





Abstract
During the coronavirus disease 2019 (COVID-19) pandemic, sleep medicine services were dramatically reduced worldwide. Implementation of mitigation strategies was suggested by expert organisations and helped to restart sleep medicine services. Distance communication and monitoring during diagnosis, treatment initiation, and treatment follow-up have been used widely, in particular for patients with sleep apnoea. Follow-up studies demonstrate both advantages and potential disadvantages with the use of these new technologies.
Emerging epidemiological evidence suggests that obstructive sleep apnoea may be an independent risk factor for adverse outcome in COVID-19, including an increased risk for hospitalisation and elevated mortality. Experimental studies explaining the underlying mechanisms behind these findings are warranted.
Abstract
Sleep medicine services have made a transition from hospital- to patient-centred care by implementation of digital tools and new clinical pathways. These new pathways adopted during the COVID-19 pandemic need thorough validation. https://bit.ly/3axYPGw
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus has caused a worldwide pandemic. According to statistics published by the World Health Organization, by mid-May 2022 more than 520 million infections with SARS-CoV-2 had been verified and almost 6.3 million patients had died with or because of verified coronavirus disease 2019 (COVID-19) [1]. The global threat of this pandemic has affected sleep quality for many individuals during the past 2 years. Given that obstructive sleep apnoea (OSA) has an estimated prevalence of between 500 million and up to 1 billion people [2], a substantial number of patients with COVID-19 also had comorbid sleep apnoea. Indeed, risk factors for severe COVID-19 included well-known risk factors for sleep apnoea like older age, male sex, obesity, arterial hypertension, and diabetes mellitus [3]. Thereby, the potential causal link between sleep apnoea and COVID-19 has been discussed since the beginning of the pandemic.
Healthcare services all over the world adapted rapidly to the new pandemic situation and shifted personnel to care for patients with severe COVID-19 infections and multiorgan failure. This had large impact on other areas of medical care including sleep medicine services for sleep apnoea patients [4].
In this review several aspects of the impact of the COVID-19 pandemic on sleep medicine will be discussed. Those aspects include:
the relationship between SARS-CoV-2 infections and sleep disorders;
the risk for severe COVID-19 infection in patients with OSA;
the role of positive airway pressure (PAP) treatment during the pandemic;
the effects of the COVID-19 pandemic on sleep medicine practice;
mitigation strategies to overcome the lockdown of sleep medicine practice; and
the potential lessons learned from the pandemic for future care models in sleep medicine.
The relationship between SARS-CoV-2 infections and sleep disorders
Several questionnaire-based studies assessed the subjective sleep quality of different populations during the pandemic. According to a meta-analysis published early 2021, ∼32% of individuals in the general population reported disturbed sleep during the pandemic [5]. The number was higher in healthcare workers (36%) and patients affected by COVID-19 reported the highest rate of disturbed sleep (up to 75% of cases).
In a comprehensive review, Kumar and Gupta [6] described potential pathways for a causal relationship between sleep disorders and SARS-CoV-2 infection (figure 1). One proposed pathway goes directly through a central nervous system infection by the SARS-CoV-2 virus. It may affect the central nervous system at certain areas of interest for sleep–wake regulation. Other potential effects may be mediated through the influence of systemic inflammation and the cytokines expressed by the immune system in response to the virus infection. Severe lung injury, subsequent hypoxia and multiorgan failure may severely affect the entire body including the basic mechanisms for sleep–wake regulation. Nocturnal breathing pattern and coughing may further deteriorate sleep by causing frequent arousals. Beside the direct effect of the virus infection on sleep–wake regulating mechanisms, pandemic-induced stress may have deteriorated sleep–wake patterns. Several changes were reported including a decrease in sleep time and a modification of the external zeitgebers (e.g. a modified working schedule) as well as difficulties initiating and maintaining sleep. Worries about risk of infection, changes at work or the economic situation may have increased overall stress levels and induced both acute and chronic sleep disturbance [5, 6]. It has been speculated that chronic sleep disturbance may have compromised both the natural immune response to SARS-CoV-2 virus infections [6] as well as the response to vaccination against the coronavirus. However, these hypotheses have not been proven. In contrast, some individuals may have increased total sleep time and reduced their social jetlag during the pandemic [7].

Pathways which may explain an increased prevalence of sleep disorders during the COVID-19 pandemic.
The risk for severe COVID-19 infection in patients with OSA
Several pathomechanisms potentially promoting SARS-CoV-2 infection and increasing the risk for severe COVID-19 in OSA patients have been discussed [8]. For example, the angiotensin-converting enzyme 2 (ACE2) receptor binds the surface spike protein of SARS-CoV-2, which enables the virus to enter human cells [9]. As the renin–angiotensin system is upregulated in patients with OSA, a potential increased risk for COVID-19 infection has been postulated [10]. Further, systemic inflammation is elevated in OSA patients with significant intermittent hypoxia which may further contribute to inflammation and the cytokine storm identified in severe COVID-19. Other factors discussed are vitamin D deficiency and pulmonary fibrosis, both of which are observed in cases with severe COVID-19 and may be associated with an increased likelihood of OSA. The overlap of risk factors for severe COVID-19 and OSA, namely male sex, age, obesity and frequent cardiometabolic disease, raises the obvious question of whether OSA is only part of the comorbidity spectrum or if OSA is an independent risk factor for adverse outcomes in COVID-19.
Initially, data on the influence of OSA on COVID-19 outcomes were contradictory when confounders like obesity were added in the analysis models [8]. However, recent large studies and meta-analyses suggest that OSA is a mild-to-moderate risk factor for adverse outcomes in COVID-19, including increased rates of hospitalisation and need for intensive care, as well as mortality [3, 11–13]. One of the most comprehensive analyses, to date, on factors predicting adverse COVID-19 outcomes was published by Bellou et al. [3]. They identified 428 articles of interest and performed 283 meta-analyses looking at 91 unique prognostic factors for 11 different outcomes in patients with PCR-verified COVID-19 (including hospitalisation, intubation rate and mortality). OSA showed consistent evidence as a risk factor for hospitalisation, with an odds ratio of 2.1 in a dataset from five studies including 2475 events from 3819 individuals. One limitation is that the risk estimates could only be computed in univariate analysis. These data are further supported by the meta-analysis of Hu et al. [11] including data from 13 studies and 31 933 COVID-19 patients. The mean adjusted effect estimate (EE) for COVID-19-related mortality in OSA patients was 1.56 (95% CI 1.2–2.0) for the entire analysis population. The elevated risk was consistent in sensitivity analyses when analysing only hospitalised COVID-19 patients (EE 1.7 (95% CI 1.38–2.1)) or patients in the age strata <60 years (EE 1.43 (95% CI 1.1–1.9)) and ≥60 years (EE 1.8 (95% CI 1.3–2.5)). Although it is stated that these effect estimates are adjusted and independent, it is not further detailed which adjustment factors have been applied. Further limitations of the analysis include the lack of exact definitions for OSA diagnosis in the included studies (apnoea–hypopnoea index threshold or diagnosis retrieved from the medical records) and missing information about ongoing OSA treatment.
The use of PAP treatment during the COVID-19 pandemic
Is the use of PAP protective for severe COVID-19 infection in OSA patients? Two recent papers have addressed this question. A large Icelandic cohort of PCR-verified COVID-19 patients (n=4756) was linked with the clinical cohort of known OSA patients to identify OSA patients with COVID-19 (n=185) [12]. Severe COVID-19, defined as hospitalisation and/or death, was fivefold more common in OSA patients compared with the remaining Icelandic inhabitants (odds ratio 5.6), but after adjustment for confounders like age, sex, body mass index and comorbidities, the odds ratio was reduced to 2.0 (95% CI 1.1–3.6). In the subgroup of OSA patients with ongoing PAP treatment (n=90), the fully adjusted odds ratio for severe outcome was still elevated with 1.9 (95% CI 0.6–6.0), although no longer statistically significant. Another study from Spain identified 2059 patients hospitalised due to severe COVID-19, 81 of whom had known OSA treated with PAP at home prior to referral [13]. Outcome was defined as death and/or severe hypoxic respiratory failure at referral. Continuous positive airway pressure (CPAP) treated OSA patients did not show an increased risk for adverse outcome as defined in this study, indicating a potential protective influence of PAP treatment on the excessive OSA-related risk. However, the limited power of both studies and their retrospective design does not allow firm conclusions to be drawn on any potential beneficial effects of OSA treatment on the elevated risk for adverse COVID-19 outcome in OSA patients. Further large size studies are warranted to address the limitations in our current understanding of the role of OSA in COVID-19: is there a dose response between risk and OSA severity, and can OSA treatment reverse the elevated risk?
In 2020, there was debate as to whether the use of PAP devices and home ventilators may increase the risk of virus spread by exhalation through the masks used in PAP and home mechanical ventilation (HMV) devices, classified as aerosol generation. The experimental evidence was given, but only limited data were reported on the actual spread of virus in OSA patients. One recent study investigated 30 patients using PAP or nasal high flow (NHF) treatment in an intensive care unit [14]. Virus particles were studied in the air and on the surfaces around patients using PAP, NHF or supplemental oxygen. Interestingly, there was no sign of increase in virus particles in the immediate care area of the patients when compared with the data for regular respiratory activities. The findings were confirmed in a study of 25 healthy volunteers quantifying aerosol emissions during breathing, speaking, and coughing, as well as during PAP and NHF use [15]. These data suggest that regular breathing, speaking, or coughing are more aerosol generating than the use of PAP or NHF [16].
Did the COVID-19 pandemic alter the pattern of PAP use in sleep apnoea patients? This question has been examined in several small studies that suggest a partial increase in PAP adherence. A large French cohort study followed the weekly PAP usage pattern, via telemonitoring, in 8477 experienced CPAP users during 2019 and 2020 [17]. Mean CPAP adherence varied considerable throughout the year during the pre-pandemic observation period, with the lowest adherence during the hot summer in 2019 and the week following Christmas. During the first lockdown in France in 2020 mean adherence increased by ∼15 min but decreased sharply when the spread of SARS-CoV-2 decreased during the subsequent summer weeks. Median PAP adherence was 7.21 (6.12–8.10) h per day in 2020 and 7.12 (6.05–8.02) h per day in 2019 (p<0.001). The authors summarised that the pandemic was followed by a small, but clinically nonsignificant, rise in PAP adherence.
The effect of the COVID-19 pandemic on sleep medicine practice
Several studies and reviews have documented the profound changes to sleep medicine services during the COVID-19 pandemic [6, 18]. In the initial phase of the pandemic, health services were directed towards the acute care of severely ill COVID-19 patients. Elective care of patients with sleep disorders was initially stopped or markedly reduced to limit the spread of the SARS-CoV-2 virus [4, 18]. Staff at sleep units situated in hospitals were allocated to other medical services, in particular critical care, respiratory, infectious disease and internal medicine. As evidenced by data from questionnaires distributed to sleep centres or by the numbers of patients reported to national quality registries, sleep laboratories faced a substantial reduction of activities during the first lockdowns in Europe and elsewhere in the world [4, 18, 19]. In detail, several countries reported a more than 90% reduction of in-house sleep evaluations by polysomnography. Even overnight supervised CPAP titrations were no longer performed due the elevated risk of virus spread through CPAP treatment. In addition, patients were afraid to visit the hospitals/sleep units due to the risk of COVID-19. A substantial backlog occurred over the pandemic period for almost all types of sleep medicine services.
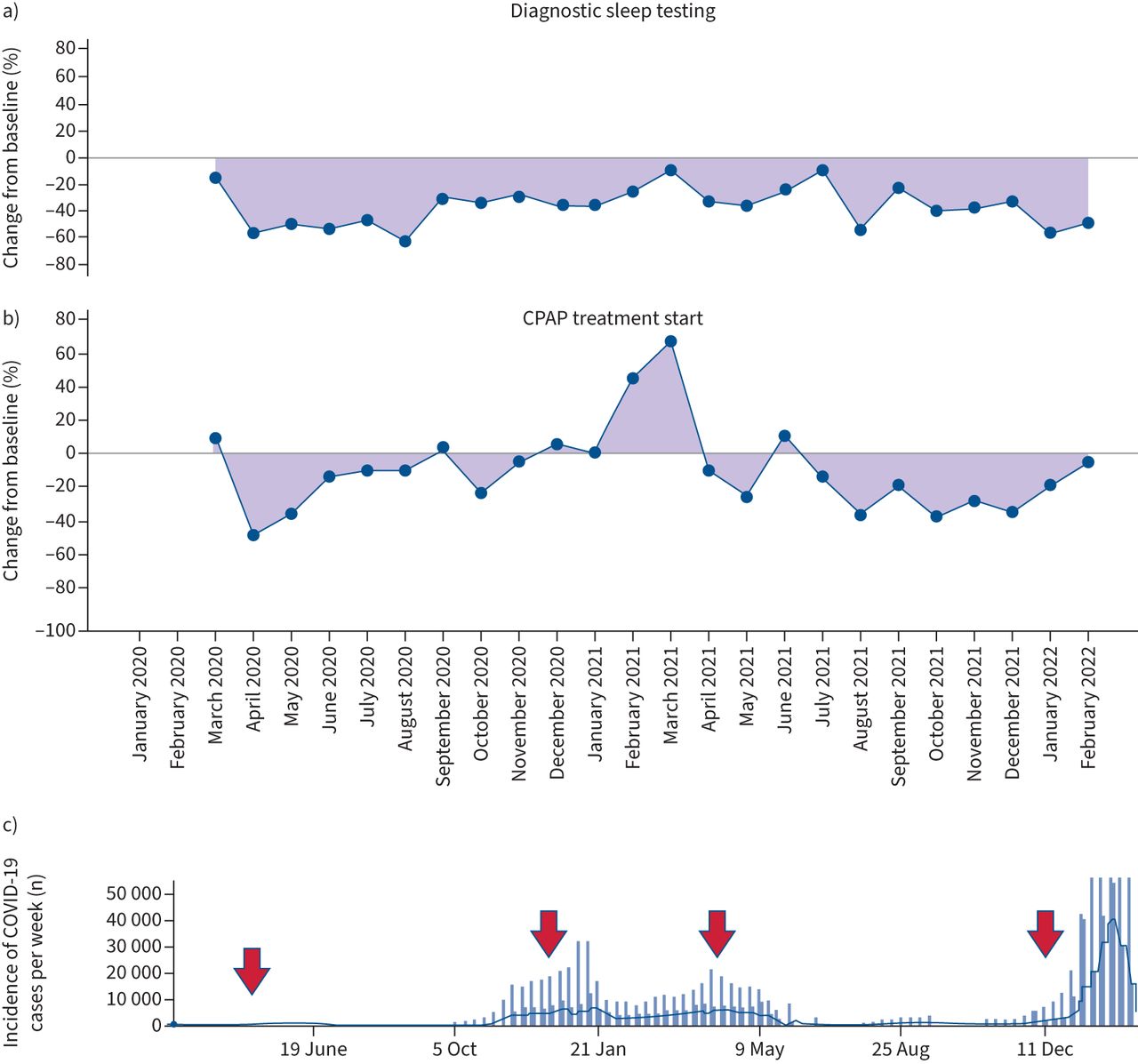
To further visualise this backlog and the transition of services over the pandemic, the National Swedish Sleep Apnea Registry (SESAR) recently published the change in the number of patients added to the register [18]. Using only centres reporting from 2018 onwards, mean values for the number of patients diagnosed and treated each month were established for 2018 and 2019 (13 788 patients for OSA diagnosis, and 10 188 starting PAP treatment and 1188 starting oral advancement therapy). Compared with the identical periods in March to December 2018 and 2019, the number of patients diagnosed with OSA was reduced by 43% and the numbers starting treatment with PAP or oral devices were reduced by 17% and 51%, respectively, during March to December 2020. During the first lockdown in spring 2020, the changes were most profound, and recovery was only observed for PAP treatment initiation (a prioritised activity). Interestingly, these number have now been updated for the entire pandemic period in 2021 and show still significantly reduced activity in the Swedish sleep centres linked to the SESAR throughout the entire pandemic period between March 2020 and February 2022 (figure 2). Reduction of sleep medicine services appears to be unrelated to the variation of verified COVID-19 incidence in the Swedish population. However, it should be kept in mind that data are reported manually through the SESAR webpage. This implies that the relative changes between 2018/2019 and 2020/2021 observed in this national registry could reflect both the reduced sleep medicine services and also in part reduced reporting by the sleep centres to the SESAR.
{kind=link}
{kind=link}
Changes in sleep medicine services for patients a) diagnosed with sleep apnoea and b) starting continuous positive airway pressure (CPAP) treatment. Data are from the Swedish Sleep Apnea Registry (www.sesar.se). Data are presented as the percentage change from baseline (mean value of registrations in the SESAR registry for each month as a percentage of the mean for 2018 and 2019). Data are only presented from centres reporting during the period 2018–2022. The zero-line indicates no change compared with the mean in 2018/2019. For diagnostic sleep testing the mean per month was calculated from 13 178 sleep diagnostic recordings in 2018/2019. The mean for CPAP treatment initiation was calculated from 10 173 patients in 2018/2019. The coloured area indicates the percentage change from these baseline levels. Data are presented for each month during the pandemic, from March 2020 until February 2022. Positive values indicate an increase, negative values indicate a reduction in reported patients. c) The incidence of PCR-positive COVID-19 patients in Sweden for the corresponding time period; arrows indicate the four main waves of the pandemic in Sweden. Data are from the COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (https://systems.jhu.edu/research/public-health/ncov/) [25].
The COVID-19 pandemic influenced other medical services closely linked to sleep medicine. For instance, services for patients on HMV were the subject of a recent questionnaire study [19]. Outpatient services were reduced by >90% and most centres were only able to offer appointments for initiation and follow-up of HMV in exceptional cases. The early wave of the pandemic induced a mean waiting list of close to 90 outpatient visits and up to four appointments to start HMV treatment at each centre. As treatment initiation and follow-up has a high medical priority in patients with chronic respiratory failure, this backlog is of high clinical significance.
Mitigation strategies to overcome the lockdown of sleep medicine practice
From start of the pandemic, the different networks of expert organisations collaborated on a national and international level to provide the best possible knowledge and evidence for sleep medicine centres. Expert societies in sleep and respiratory medicine took the lead for this work (e.g. European Respiratory Society, American Academy of Sleep Medicine, and national sleep and respiratory societies in Europe). As summarised in several reviews, national and international guidance documents were introduced and continuously amended from spring 2020 onwards [6, 18]. The European Respiratory Society published a consensus statement on the gradual reopening of sleep services [20]. The statement acknowledged national policies, reimbursement rules and the relative role of public versus private practices. It also highlighted the necessity to follow the overall national recommendations according to the epidemiological phase of the COVID-19 infection. The paper contained flowcharts approved by a European expert panel to guide healthcare personnel during COVID-19 screening and sleep diagnostic procedures, as well as PAP/HMV treatment procedures in sleep medicine centres. The recommendations outlined possible routes to continue with sleep medicine services using new routines to avoid personal contacts, patient travel, and any direct exposure of patients and personnel to the aerosols from PAP and HMV device treatment. These new routines were characterised by distance monitoring, use of single-use devices for diagnosis, and implementation of digital communication between the patient and healthcare professionals by phone, web-calls, and telemonitoring/telemedicine.
Caregivers for patients with other sleep disorders like insomnia also received guidance, with a recommendation for cognitive behavioural therapy (CBT) for insomnia treatment during the pandemic [21]. Increased levels of daytime stress, anxiety and depression, but also long-term COVID-19, might be potential causes for the elevated prevalence of chronic insomnia and disrupted sleep. The recommendations highlighted the link between pandemic-related stress factors and disturbed sleep. Adaptions of CBT elements were discussed, as routines at work and family life had changed and recommendations for physical exercise and social interaction may not be feasible under the circumstances of national lockdown.
Lessons learned in sleep medicine for future practice
The pandemic may have imposed a paradigm shift in sleep medicine: prior to the pandemic, the patient came to the healthcare professional. Sleep centres provided in-house services including overnight procedures for one or even several nights. This model did not work in most places during the pandemic and new care models were developed. Several of these changes in clinical practice during the pandemic are listed in table 1. As described in reviews and statement papers [20, 22], sleep specialists have learned that good medical practice can be provided if the healthcare professionals come to the patient by means of novel healthcare processes and tools. These tools may include posting out diagnostic equipment, cloud-based data transfer of medical information from devices, more home-based procedures for sleep diagnosis and treatment, video consultations, and digital communication with chats, text messages or phone-apps. In part, these technical solutions were already available prior to the pandemic but they were not frequently used in clinical routine at the beginning of the pandemic [4]. This low degree of use was probably due to the uncertainty about their advantages and disadvantages. However, the prolonged time of restrictions introduced by the COVID-19 pandemic facilitated a more rapid, worldwide implementation of, for instance, telemedicine. It is likely that these patient care models, based on experiences during the COVID-19 pandemic, will further influence sleep medicine practice in the next decade [20, 22].
Overview of changes to routine procedures in sleep medicine during the COVID-19 pandemic
Despite the positive experiences gained during the pandemic, a few clinically important questions need to be considered when discussing an ongoing paradigm shift in sleep medicine services. First, does the sleep specialist need to meet the patient in person to obtain a proper history for the diagnosis of sleep disorders? Probably not. However, whenever a physical status is required, for example to establish anatomic risk factors (upper airway anatomy) or to assess dental status prior to evaluation of mandibular advancement therapy in sleep apnoea, a physical meeting at the doctor's office is necessary. In cases of suspected sleep-related hypoventilation at least a cardiopulmonary status and an arterial blood gas test need to be performed. When hypersomnia of central origin or certain types of parasomnia disorders are suspected, a physical status including a neurological examination is mandatory.
Secondly, PAP treatment initiation and follow-up have been performed without mask adaptation and patient education on-site. A subgroup of patients may prefer this procedure as it saves time spent travelling and loss of productive working hours. However, there is evidence from studies that a remote start for PAP treatment is associated with reduced long-term compliance. A multicentre study in the UK compared the adherence rate with PAP treatment when started at a distance during the pandemic with historic data from 2018 and 2019, when PAP treatment was started during a face-to-face meeting [23]. They found that pre-pandemic median CPAP usage was 5.4 (2.7–6.9) h per night at the first follow-up and this fell by 0.9 h per night (95% CI 0.5–1.2, p<0.0001) in 2020. The authors state that they found clinically relevant reductions in CPAP usage with the pathway changes introduced post-COVID-19 [23]. Similar findings are reported in a study which allocated 666 patients to three pathways for PAP treatment initiation [24]. Patients in group A choose a group session for PAP education at the sleep clinic, while those in group B choose to receive the PAP equipment by shipment followed by a subsequent video-based training session. Group C was offered only treatment variant B during the COVID-19 pandemic. Group A was significantly more likely to continue PAP treatment (67%) compared with groups B and C (54% and 56%, respectively).
Thirdly, the integration of external communication systems (chat, text messages, telemonitoring solutions) and data transfer into the medical records are not yet automated; time-consuming double reporting or manual transfer between systems is necessary. The legal aspects for cloud-based data transfer as well as the ownership of patient-related data are still unresolved and under review in many countries. There is strong evidence that distance monitoring and direct patient communication are helpful tools to improve patient outcomes, but some legal questions may need further consideration.
Finally, reimbursement models for medical care based on digital/remote consultation and telemedicine-based patient follow-up using novel technologies may not be fully established and calibrated against the actual workload.
Conclusions
The data available today provide emerging evidence that OSA might be one additional, independent risk factor for adverse outcomes in SARS-CoV-2 infections. The pandemic resulted in a significant and long-standing reduction in sleep medicine services and there is a high risk of a substantial backlog for sleep medicine services in the coming years. However, mitigation strategies were developed, and a broad consensus was reached on a national and international level taking the local, regional and national variation in the pandemic into consideration. The sleep medicine field is now better prepared for upcoming challenges during a pandemic.
By using modern technologies and new working models we all have gained knowledge and experiences during the pandemic which will help us to adapt the services to our patients’ preferences and needs. This knowledge will of course influence future sleep medicine management. Scientific work-up of the pandemic and its influence on sleep in the population and on patients with different sleep disorders will continue to grow, and the number of scientifically sound publications is rapidly increasing. It is anticipated that the lessons learned during the pandemic will influence sleep medicine practice in the coming decade. Thoughtful implementation of this new knowledge along with solid scientific validation compared with standard of care is recommended.
Key points
The role of sleep apnoea as a risk factor for a worsened outcome of COVID-19 infection, evidenced as hospitalisation, need for intensive care or fatal outcome, is not yet fully understood. Several studies suggest that untreated OSA is a risk factor for severe COVID-19 infection, but this association becomes weaker after controlling for confounders like obesity and hypertension. The impact of OSA treatment on the elevated risk is less frequently studied.
The COVID-19 pandemic led to a profound reduction of sleep medicine services in many countries and hospitals. Services have not fully recovered 2 years after the start of the global pandemic.
The pandemic led to substantial changes in sleep medicine services. In-hospital diagnostic and treatment services were changed to remote patient contacts including telephone calls, video meetings and telemedicine-based remote control of diagnostic procedures, and CPAP initiation and follow-up procedures.
Self-evaluation questions
What are the possible pathways for the development of sleep disorders during the COVID-19 pandemic?
What risk factors do severe COVID-19 and OSA have in common?
Is there a higher risk of severe COVID-19 in patients with known OSA?
How does PAP treatment interfere with SARS-CoV-2 infection?
What mitigation strategies have been implemented at sleep medicine centres to continue patient care during the COVID-19 pandemic?
What lessons have been learned from the COVID-19 pandemic regarding future sleep medicine services?
Suggested answers
1) Direct central nervous system engagement of the SARS-CoV-2 virus; 2) cardiopulmonary engagement of COVID-19 disease, including respiratory symptoms like cough and dyspnoea and other manifestations like fever and headache; 3) change in lifestyle during the pandemic (e.g. lockdown, working at home, restrictions in daily life routines); 4) worry and increased anxiety during the pandemic (e.g. risk of infection and severe COVID-19, increased risk for familiy members, economic stability).
Older age, male sex, obesity, and cardiometabolic comorbidities like hypertension and diabetes.
The evidence from epidemiological studies is increasing that OSA may be an independent risk factor for severe COVID-19. However, there are no data available today explaining the exact mechanisms behind this association.
PAP may increase the risk for contamination and virus spread, but the evidence is rather weak. There are no convincing data available as to whether treatment of OSA by PAP can substantially reduce the risk for severe COVID-19 or improve the outcome of patients with severe COVID-19. OSA patients on PAP treatment may have slightly increased the amount of PAP use during the pandemic, but this increase is not considered clinically relevant.
Several mitigation strategies have been suggested: 1) regular testing of patients prior to visiting the sleep medicine facility; 2) change in routines at sleep medicine centres with home sleep testing and home titration of PAP instead of in-lab procedures; 3) remote follow-up procedures including telemonitoring of PAP devices, phone calls and video meetings with patients instead of in-lab patient visits; 4) adaptation of routines in relation to the local/national recommendations and the status of the pandemic.
In general terms, pre-pandemic services were characterised by the fact that the patient came to the sleep centre. During the pandemic, the sleep healthcare professionals came to the patient by means of new technologies (telemedicine-based diagnosis and treatment follow-up, video consultations). The usefulness of these new routines for sleep medicine services outside the pandemic is under scientific evaluation and review.
Footnotes
Conflict of interest: L. Grote reports grants or contracts from the Swedish Heart and Lung Foundation (No. 20180567, 20210529), the agreement with the Swedish Government concerning research and education of doctors(ALFGBG-725601 and -966283), EU Horizon 2020, EUROSTAR (grants: “Sleep Revolution”, “Apnoeaway”, and “WATCH-IT”), and Desitin (clinical trial contract); royalties or licenses from Desitin (pharmacologocal treatment in OSA); lecture fees from AstraZeneca, Lundbeck, Resmed and Philips; and leadership or fiduciary role in other board, society, committee or advocacy group from National guidelines for treatment in OSA Chair (part of regular salary), National quality registry for sleep apnea (SESAR) Chair (part of regular salary), European quality registry for sleep apnea (ESADA) (steering group member, unpaid), European Respiratory Society, Assembly 4 (LRPC member, unpaid) and European Sleep Research Society (examination committee, unpaid).
- Received May 23, 2022.
- Accepted June 30, 2022.
- Copyright ©ERS 2022
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- The relationship between SARS-CoV-2 infections and sleep disorders
- The risk for severe COVID-19 infection in patients with OSA
- The use of PAP treatment during the COVID-19 pandemic
- The effect of the COVID-19 pandemic on sleep medicine practice
- Mitigation strategies to overcome the lockdown of sleep medicine practice
- Lessons learned in sleep medicine for future practice
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics