting of sedative or hypnotic medications. The confused behaviour is generally confined to the bed, for example sitting up and pulling at bedclothes, but without sleepwalking or the prominent fear associated with sleep terrors. Behaviour is usually benign but can occasionally be violent.
Sexsomnia is considered a subtype of confusional arousal, as behaviour is typically confined to the bed and associated with amnesia of the event, and patients will almost always have a history of DOA during childhood [1, 21]. Most events are triggered by a bedpartner's movement. Rarely, sexual behaviour can arise from REM sleep [22] or may have to be differentiated from sexual epileptic seizures [23]. Behaviour can range from masturbatory activity to attempted intercourse during sleep without awareness of the event, which can have major interpersonal relationship or forensic consequences.
Sleepwalking
Sleepwalking prevalence estimates are 14.5% in childhood and up to 4% in adulthood [19, 24]. Sleepwalking is characterised by ambulation outside of the bed, which in extreme cases can result in leaving the house, or even in complex behaviours such as driving long distances. Events can last anywhere from 1 to 20 min [1], and waking the patient during an event can rarely lead to an inappropriate or violent response, so it is generally preferable to gently guide the sleepwalker back to their bed [24].
Sleep terrors
Sleep terrors prevalence estimates are as high as 39.8% in childhood and 10.4% in adulthood [19]. Also known as night terrors or pavor nocturnus, these events are characterised by intense fear sometimes accompanied by a loud and piercing scream and a sympathetic nervous system response, including tachycardia, tachypnoea, flushing and mydriasis [1]. Adults can jump out of bed in response to a perceived threatening image or dream visualisation. In extreme situations, this has the potential to cause serious injury, in the event of falling out of bed or even jumping out of a window. Events typically last anywhere from 5 to 20 min and attempts to abort the event by waking the patient up can again lead to increased confusion and agitation.
Sleep-related eating disorder
SRED is rarely seen in clinical practice and was identified in <2% of 512 patients attending a specialist sleep clinic with NREM parasomnias [20]. This NREM parasomnia is characterised by episodes of eating after arousal from sleep with limited awareness but often a sense of involuntary or compulsive eating, followed by post-event amnesia [1]. This contrasts with night eating syndrome (NES), during which patients will eat >50% of their daily caloric intake at night, but with full awareness of their eating. However, NES and SRED may often coexist. Patients with SRED often eat atypical foods, such as uncooked pasta, and are alerted to their behaviour by finding the detritus of their eating as evidence of their parasomnia activity. Patients may experience complications of abdominal pain, weight gain or rarely poisoning from eating inedible substances. SRED is associated with restless legs syndrome (RLS), and treatment with sedatives or hypnotics can worsen amnestic SRED [25].
REM parasomnias
REM behaviour disorder
RBD is characterised by a loss of muscle atonia during REM sleep, accompanied by dream enactment behaviour (table 3) [1]. Patients are commonly male and older at presentation. Behaviour during REM sleep can range from relatively mild activity (e.g. limb jerking, singing, laughing, shouting, or calling out) to more violent activity (e.g. hitting or kicking out, running in bed, or falling out of bed). In contrast to NREM parasomnias, behaviour tends to be less complex, and patients are unlikely to get out of bed or sleepwalk. Motor activity tends to occur more during the latter half of the sleep period when REM sleep predominates, again in contrast to NREM parasomnias which tend to occur in the first half of the sleep period [26]. Behaviour is strongly linked to relevant narrative dream mentation, with dreams often acquiring a violent or confrontational theme, and patients report needing to protect themselves or their loved ones [26]. RBD in younger patients is less male-dominant, with less violent dream content and enactment. It is often associated with antidepressant use or can be a presentation of narcolepsy. These patients may be less likely to develop sinister neuropathology than their older counterparts, although this requires further study [27].
ICSD-3 criteria for RBD
Dream enactment behaviour can present a safety risk for patients and their bed partners, and a discussion about implementing safety measures in and around the bed is an important part of the management of RBD [28]. Comorbid sleep disorders may again be found, such as in POD where features of NREM parasomnias such as sleepwalking or sleep terrors are seen along with RBD [1]. Interestingly, RBD may have a protective effect on comorbid OSA, as the loss of REM atonia may blunt the upper airway collapsibility usually seen during REM sleep [29].
Recurrent isolated sleep paralysis
Recurrent isolated sleep paralysis is the inability to perform voluntary movements at sleep onset (hypnagogic) or on waking from sleep (hypnopompic) in the absence of a diagnosis of narcolepsy [1]. REM-related muscle atonia intrudes into wakefulness and patients are unable to speak or make any voluntary movements, although basic functions like breathing are unaffected. The events typically last seconds to minutes and can be aborted by stimulation such as being touched, or the patient making an intense effort to move. They are often accompanied by feelings of fear or anxiety, as well as auditory, visual or tactile hallucinations in 25–75% of cases.
Nightmare disorder
Nightmare disorder is characterised by the repeated occurrence of nightmares that cause clinically significant distress and are not attributable to another mental disorder or substance or alcohol use [1]. Nightmares arise out of REM sleep and often lead to an arousal where the patient is fully alert with a vivid recollection of their dream, in contrast to confusional arousals or sleep terrors, where the arousal is partial [30]. This also differentiates nightmare disorder from RBD, where patients experience vivid dreams associated with dream enactment behaviour but without arousals from sleep. Nightmares can be idiopathic or related to post-traumatic stress disorder (PTSD), where the nightmare content will either figuratively or thematically often reflect the inciting trauma. Nightmare disorder is largely a result of hyperarousal accumulated during the day and maintained at night, as seen in PTSD and insomnia, combined with impaired fear extinction, where fear memories are continually reinforced. These two factors contribute to a nightmare script, seen as a maladaptive response to traumatic experiences, childhood adversity, organic sleep fragmentation such as OSA or PLMS, or other cognitive or psychiatric conditions such as anxiety disorders [31].
Sleep-related hypermotor epilepsy
Sleep-related hypermotor epilepsy (SHE), previously known as nocturnal frontal lobe epilepsy (NFLE), is a rare form of focal epilepsy characterised by abrupt sleep-related seizures with various motor manifestations [32]. Seizures occur predominantly during sleep (although not always), primarily during NREM sleep and rarely during REM. Seizures can occur multiple times a night almost every night, with clustering a characteristic feature; this contrasts with NREM parasomnias, which tend to only occur once a night, if at all. Additionally, events arising within the first 30 min of sleep onset are unusual in NREM parasomnias, in contrast to the focal seizures of SHE. Seizures are brief, often <2 min, with a highly stereotyped motor pattern within individuals that can include emotive expression, tonic posturing, and hyperkinetic behaviours (e.g. kicking or cycling of limbs, or rocking body movements). SHE is discussed here as an important differential diagnosis for non-epileptic parasomnias, and while a video PSG (vPSG) is the “gold-standard” diagnostic tool, SHE can be identified with a few unique clinical features (table 4). Video recordings are often crucial in making the diagnosis of SHE, since the EEG, even during events, is frequently normal or obscured by movement artefact.
Different features of parasomnias, including DOAs, SHE, idiopathic RBD and nightmares
Assessment
The diagnosis of parasomnias is primarily clinical, and in the case of NREM parasomnias, the diagnosis can safely be made with a careful clinical history alone in 95% of typically presenting cases [1, 34]. Hence, a collateral history from the patient's bed partner is essential (where available), due to the limited recall that patients have of their behaviour during sleep; in RBD, this can be low as 35–44% [35, 36]. As parasomnias will vary in age of onset, duration, frequency, and intensity, as much of this information as possible should be obtained from the interview to guide the diagnosis, prognosis and treatment plan. An effort should be made to identify priming and precipitating factors, and so patients should be asked detailed questions regarding their sleep hygiene, sleep routines, and for any symptoms of comorbid sleep disorders such as OSA. With the ubiquity of smartphones, home video recording by bedpartners or family members can add valuable information, especially in capturing evidence of infrequent activity that may not be seen during one night of PSG [37] or in trying to differentiate parasomnia activity from seizure activity [38].
Video PSG
While NREM parasomnias are often a clinical diagnosis, video PSG (vPSG) can be helpful, particularly in atypical, injurious or violent cases, where the differential may include RBD, SHE, other sleep disorders or, rarely, functional neurological disorder or malingering [36–38]. Unfortunately, only 60–70% of vPSGs in patients with NREM parasomnias demonstrate diagnostic features, with half of those studies identifying abrupt arousals from slow wave sleep and sympathetic activation. Complex behaviours typical of NREM parasomnias are only demonstrated in 30–35% of vPSGs [39, 40]. However, vPSG can additionally provide valuable information about sleep quality and comorbid sleep disorders, such as OSA or PLMS; our centre found additional fragmentary sleep pathologies in 28.9% of a cohort of 512 patients with NREM parasomnias or POD [40].
Macro-sleep architectural changes associated with NREM parasomnias are inconsistently reported in literature, with some evidence to support a higher amount of slow wave sleep [41]. A higher number of arousals from sleep is usually demonstrated when compared with controls, but not when compared to patients with other fragmentary sleep pathologies [41, 42].
However, micro-sleep EEG changes seen on PSG are more consistently representative of a NREM parasomnia disorder. The cyclic alternating pattern (CAP) is an EEG marker of sleep instability, as EEG activity alternates between A (phasic) intruding on B (background) rhythms, and indicates increased arousability. An increased CAP rate has been seen in patients with DOAs, with parasomnia events triggered during phase A of the CAP. However, as with arousals, while CAP rate is increased in patients with NREM parasomnias compared with controls, the rate is similar to that of patients with other fragmentary sleep pathologies [43]. Hypersynchronous delta-wave (HSD) activity is another EEG marker that has been found in patients with NREM parasomnias [15, 18]. HSD describes multiple high-amplitude delta waves occurring during slow wave sleep that immediately precede and can often follow arousals from slow wave sleep. Again, this marker is more frequent in patients with NREM parasomnias compared with controls but is not specific, and is also seen in patients with fragmentary sleep pathology without NREM parasomnias [42].
A combination of macro- and micro-sleep features, along with behavioural events, can significantly increase the diagnostic accuracy for NREM parasomnias. The Slow Wave Sleep Fragmentation Index (SWSFI) combines microarousals, longer awakenings, and HSD associated with muscle activity. In the presence of at least one NREM parasomnia event (e.g. confusional arousal), vPSG has an improved sensitivity of 95% and specificity of 82% for the diagnosis of NREM parasomnias [44]. Another vPSG finding with a relatively high sensitivity and specificity for NREM parasomnias is if the patient demonstrates at least two episodes of eye-opening during stage N3 sleep; however, this is also seen in patients with SHE, and so the other clinical features should be carefully considered in these cases [32, 45].
For REM parasomnias, vPSG is used in the diagnosis of RBD, which requires 1) a history of abnormal behaviour during presumed REM sleep and 2) a vPSG recording demonstrating REM without atonia (RWA) [1]. RWA is the cardinal feature of RBD on PSG, picked up on electromyographic (EMG) chin and/or limb leads and scored using American Academy of Sleep Medicine (AASM) scoring guidelines [46]. Given the potential prognostic implications of a diagnosis of RBD in older patients, there remains some debate about the most appropriate precise definition of RWA on vPSG. The AASM have recommended that flexor digitorum muscle EMG recording be added to the PSG montage for the diagnosis of RBD [1]. It is important to note that RWA is not always seen in association with dream enactment behaviour in patients with RBD [47], although isolated RWA, in the absence of frank dream enactment behaviour, is thought to be a weaker marker of future development of neurodegenerative disorders compared with established RBD [48].
Treatment
Parasomnias are managed with a combination of pharmacological and non-pharmacological intervention, as well as treating any underlying contributary pathology such as comorbid sleep disorders or psychiatric conditions.
Safety measures
Safety measures should be discussed for both NREM parasomnias and RBD, for example removing potentially dangerous items from the surrounding bedroom area, or locking windows, doors or medicine cabinets; this advice can be tailored to the patient's typical NREM or REM parasomnia behaviour. Partners or family members should also be advised against forcefully waking the patient, which could cause further agitation, and instead try to gently guide them back to bed safely [49]. In patients with potentially injurious parasomnias, this advice may include placing cushions between bed partners or asking bed partners to sleep separately. Patients with RBD can also place cushions next to the bed, lower the bed or lie the mattress on the floor altogether to avoid serious injury because of dream enactment.
NREM parasomnias
Sleep hygiene is an appropriate first line of treatment for patients presenting with NREM parasomnias. Patients should be advised to avoid sleep deprivation and counselled on the effects of caffeine, alcohol and late exercise on sleep quality, and should be signposted to accessible patient information regarding sleep hygiene. This may be sufficient treatment for some patients, as seen in 13% of 512 patients with undifferentiated NREM parasomnias [20].
Priming and precipitating factors for NREM parasomnias should be addressed if present. As up to a third of patients with NREM parasomnias display evidence of concomitant sleep pathology [20, 40], such as OSA or PLMS, treatment of underlying sleep disorders alone, in particular OSA, can lead to satisfactory control of parasomnias in almost 20% of cases [20]. A novel non-pharmacological therapy, termed cognitive behavioural therapy (CBT) for NREM parasomnias, aimed at education of patients around disease pathophysiology and managing treatment expectations, combining sleep hygiene, anxiety management and mindfulness has offered promising results in select cases with behaviourally and psychologically driven precipitating and priming factors [50]. There is some early retrospective evidence to suggest that a combined non-pharmacological approach with sleep hygiene, safety measures, CBT and treatment for OSA if needed can be successful in up to a third of patients with NREM parasomnias, and this may be the preferred approach during pregnancy and in children [20].
If there is a risk or history of injury due to parasomnias, pharmacotherapy clearly becomes a potential first-line option. Much of the evidence for pharmacotherapy in parasomnias is based on case studies, clinical experience, and small clinical trials [51]. Clonazepam has the widest evidence base as a first-line option for NREM parasomnias, successfully controlling parasomnias as a single agent in up to 86% of patients [52]. It is particularly valuable if the patient or bed-partner is at risk of injury as a result of the parasomnia behaviour and if the benefit outweighs the risks of night-time falling or worsening OSA. While sedative-hypnotics have been associated with prolonged parasomnia events, zopiclone has been shown to be successful in treating NREM parasomnias, particularly when associated with insomnia, as have antidepressants such as fluoxetine, citalopram and mirtazapine [20, 49, 51]. Melatonin has also emerged as a successful treatment option for patients with sleepwalking, a mixed NREM parasomnia phenotype or POD, and may be a reasonable first-line option for patients without potentially dangerous parasomnias due to its relatively clean safety and side-effect profile when compared with clonazepam [20].
REM parasomnias
Due to the different pathophysiology, pharmacotherapy is more clearly indicated for RBD than in NREM parasomnias, although again the evidence is based on clinical experience and relatively small clinical trials. Clonazepam remains a first-line agent and is recommended in the AASM clinical practice guidelines [53]. Clonazepam is effective in up to 80% of patients with RBD at low doses (0.5–2 mg), with tolerance and dose-escalation rarely reported in this group. With its sedative effects, it should be used cautiously in frail or elderly patients, or those with OSA and not on treatment. Melatonin is also recommended by the AASM, although the evidence is less strong than for clonazepam, but its favourable side-effect profile compared with clonazepam causes many clinicians to regard it favourably as initial therapy, particularly when considering any comorbid OSA or the polypharmacy often seen in older patients [53]. Melatonin in doses of 3–12 mg has been found to satisfactorily reduce dream enactment in up to 86% of patients with RBD [54]. Medication lists should also be reviewed for antidepressants, which have been found to likely trigger RBD (as opposed to causing it de novo) [55]. It is again important to manage any comorbid sleep pathologies, as treatment with positive airway pressure for concomitant OSA in RBD can reduce dream enactment activity, possibly by restricting patients’ freedom of movement [27]. Treatment of PLMS in RBD patients may be simultaneously effective for both PLMS and RBD, albeit not to the same degree of success as in NREM parasomnias [56].
Legal implications
In rare circumstances, the diagnosis of a parasomnia may have important forensic implications. Diagnoses of sexsomnias, sleepwalking or RBD have been utilised as a defence in several high-profile cases of physical or sexual assault, or even murder. For NREM parasomnias in particular, given the low sensitivity and specificity of vPSG findings, the diagnosis may sometimes rest heavily on the clinical history, which may be unreliable where the accused is the only historian. Furthermore, the variability in behaviour requiring executive functioning or not, sleep environment, or proximity to the victim in cases of forensic parasomnias make retrospectively establishing a parasomnia event difficult, particularly when considering alternative neuropsychiatric diagnoses such as sleep-related dissociation or fugue states [57]. An antecedent diagnosis of parasomnia is preferable, and patients who have a history of potentially injurious or violent parasomnias should be made aware that, while they are not legally culpable for behaviour performed while they are asleep (the so-called “sleepwalking defence”), they are legally culpable for the potentially negligent position they put themselves in when falling asleep; this would include being aware of their surroundings, bedpartners, or any potential triggers to their parasomnias such as medications [23]. The role of alcohol remains under debate, as the ICSD-3 essentially excludes it as a potential trigger for DOAs due to the direct effects of alcohol intoxication and lack of concrete evidence identifying alcohol as a trigger for DOAs. However, the effects of alcohol on sleep architecture have been well described and there is (largely retrospective) data reporting the effects of alcohol on sleep behaviours [58]. Any cases with a forensic implication should involve a clinician trained as an expert witness.
Conclusion
The recognition and diagnosis of a parasomnia has broad implications, which in some circumstances extend beyond the management of the condition. These disorders may have consequences beyond the bedroom and a good night's sleep; they raise potential issues surrounding patient and bed-partner safety, may have forensic repercussions, and may provide important prognostic information, particularly regarding the risk of neurodegeneration. In some cases, making a firm diagnosis, especially based upon the clinical history, is not without difficulties, due to the variability in presentation and wide differential diagnosis. Appropriate referral to a specialist sleep centre with appropriate polysomnographic facilities and a multidisciplinary team to identify the potentially complex sleep pathology at play should be considered, and patient and bed-partner safety should be prioritised.
Self-evaluation questions
Which of the following statement(s) regarding factors contributing to DOAs is/are true?
The HLA DQB1 genotype is found in the majority of patients with DOAs.
Z-drugs and other hypnotics are protective through sedation and reducing the risk of arousal from sleep.
Comorbid sleep disorders, such as OSA or PLMS, increase the risk of parasomnias by both increasing the sleep urge and increasing the frequency of arousals from sleep.
Predisposing, priming and precipitating factors are always identified for patients with parasomnias.
Which of the following clinical features suggests SHE rather than a NREM parasomnia?
Typically occurring during the first third of the night.
Episodes tend to decrease in frequency from childhood.
Complex motor behaviour with eyes open and limited awareness.
Occurring up to every night, multiple times a night.
Which of the following about the prognosis of RBD is true?
A diagnosis of isolated RBD in an older patient is very likely to be a heralding symptom of neurodegenerative pathology.
Episodes of RBD tend to self-resolve over time.
A vPSG finding of REM sleep without atonia in a younger patient is very likely to be a heralding symptom of neurodegenerative pathology.
Dream enactment is difficult to manage, with medications only achieving satisfactory treatment in a minority of patients.
Which of the following non-pharmacological intervention is not recommended in the treatment of NREM parasomnias?
Sleep hygiene, to improve sleep quality.
Always share a bed, to ensure a collateral history.
Safety measures, to prevent injuries.
Cognitive behavioural therapy.
Suggested answers
c.
d.
a.
b.
Footnotes
This article has been corrected according to the author correction published in the September 2022 issue of Breathe.
Conflict of interest statement: All authors were involved in reviewing and drafting of the manuscript. The authors declare that the manuscript was written in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
- Received April 22, 2022.
- Accepted June 26, 2022.
- Copyright ©ERS 2022
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










