





Abstract
The global burden of bronchiectasis in children and adolescents is being recognised increasingly. However, marked inequity exists between, and within, settings and countries for resources and standards of care afforded to children and adolescents with bronchiectasis compared with those with other chronic lung diseases. The European Respiratory Society (ERS) clinical practice guideline for the management of bronchiectasis in children and adolescents was published recently. Here we present an international consensus of quality standards of care for children and adolescents with bronchiectasis based upon this guideline.
The panel used a standardised approach that included a Delphi process with 201 respondents from the parents and patients’ survey, and 299 physicians (across 54 countries) who care for children and adolescents with bronchiectasis.
The seven quality standards of care statements developed by the panel address the current absence of quality standards for clinical care related to paediatric bronchiectasis. These internationally derived, clinician-, parent- and patient-informed, consensus-based quality standards statements can be used by parents and patients to access and advocate for quality care for their children and themselves, respectively. They can also be used by healthcare professionals to advocate for their patients, and by health services as a monitoring tool, to help optimise health outcomes.
Abstract
Child-BEAR-Net has developed internationally derived, clinician-, parent- and patient-informed, consensus-based quality standards of care statements that patients and parents can use to access and advocate for quality care https://bit.ly/3w0tweP
Educational aims
To inform health service providers/commissioners and healthcare professionals of the international consensus recommendations for quality standards of care in the management of children and adolescents aged ≤18 years with bronchiectasis unrelated to cystic fibrosis. This includes patients with the clinical syndrome of chronic wet or productive cough with recurrent exacerbations, and radiographic confirmation of bronchiectasis.
To inform adolescents and parents of children and adolescents with bronchiectasis of these internationally derived quality standards of care statements to help in discussions with healthcare teams and help facilitate access to appropriate care.
Introduction
There is increased recognition of the resurgence of bronchiectasis [1, 2], as well as its adverse impact upon global respiratory morbidity [2] and mortality [3]. Bronchiectasis is now more common than thought previously [1, 4], with an estimated 3 million people affected worldwide [5]. However, despite this large burden of disease, bronchiectasis is deemed one of the most neglected pulmonary disorders in clinical practice by the European Respiratory Society (ERS) [6]. It is associated with a high patient burden, and high patient needs and treatment costs [7–9]. Yet, bronchiectasis is relatively under-researched and under-serviced [10] with large unmet needs, especially in children and adolescents [7, 11].
To enhance evidence-based management of paediatric bronchiectasis, an ERS task force recently published a clinical practice guideline (CPG) [12]. The CPG aimed to assist health professionals to provide the best care management of children and adolescents with bronchiectasis. By doing so, it sought to achieve the following in children and adolescents with bronchiectasis: 1) optimise lung growth, 2) preserve lung function, 3) enhance quality of life (QoL), 4) minimise exacerbations, 5) prevent complications, and 6) possibly reverse radiographic airway dilatation seen in chest computed tomography (CT) scans [1, 12].
The CPG posed 14 questions leading to 26 recommendations, where each recommendation was guided by parents’ views and balanced the possible benefits and risks associated with each of the treatment approaches [12]. Of the 14 questions, seven were framed as “Population, Intervention, Comparison and Outcome” (PICO) questions and seven were narrative questions (NQs) [12]. To aid dissemination, with the ERS and the European Lung Foundation (ELF), we also produced a pocket version, a slide kit and lay summary. Additionally, we wrote an accompanying article in Breathe with case studies to highlight the appropriate management of paediatric bronchiectasis [13].
We now need ongoing activities to facilitate implementation of the CPG. This requires additional tools, and an initial step is the availability of a series of quality standards of care statements. Quality standards of care are “a set of statements which describe the level of care consumers can expect from a health service. They aim to protect the public from harm and improve the quality of care provided” [14]. While quality standards of care statements (based on the British Thoracic Society guideline) exist for adult patients with bronchiectasis [15], there were no such statements issued for paediatric bronchiectasis.
Having standards matters in healthcare [16], even though defining standards can be complex and achieving consensus may be difficult [17]. Currently, many countries (e.g. Australia and the UK [18, 19]) have a governmental body or commission to help the health system deliver quality care and to provide regular reports [14] in recognition of the importance of standards of care. In addition, specialised societies, such as the British Thoracic Society, have established a “Standards of Care” Committee.
Standards of care are likely to be even more important in neglected diseases where inequity can be frequent and substantial. Bronchiectasis is one such example [6], especially affecting children [11]. Marked inequity between, and within, countries and among chronic respiratory diseases exist, even in resource-rich countries [3, 10, 20]. The need for better health services and clinical research for improving the lives and outcomes of children and adolescents with bronchiectasis and the lives of their families was made abundantly clear in a recent international parent and patient survey of their clinical needs [7]. This was illustrated by some children with bronchiectasis being unable to access physiotherapy expertise and the poorer quality of care provided to children with bronchiectasis compared to those with cystic fibrosis.
To aid the future implementation of the CPG, we developed a quality standards of care document to accompany the ERS CPG [12]. Its development was one of the five objectives of the newly established ERS Clinical Research Collaboration for paediatric bronchiectasis (Child-BEAR-Net; Children's Bronchiectasis Education, Advocacy and Research Network [21]). In a recent article, we described and elaborated on the development and interpretation of these quality standards of care statements [22]. Here, we explain how each quality standard could be measured, describe its underlying rationale, and also provide a description of what it means for health service providers and healthcare professionals, as well as for children and adolescents with a diagnosis of bronchiectasis.
Development of the quality standards of care statements
Our methods are described in detail in the supplementary material (figure S1). Briefly, we formed a panel with a steering committee, where membership of both groups was based upon the Child-BEAR-Net's governance framework (www.improveBE.org). The Child-BEAR-Net committee has 24 members consisting of an ELF representative, parent advisory group member, specialists in paediatric respiratory medicine who are experts in managing children and adolescents with bronchiectasis, as well as paediatric experts in infectious disease, environmental health, allergy, radiology, physiotherapy, the Cochrane Airways Group coordinating editor (also a family medical practitioner), a respiratory physiologist, a statistician, and two global leaders in adult bronchiectasis. Both groups iteratively developed draft statements from the CPG recommendations [12] that were considered the most important and were also measurable. These draft statements were agreed upon and then presented using two surveys to: 1) the community of patients with bronchiectasis as a child and the parents of children and adolescents with bronchiectasis; and 2) healthcare professionals who care for children and/or adolescents with bronchiectasis. We defined consensus a priori as achieving at least 80% agreement with both the patients and parents and the healthcare professional surveys for each statement. A summary of the demographics of the respondents to the surveys are presented in figures S2a–b.
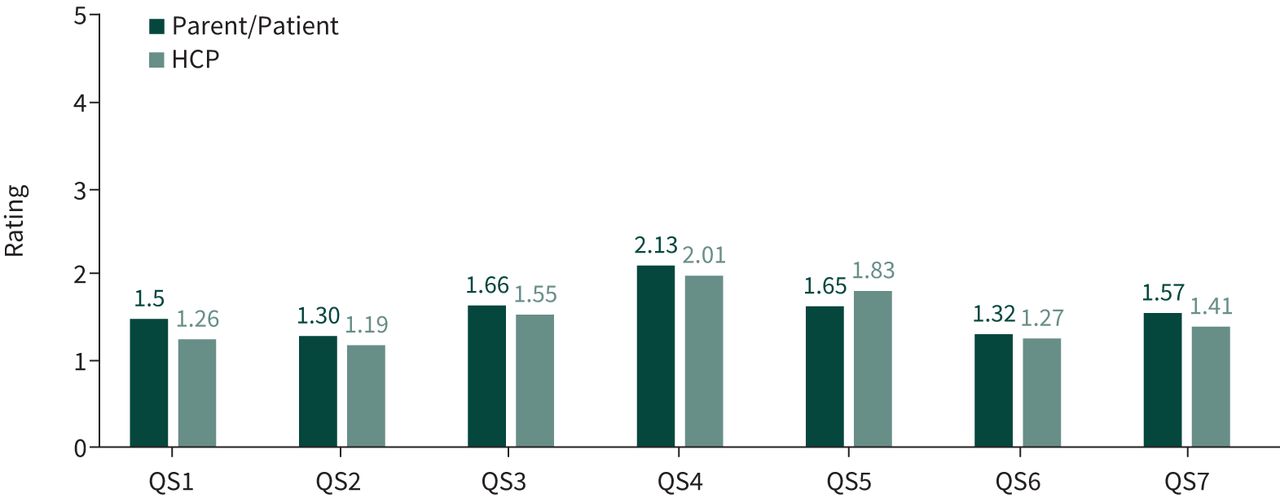
The weighted mean scores from both surveys are presented in figure 1 and the results summarised in the supplementary material. We achieved consensus on six statements and reworded one (statement 4) based on the free-text comments from survey responders and following further discussion within the steering committee. This statement was then amended to reflect more accurately the intended use of long-term macrolides as recommended in the CPG [12].

{kind=link}
Comparison of the weighted average for each of the quality standard (QS) of care statements from both surveys. Rating scale: 1 (strongly agree) to 5 (strongly disagree). HCP: healthcare professional.
The quality standards of care statements
A summary of the seven statements is presented in table 1, while table 2 presents the expanded version conveying additional information that includes quality measures, descriptions of what the quality statement means for various audiences and the rationale.
Summary of quality standard of care statements for clinically significant bronchiectasis in children and adolescents
Expanded quality standards of care statements
Statement 1: children and adolescents suspected of bronchiectasis have this confirmed by a chest CT scan
This statement was derived from PICO-1 in the CPG [12]. Chest CT scans are important for the accurate diagnosis of bronchiectasis, as there are other causes of a chronic (>4 weeks) wet or productive cough in children and adolescents. The chest CT scan also provides details on the extent of disease that may be used to guide clinical management. While CT scan data may not always be available (e.g. poor access to CT scanning facilities in resource-poor settings) and treatment should not be delayed, an accurate diagnostic method is seen as critical. Furthermore, the early diagnosis of bronchiectasis was one of the top priorities articulated by parents of children and adolescents with bronchiectasis or adults who had bronchiectasis diagnosed either during childhood or adolescence [7].
The CPG [12] recommended using child-specific criteria (rather than adult criteria). The key radiographic criterion for diagnosing bronchiectasis on chest CT scans is detecting abnormally dilated airways (determined by measuring the inner diameter of the bronchus to the adjacent artery diameter ratio (BAR)). The paediatric criterion for abnormality is a BAR >0.8. The BAR increases with age in otherwise healthy adults and increasing BAR is the main marker of severity in bronchiectasis radiographic scores [12]. Thus, diagnosing bronchiectasis earlier requires using an appropriate BAR diagnostic threshold to define abnormality. The CPG also suggested using multi-detector CT (MDCT) with high-resolution CT (HRCT) chest scans instead of HRCT scans alone as the former provides greater sensitivity. Using more sensitive diagnostic methods may be important for reimbursement issues in some countries, where the reimbursement of several treatment regimens for patients with bronchiectasis requires a radiographically confirmed diagnosis.
The above recommendations will lead to an earlier diagnosis of bronchiectasis and subsequent treatment, as many studies have described diagnosing bronchiectasis objectively resulted in a change in management (outlined in the supplement to the CPG [12]). However, there are no data comparing MDCT versus HRCT scans with clinical outcomes (e.g. change in management or QoL scores).
Requesting a chest CT scan for diagnosing bronchiectasis requires physician awareness. Thus, raising awareness amongst healthcare professionals and the general population of bronchiectasis in children and adolescents and the diagnostic role of chest CT scans is necessary. Also, strategies are needed to improve the availability and accessibility to high-quality scanners that reduce radiation exposure risk to patients, and also to healthcare professionals who can correctly interpret paediatric chest CT scans.
Statement 2: children and adolescents with bronchiectasis are taught appropriate airway clearance techniques by a respiratory physiotherapist
This statement was derived from PICO-4 in the CPG [12]. Airway clearance techniques (ACTs) are now standard therapies for children with any form of chronic suppurative lung disease. As there are many different types of ACT methods, age- and cognition-appropriate techniques targeted for individual children and adolescents are best taught and reviewed biannually by physiotherapists with expertise in paediatric respiratory care. Individual assessment also includes determining the frequency with which ACTs should be undertaken. Irrespective of the basal ACT frequency, children and adolescents should receive ACT more frequently during acute exacerbations of bronchiectasis.
While adverse events from ACTs are very minimal, ACTs can be time-consuming and adherence problematic. The burden of treatment may not be considered trivial from the patient and parent perspective, particularly in adolescence and/or when children are well for long periods of time.
Having access to physiotherapists with expertise in paediatric lung diseases and being taught the techniques and how to use the equipment at home were management priorities articulated by the parent advisory group and parents of children and adolescents with bronchiectasis or adults who had bronchiectasis diagnosed during either childhood or adolescence [7]. Health system resource requirements need to include access to physiotherapists with expertise in paediatric respiratory care to teach ACTs, monitor adherence and the ability to perform ACTs. In the modern era, digital technology and telehealth may facilitate online consultations and teaching when geographical distances are an issue, which will reduce costs. We also need strategies to improve acceptability and adherence to ACTs.
Statement 3: children and adolescents with bronchiectasis with an acute exacerbation are prescribed at least 14 days of antibiotics
This statement was derived from PICO-5 in the CPG [12]. Recurrent respiratory exacerbations (“flare-ups” or “attacks”) are common in people with bronchiectasis [23]. A respiratory exacerbation is considered present when a child or adolescent has increased respiratory symptoms (predominantly increased cough with or without increased sputum quantity and/or purulence) for >3 days [12]. Other less common respiratory symptoms and signs include haemoptysis, chest pain, breathlessness and wheeze, changes in chest auscultation findings and in chest radiographs (if these are indicated on clinical grounds). Systemic symptoms (fever, fatigue, malaise, a change in the child's behaviour or appetite) may also herald onset of an exacerbation but are nonspecific. Healthcare professionals should not rely upon these less common symptoms and signs being present.
Acute exacerbations have major negative health impacts upon people with bronchiectasis and are particularly important in children and adolescents as they are associated with increased respiratory symptoms, impaired QoL, accelerated lung function decline (decrease in forced expiratory volume in 1 s of −1.9% predicted per hospitalised exacerbation) and considerable healthcare costs [8, 24, 25]. Exacerbations are also associated with substantial healthcare utilisation. An Australian study reported high acute healthcare attendance and school/childcare absences (30 and 24.9 episodes per 100 person-months of observation, respectively) [26]. The ELF patient and parents’ survey showed that exacerbations were one of the top three factors that affected the child or adolescent's QoL [7].
There is a single high-quality study supporting antibiotics to treat exacerbations in which children who received oral amoxicillin-clavulanate were significantly more likely than those receiving placebo to have resolution of their exacerbation by day 14 of treatment [27]. However, there are no data for the duration of antibiotics required and so this quality standard is similar to that recommended in adult guidelines [28]. Although antibiotics are generally well tolerated, concerns remain over antimicrobial stewardship where frequent antibiotic consumption induces antibiotic resistance. Further research is needed to guide the duration of therapy so that these potential adverse effects (including antibiotic resistance) do not outweigh the benefits of treatment.
Children should be monitored for resolution of symptoms as some exacerbations may require more intensive treatment. The CPG [12] recommended that when the exacerbation is severe (e.g. the child or adolescent is hypoxic) and/or when the child or adolescent does not respond to oral antibiotics, intravenous antibiotics will be needed.
Timely treatment of exacerbations may be difficult in some settings where patients do not have easy access to healthcare facilities or to appropriate antibiotics. Health systems should ensure that patients have access to appropriate antibiotics for the recommended duration of treatment.
Statement 4: children and adolescents with bronchiectasis who have >1 hospitalised or ≥3 non-hospitalised exacerbations in the previous 12 months are offered at least a 6-month trial of macrolide antibiotics and their response assessed
This statement was derived from PICO-7 in the CPG [12]. Given the burden of exacerbations, and high-level evidence that using long-term macrolides (azithromycin) reduces acute respiratory exacerbations, the CPG recommended using macrolide antibiotics in selected patients [12]. Also, the desirable effects are large as preventing exacerbations is one of the goals of managing children with bronchiectasis. However, long-term macrolides are not recommended for all patients as there is a significant increase in macrolide-resistant bacteria in the upper airways of children receiving long-term azithromycin, compared with placebo [29]. Nevertheless, the clinical significance of macrolide-resistant pathogens colonising the upper airways is uncertain at an individual level. The longest duration randomised controlled trial using macrolides (∼24 months of azithromycin) [29] reported in their post hoc analyses that antibiotic use for non-pulmonary infections was significantly lower in the azithromycin group compared with placebo (incidence rate ratio 0.50, 95% CI 0.31–0.81; p=0.005).
Ensuring adherence of at least 70% is important for effectiveness in reducing acute respiratory exacerbations [29]. High adherence also reduces the risk of antibiotic resistance as adherence ≥70% (versus <70%) was associated with lower carriage of any pathogen (odds ratio (OR) 0.19, 95% CI 0.07–0.53) and fewer macrolide-resistant pathogens (OR 0.34, 95% CI 0.14–0.81) [30]. It is also important that children on long-term macrolides are reviewed for risk versus benefit.
Azithromycin should not be used in children or adolescents with contraindications to macrolides. This includes children and adolescents with an abnormal electrocardiogram, liver function abnormality and hypersensitivity to azithromycin. In those with a family history of prolonged QT syndrome, arrhythmias and acute cardiac events, an electrocardiogram should be obtained before commencing any macrolide therapy. In addition, a lower airway specimen should be obtained (when possible) to exclude nontuberculous mycobacteria before commencing long-term macrolide antibiotics.
Health systems need to ensure that macrolide antibiotics are available and patients have good access to them. Ideally, health systems should also provide the structure required for monitoring adherence.
Statement 5: children and adolescents with bronchiectasis have the minimum panel of diagnostic tests undertaken
This statement was derived from NQ-1 in the CPG [12]. As identifying an underlying cause of bronchiectasis will influence management, there is a large desirable effect of setting a standard set of investigations as a minimum panel. These are: 1) chest CT scan (to diagnose bronchiectasis), 2) sweat test, 3) lung function tests (in children and adolescents who can perform spirometry), 4) full blood count, 5) immunological tests (total IgG, IgA, IgM, IgE and specific antibodies to vaccine antigens) and 6) lower airway bacteriology. In settings where tuberculosis or HIV have a high prevalence and/or there is a history of close contact with tuberculosis, assessment for tuberculosis infection/disease or HIV, respectively, is also undertaken as part of the minimum panel of tests.
Although lung function and respiratory cultures do not identify the cause, they help assess severity and guide antibiotic choices, thus optimising treatment. Some children and adolescents require additional investigations (e.g. flexible bronchoscopy with bronchoalveolar lavage or tests for primary ciliary dyskinesia or aspiration) that are tailored to their clinical history, while other tests will also depend upon the different geographical distribution of causes of bronchiectasis, such as HIV infections and tuberculosis.
Health services should increase accessibility to centres practising standard of care management for children and adolescents with bronchiectasis that includes undertaking the recommended minimum panel of tests.
Statement 6: children and adolescents with bronchiectasis receive specialist paediatric respiratory physician care
Statement 7: children and adolescents with bronchiectasis are reviewed at least 6-monthly by a multidisciplinary team
Both the above statements were derived from a combination of NQs 3–5 in the CPG [12]. Current standard care in specialist respiratory clinic settings leads to improved lung function post-diagnosis, as documented in the supplement to the CPG [12].
In any chronic illness, disease monitoring is an important component of routine clinical care and this is best undertaken by a multidisciplinary team (MDT) with individualised and multidisciplinary case management operating within an inter-professional framework [31]. MDT care is defined as healthcare professionals from several disciplines working together to provide comprehensive and coordinated management to meet the needs of the individual patient [32, 33]. An MDT led by a clinician with expertise in chronic suppurative lung disease and bronchiectasis (i.e. a specialist paediatric respiratory physician) is recommended and was specifically highlighted by the parent advisory group. Other members of the MDT should include respiratory nurses and specialist paediatric physiotherapists, as well as easy access to dieticians, psychologists, pharmacists, and other medical specialists (e.g. infectious diseases, immunologists and radiologists with expertise in respiratory medicine).
Specialists in tertiary paediatric respiratory clinics currently use a model of care that, although not fully described, includes standardised care involving assessment of clinical stability and any deterioration in overall and respiratory health. In these settings, studies have shown that such a model leads to improved lung function post-diagnosis of bronchiectasis. The monitoring process in tertiary paediatric respiratory clinics consists of clinical symptoms, frequency and severity of respiratory exacerbations, and lung function indices. It also includes reviewing their general well-being, re-evaluation of their educational needs, vaccinations, psycho-social support, and performance of exercise and ACT requirements, including any equipment. It is also important to educate healthcare professionals, families and patients on the role of surveillance sputum cultures for informing future treatments, even in those with clinically stable bronchiectasis. Factors important for reversibility and/or prevention of bronchiectasis should be identified early. These include treatment of inhaled foreign bodies, preventing early and severe pneumonia, preventing recurrent protracted bacterial bronchitis, treating primary immunodeficiency disorders causing bronchiectasis, promoting breastfeeding, and avoiding tobacco smoke, vaping and other airborne pollutants.
When deterioration occurs, evidence supports assessing and investigating for treatable traits: new infection, asthma, nutritional deficiencies, dental or sleep disorders (as described in the supplement to the CPG [12]). Ideally, members of the MDT should be available at short notice for management of exacerbations.
Differential access (from living in rural regions or away from a major centre with all the necessary specialist expertise) is currently problematic for some patients with bronchiectasis. Health systems need to support the access of children and adolescents to centres practising standard of care.
Discussion
Using a Delphi process, we derived an international quality standards of care document that consists of seven statements that are based upon recommendations from the ERS paediatric bronchiectasis CPG [12]. The only quality standard document available for bronchiectasis, that we are aware of, is that of the British Thoracic Society [15], which was based on their 2010 guideline. The British Thoracic Society quality standards statement [15] has been used to assess and monitor the quality of care provided to adults with bronchiectasis in the UK [34] and in other countries [35]. A paediatric-specific document is necessary in the context of several major differences between children and adults with bronchiectasis [1, 2, 15, 36]. These include children and adolescents needing age-appropriate parental care, support and input. In addition, there are important differences in pathogen profiles (bacterial [36] and microbiota [37]), immunological responses [38], comorbidities, relative frequency of underlying aetiologies [2], diagnostic criteria in chest CT scans, and measurements and definitions of treatment outcomes [1]. Consequently, our quality standards of care statements are different to the British Thoracic Society document [15]. However, there are also similarities as the structure we used was guided by the British Thoracic Society quality standards [15], which was led by a steering committee member (A.T. Hill) in our panel.
Clinical guidelines that impact upon outcomes of care are required to be evidence-based and well-developed with wide dissemination and implementation. Improving healthcare is complex and requires many steps with coordinated action between healthcare professionals, health systems, other government and non-government agencies, and communities [39]. Implementing guidelines is also complex with a scientific body of work that is context specific [40]. The availability of quality standards of care statements is only one of the initial steps in this journey.
Conclusion
This document from the ERS Clinical Research Collaboration Child-BEAR-Net presents the first quality standards of care statements for children and adolescents with bronchiectasis. It used an international Delphi process, which included healthcare professionals, parents and patients with bronchiectasis. We believe that our international consensus quality standards of care statements for managing children and adolescents with bronchiectasis are an initial step in improving the overall quality of care they receive. To help address the current inequity, these statements can be used by: 1) parents and patients to access and advocate for quality care for their children and themselves; 2) healthcare professionals to advocate for their patients; and 3) health systems as a monitoring tool. The next step is for this tool to be used for quality improvement and to improve standards, as achieved by the cystic fibrosis quality improvement programme [41].
Key points
An ERS task force recently published a paediatric clinical practice guideline for the management of children and adolescents with bronchiectasis where 14 questions were posed leading to 26 recommendations.
The ERS Clinical Research Collaboration on paediatric bronchiectasis (Child-BEAR-Net) has now developed seven quality standards of care statements from this guideline that represent an international consensus by patients with bronchiectasis, parents of children with bronchiectasis and clinicians involved in their care.
Each quality standard of care is accompanied by explanations of how it can be measured, a description of what the quality standard means for health service providers/commissioners, healthcare professionals, and children and adolescents with bronchiectasis, as well as the rationale for each quality standard.
The quality standards of care can be used to support and monitor the implementation of the ERS paediatric bronchiectasis clinical practice guideline.
Self-evaluation questions
Regarding the quality standard of care statement for diagnosing bronchiectasis in children and adolescents, which one of the following is true?
The diagnosis of bronchiectasis only requires an abnormal chest radiograph.
A chest CT scan is needed to confirm the diagnosis of bronchiectasis.
The diagnosis of bronchiectasis warrants only a thorough history and examination.
The adult criterion of a broncho-arterial ratio >1–1.5 can be used to diagnose bronchiectasis in children and adolescents.
Regarding children and adolescents with bronchiectasis undergoing a set of tests, which one of the following is true?
Lower airway bacteriology and lung function tests (when age appropriate) are not part of the panel of tests undertaken in all patients.
Video-fluoroscopy, HIV serology, and interferon-γ release assays for tuberculosis are performed routinely in all adolescents.
The standard tests include full blood examination, immunological tests (total IgG, IgA, IgM, IgE, specific antibodies to vaccine antigens) and a sweat test.
When the diagnosis of bronchiectasis is straightforward and confirmed radiographically, additional tests are no longer necessary.
Regarding caring for children and adolescents with bronchiectasis, which one of the following is false?
All children and adolescents with bronchiectasis should undergo specialist clinical review at least 6-monthly.
A multidisciplinary team that includes specialist paediatric respiratory physicians is required to optimise care.
Receiving the standard of care in specialist settings improves lung function post-diagnosis of bronchiectasis.
Children and adolescents with bronchiectasis are best managed in primary care with specialist review only when necessary.
Regarding ACTs in children and adolescents with bronchiectasis, which one of the following is true?
ACTs should be taught by physiotherapists with expertise in paediatric respiratory care.
Once taught and mastered, ACTs can remain the same, irrespective of age and clinical state.
ACTs are not always necessary and do not need to be made available by health systems.
The frequency of ACTs is unaltered during an exacerbation, especially when it results in dyspnoea.
Regarding the quality standard of care statements for children and adolescents with bronchiectasis, which one of the following is false?
Children and adolescents are prescribed at least 14 days of antibiotics for treatment of an acute exacerbation.
Those with >1 hospitalised or ≥3 non-hospitalised exacerbations in the previous 12 months are offered at least a 6-month trial of macrolide antibiotics and the response assessed.
Health service providers/commissioners should ensure that access to specialist paediatric respiratory physician care is available.
Children and adolescents should receive their care and have their progress monitored solely in primary healthcare settings.
Suggested answers
1. b.
2. c.
3. d.
4. a.
5. d.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material EDU-0144-2022.SUPPLEMENT
Footnotes
Conflict of interest: E. Alexopoulou, A. Bush, C. Constant, K. Douros, R. Fortescue, M. Griese, A. Hector, B. Karadag, A.T. Hill, A. Kantar, O. Mazulov, F. Midulla, A. Moeller, M. Proesmans, S.T. Yerkovich, A. Zacharasiewicz, Z. Powell, C. Wilson and A.J. Collaro have nothing to disclose. J. Boyd is an employee of the European Lung Foundation. A.B. Chang reports grants from National Health and Medical Research Council, Australia, during the conduct of the study; monies provided to institution from IDMC Membership of unlicensed products (GSK, AstraZeneca), and vaccine (Moderna), other from Advisory member of study design for unlicensed molecules for chronic cough or bronchiectasis (Merck, Zambon, Boehringer Ingelheim); personal fees from being an author of two UpToDate chapters, outside the submitted work. J.D. Chalmers reports grants and personal fees from AstraZeneca, grants and personal fees from Boehringer Ingelheim, personal fees from Chiesi, grants and personal fees from GlaxoSmithKline, grants from Gilead Sciences, grants and personal fees from Insmed, personal fees from Novartis, personal fees from Zambon, outside the submitted work. J. Grigg reports grants and personal fees from OM Pharma, personal fees from GSK, personal fees from Novartis, personal fees from Omron, personal fees from Astra Zeneca, outside the submitted work. K. Grimwood reports grants from Australian National Health and Medical Research Council and the Australian Medical Research Future Fund during the conduct of the study.
- Received May 20, 2022.
- Accepted August 8, 2022.
- Copyright ©ERS 2022
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










