





Abstract
Accumulated evidence supports the efficacy of noninvasive respiratory support therapies in coronavirus disease 2019 (COVID-19)-related acute hypoxaemic respiratory failure, alleviating admissions to intensive care units. Noninvasive respiratory support strategies, including high-flow oxygen therapy, continuous positive airway pressure via mask or helmet and noninvasive ventilation, can be alternatives that may avoid the need for invasive ventilation. Alternating different noninvasive respiratory support therapies and introducing complementary interventions, like self-proning, may improve outcomes. Proper monitoring is warranted to ensure the efficacy of the techniques and to avoid complications while supporting transfer to the intensive care unit. This article reviews the latest evidence on noninvasive respiratory support therapies in COVID-19-related acute hypoxaemic respiratory failure.
Abstract
In COVID-19-related acute hypoxaemic respiratory failure, noninvasive respiratory support therapies have been shown to reduce the risk of intubation and they should be considered safe and adequate, in the proper setting and with experienced teams https://bit.ly/3GQbgKs
Introduction
In the first phases of the pandemic, due to the fears of rapidly progressive coronavirus disease 2019 (COVID-19)-related acute hypoxaemic respiratory failure (AHRF) and putative nosocomial infection risks, there was a trend for advising early intubation and invasive mechanical ventilation (IMV) instead of noninvasive respiratory support therapies [1]. Subsequent prospective cohort studies confirmed that noninvasive respiratory support therapies improved outcomes compared with early IMV [2, 3] and that noninvasive respiratory support therapies were not “generating” but rather “dispersing” bioaerosols farther away from the patient [4]. However, in patients not responding to noninvasive respiratory strategies, early intubation and a switch to IMV were highly recommended [5].
The use of noninvasive respiratory support therapies has evolved over time during the pandemic. In the beginning, the scarcity of noninvasive respiratory support devices prompted the repurposing of existing continuous positive airway pressure (CPAP) and noninvasive ventilation (NIV) machines [6–8]. Noninvasive respiratory support therapies became the first-line intervention for COVID-19-associated AHRF as experience was gained about its efficacy and safety [9] and manufacturers increased production [10]. Furthermore, noninvasive respiratory support therapies outcomes and management have changed over time depending on pandemic waves [11], COVID-19 vaccination coverage [12], circulating viral variants [13], and published evidence [14, 15].
Description of noninvasive respiratory support therapies
AHRF is the result of a range of pathophysiological processes and patients with this condition will require respiratory support while the underlying pathology is treated. It has been increasingly recognised that different therapeutic strategies to provide oxygenation and to offload the work of breathing in AHRF impact on clinical outcomes [16]. The term “noninvasive respiratory support therapies” is increasingly used to describe medical interventions providing oxygenation and/or ventilation to patients with AHRF that represent a higher level of support than conventional oxygen therapy (COT) alone but fall short of IMV. Noninvasive respiratory support therapies encompass several discrete therapies, principally CPAP, NIV and high-flow oxygen therapy (HFT). Both CPAP and NIV have been used in the management of acute respiratory failure to provide respiratory support without the need for IMV and its associated morbidity, with HFT being introduced as an alternative method in recent years, and adoption of these strategies has been accelerated by the challenges posed by the COVID-19 pandemic.
CPAP provides a single continuous positive airway pressure that improves oxygenation by increasing functional residual capacity, recruiting poorly ventilated lung regions, and therefore improves the operating lung volume and the ventilation/perfusion matching. As there is a single level of pressure, CPAP does not require synchronisation with the patient and so it is simpler to set-up and deliver than NIV. NIV provides a higher level of pressure delivered during the inspiratory phase (inspiratory positive airway pressure (IPAP) or pressure support (PS)) and a positive end-expiratory pressure (PEEP), showing the same physiological benefits as IMV, reducing muscle loading and work of breathing and improving gas exchange [17]. NIV requires a degree of synchronisation between the ventilator and patient, and therefore, requires more skill for set-up and effective delivery than CPAP. CPAP and NIV may be delivered via the same devices used for IMV, but there are also a range of dedicated noninvasive ventilator devices which offer potential advantages. The terminology to describe the modes and settings of devices are not standardised and so familiarity with the models in question is important. They can both be delivered via single-limb or dual-limb circuits, but whichever system is used, it is important to realise that the use of a noninvasive interface will lead to unintentional leaks, which can impact ventilator performance and patient–ventilator synchrony. The latter needs to be appreciated as it is associated with negative physiological and clinical consequences. CPAP and NIV are commonly delivered via a range of oronasal masks but also using other interfaces, including the helmet (figure 1), with the latter allowing for the delivery of higher PEEP and minimal leaks [18].
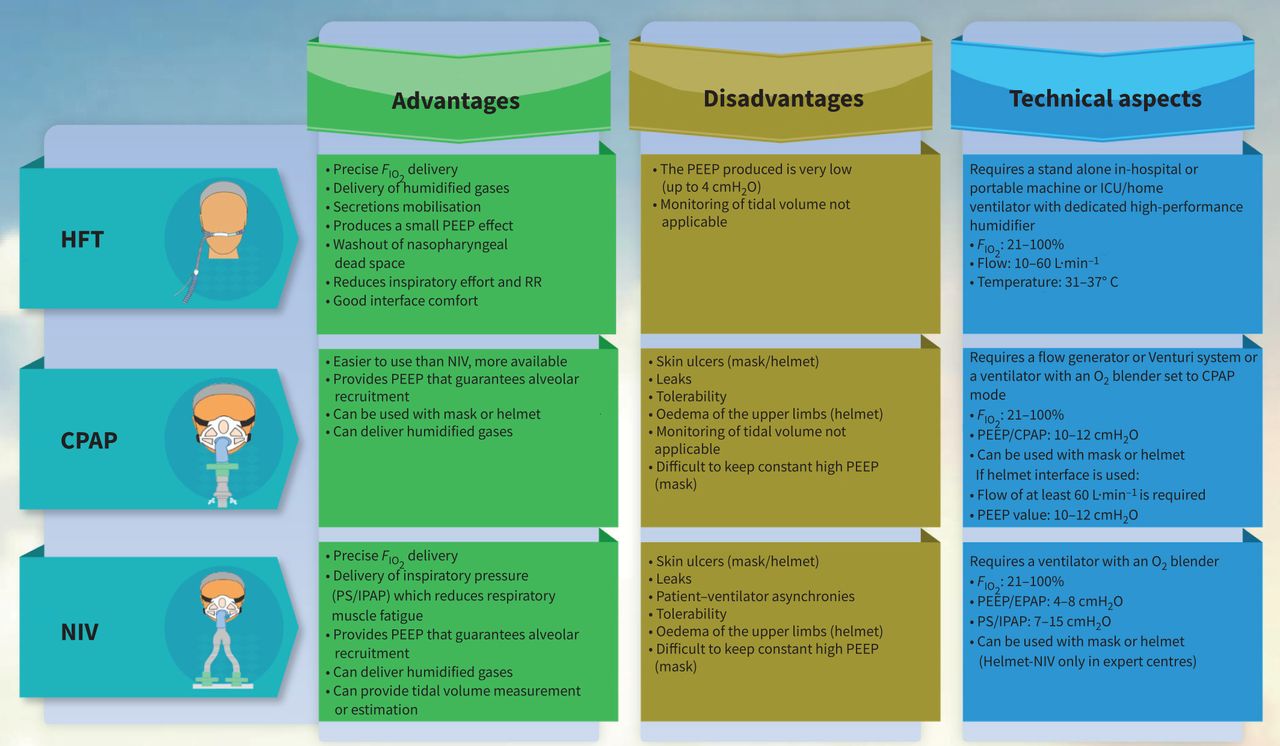
Noninvasive respiratory support therapies for acute hypoxaemic respiratory failure. HFT: high-flow oxygen therapy; CPAP: continuous positive airway pressure; NIV: noninvasive ventilation; FIO2: fraction of inspired oxygen; PEEP: positive end-expiratory pressure; RR: respiratory rate; ICU: intensive care unit; PS: pressure support ventilation; IPAP: inspiratory positive airway pressure; EPAP: expiratory positive airway pressure.
HFT delivers warmed and humidified air at flow rates above that of COT, usually between 15 and 60 L·min−1, thus matching patients' inspiratory peak flow, even in patients with high demand. Therefore, HFT provides accurate delivery of the set fraction of inspired oxygen (FIO2), limiting the dilution of the inhaled oxygen with room air and including humidification to prevent airway drying and facilitate mucociliary clearance. Moreover, HFT provides a washout of airway dead space, a flow-dependent reduction in inspiratory effort as well as a PEEP effect proportional to the flow rates while ensuring patient comfort [19]. Due to this strong physiological rationale, HFT has been suggested as an alternative to NIV in patients with AHRF [20].
Noninvasive respiratory support therapies in AHRF: evidence before the COVID-19 pandemic
Most studies in critical care combine both CPAP and NIV, with the addition of pressure support being optional and titrated to work of breathing. NIV has become the gold standard in the management of acute hypercapnic respiratory failure in patients with COPD [21] and is used in clinical practice beyond this indication in obesity and neuromuscular disease [22]. However, the use of NIV and CPAP in AHRF is more controversial, with potential harm in patients with the most severe lung injury (arterial partial pressure of oxygen (PaO2)/FIO2<150 mmHg) [23] and a variance in efficacy based on the underlying pathophysiological process. Indeed, the physiological effects of CPAP and NIV are different and the choice between these two modalities might affect the clinical outcome. Although few comparative studies between CPAP and NIV are available, both techniques improve oxygenation; however, physiological studies showed that CPAP has minimal effects on respiratory effort, while NIV (with the combination of pressure support and PEEP) unloads the respiratory muscles reducing inspiratory oesophageal pressure swings and improves dyspnoea relief [24, 25]. Therefore, CPAP could be preferred if the effort is low and NIV if the effort is high. Thus, CPAP and NIV are recommended in specific subgroups of patients with their use in patients with de novo acute respiratory failure limited to patients with less severe disease and in an appropriate clinical context that allows access to rapid escalation and a switch to IMV if needed. Specific groups with AHRF that may benefit from CPAP and/or NIV include acute cardiogenic pulmonary oedema, post-surgical and immunocompromised patients [26, 27].
The data to support HFT being used in isolation or as an alternative to NIV have been increasing over the past decade and have now been incorporated into formal clinical practice guidelines [20]. HFT offers a simpler interface and requires less technical skill than NIV and this is demonstrated by the higher duration of this treatment delivered to patients during clinical trials [28]. The evidence to support HFT as the noninvasive respiratory support therapy of choice in patients with de novo acute respiratory failure is equivocal, but there is clear evidence of efficacy, with a reduction in mortality and intensive care unit (ICU) length of stay compared with COT [29, 30]. However, the level of certainty of superiority of HFT over NIV is low due to the heterogeneity of the patient populations in clinical trials and the deviations from current best practice, in particular, the limited duration of NIV delivered in some of the intervention periods [20, 31]. However, guidelines suggest the use of HFT as a first-line treatment for de novo respiratory failure because of the possible harmful effects of facemask NIV.
Prior to the COVID-19 pandemic, there was increasing evidence supporting noninvasive respiratory support therapies to manage patients with AHRF, with the use of HFT in particular expanding due to clinical benefits and ease of application. The choice of noninvasive respiratory support therapies should be carefully considered, with underlying patient characteristics (e.g. premorbid respiratory disease), the pathophysiological driver of AHRF and the skill mix of the clinical team all being important aspects of the decision-making.
Noninvasive respiratory support therapies: an aerosol-generating procedure?
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was the first pandemic to hit the world rapidly with healthcare professionals knowing so little about the infective agent. After the identification of the virus, it became a priority to understand how SARS-CoV-2 disseminated. As for all respiratory diseases, viral aerosol transmission was rapidly identified as the main source of contamination [32].
During the first phase of the pandemic, given the high rate of infections amongst healthcare professionals, extensive precautionary measures were taken [9]. Hence, all procedures at risk of generating aerosols were to be performed with extensive personal protective equipment. Numerous strategies were suggested to avoid contamination of healthcare workers. Modified NIV circuits with 3-D printed materials [33] and canopies [34] were suggested as approaches to reduce aerosolisation. However, these suggestions were not without consequences for the delivery of care. It was shown that the change in NIV circuits and the insertion of antimicrobial filters at the expiratory port was associated with an increase in dead space [35] and work of breathing, and changes in ventilator performance, including an increased rate of patient–ventilator asynchrony [36] that are associated with a worse prognosis [37].
These recommendations to limit exposure to aerosol-generating procedures contributed to an increase in the burden of care needed for the management of infected patients. Even though preliminary surface analysis showed reassuring results [38], data exploring aerosol generation were communicated after the second wave of the pandemic [39]. These studies showed that the delivery of CPAP and NIV was not associated with aerosol emission [40]. However, proper mask fitting is crucial to avoid leaks that are associated with viral aerosol dispersion [41]. It was also shown that the use of HFT generated aerosols; however, most of them originated from the high-flow device rather than from the patient [42].
Currently, guidelines recommend the use of eye protection for all care of patients infected with SARS-CoV-2 and the use of N95 masks for aerosol-generating procedures (physiotherapy, bronchoscopy, intubation). In addition, good aeration should be organised in all rooms in which patients with SARS-CoV-2 are hospitalised [43].
The issue of patient self-inflicted lung injury and how to make spontaneous effort non-injurious during noninvasive respiratory support therapies
Ventilator-inflicted lung injury is a well-known complication from mechanical ventilation that contributes to the severity of acute respiratory distress syndrome (ARDS) and has led to a reduction in the targeted volume set during IMV [44]. For patients that do not require IMV, noninvasive respiratory support therapies can be given to patients [29]; however, in such circumstances, it is not possible to control the tidal volume generated by the patient. The patient's spontaneous tidal volume can be important and may contribute to lung injury itself. Patients' high respiratory drive and intense inspiratory effort result in large tidal volumes and dynamic variations in transpulmonary pressure that may worsen lung damage. The consequent generation of asynchronous and inhomogeneous alveolar ventilation, mainly in the dependent dorsal region, defined as “pendelluft phenomenon”, promotes an abnormal increase in transvascular pressure that worsens the alveolar and interstitial oedema and heterogeneous transmission of muscular pressure and diaphragmatic injury, all yielding ventilator inhomogeneity, local overstretch and worsening inflammation. The regional increase in transpulmonary pressure increases lung stress and may perpetuate lung injury; this phenomenon occurring during spontaneous breathing is described as patient self-inflicted lung injury (P-SILI) [45]. High PEEP promotes lung recruitment during spontaneous breathing and avoids the emergence of the pendelluft phenomenon mitigating lung injury [46]. However, an increased risk of developing P-SILI may occur because of the persistence of high inspiratory effort despite noninvasive respiratory support therapies, which is associated with treatment failure and need for IMV [47, 48].
With the SARS-CoV-2 pandemic, the use of noninvasive respiratory support therapies has increased significantly. COVID-19-related AHRF is associated with an increased respiratory drive that may contribute to the onset of P-SILI [49]. Increased respiratory drive, in combination with the alveolar damage caused by SARS-CoV-2 infection, may contribute to the increased rate of pneumomediastinum reported in SARS-CoV-2 infection [50, 51].
Monitoring respiratory effort without invasive measurements is challenging in clinical practice in patients using COT or noninvasive respiratory support therapies. However, bedside clinical evaluation may provide useful insights, especially when patients have an increased respiratory rate (RR) and large thoracic movements. In this setting, an improvement in the ROX index (the ratio between RR and peripheral oxygen saturation (SpO2)/FIO2) may also be a useful tool [52]. Preliminary results have suggested that monitoring pressure swings in HFT nasal cannula may be an easy-to-use surrogate of respiratory effort [53]. For patients treated with CPAP [54], data from the ventilator, in the absence of leaks, can provide information on the estimated delivered tidal volume [55].
Monitoring of noninvasive respiratory support therapies in AHRF
As an intervention made in a critical or “semi-critical” patient, and due to the failure rate reported in most trials (ranging from 20 to 50% [56]), cautious monitoring of the response to noninvasive respiratory support therapies is always needed. Monitoring tools for noninvasive respiratory support therapies may be divided into three different categories: bedside clinical variables and physiological scales, physiological “invasive” measurements, and imaging techniques (table 1).
Tools for monitoring noninvasive respiratory support therapies in acute hypoxaemic respiratory failure
Bedside clinical variables and physiological scales
Simple clinical observation may be enough to determine when a patient is at high risk of failure. The initial severity of the oxygenation impairment (i.e. PaO2/FIO2 <150 mmHg) [23] or the lack of improvement [57] may be predictors or indicators of noninvasive respiratory support therapy failure. In ICU or high-dependency unit settings, arterial catheterisation may allow for frequent arterial blood gas sampling; however, it is not a continuous monitoring tool and can be associated with vascular injuries [58]. As noted by Winck and Scala [59], when using high FIO2, PaO2/FIO2 ratio may not reflect the severity of the exchange, and baseline arterial partial pressure of carbon dioxide needs to be considered; perhaps the use of the alveolo–arterial gradient may be more accurate.
Oxygenation can be continuously monitored by peripheral pulse oximetry. It is reliable, easy to use, noninvasive and widely available, but in severely hypoxaemic patients it may have some limitations. In particular, early in the COVID-19 pandemic, a phenomenon called “silent hypoxia” disconcerted physicians. Awareness of the limitations of pulse oximetry and the lack of information on the whole gas exchange (as it does not provide information on hypo- or hypercapnia) are necessary to avoid misinterpretation [60, 61].
RR is one of the most relevant physiological variables related to the success or failure of noninvasive respiratory support therapies. The main advantages of RR are that it is easily measured at the bedside and can be continuously recorded. Although it is poorly correlated to the intensity of the inspiratory effort [62], a high RR at the beginning or the absence of its decrease after a short period of noninvasive respiratory support therapy may reflect the severity and high probability of failure. Blez et al. [63] evaluated the change in RR at 30 min after starting noninvasive respiratory support therapies, as a sole predictor of success or failure, with a similar performance as other more commonly used indexes. With these simple bedside physiological measurements some clinical scales have been proposed: a purely clinical scale, with easy-to-record variables, is the WOB (work of breathing) scale [64]. Developed for COVID-19 patients, it takes into account the RR, the presence of nasal flaring, and the use of accessory muscles (sternocleidomastoid and abdominal muscles) and it is intended to measure “inspiratory effort”.
The HACOR score (heart rate, acidosis, consciousness level, oxygenation, and RR) has been proposed as a bedside tool for predicting NIV failure [65]. It has been recently updated, including six new variables related to the aetiology of ARDS (pneumonia, cardiogenic pulmonary oedema, pulmonary ARDS, immunosuppression, and septic shock) and the sequential organ failure assessment score (SOFA score) [66]. It seems to improve diagnostic capabilities when compared with the “original” HACOR score, especially at baseline and in the first 1–2 h.
Another score of interest in predicting outcomes under HFT is the ratio of SpO2/FIO2 to respiratory rate (Respiratory rate–OXygenation, ROX index) [67], which was developed and validated as a tool for predicting success or failure of HFT. It is a simple and reliable tool that is broadly available, but with the limitations of both the SpO2 measurement and the physiological meaning of the RR. In COVID-19 patients, Chandel et al. [68] demonstrated that a ROX index >3.0 at 2, 6 and 12 h after initiation of HFT was 85.3% sensitive for identifying HFT success. By contrast, Zucman et al. [69] determined that the most sensitive cut-off point for intubation risk was 5.37 at 4 h. Regarding patients with HFT outside ICU, Vega et al. [70] determined that the value with the highest sensitivity was 5.9, while the classic value of 4.88 was not sufficiently discriminating. Other authors found different cut-off levels, such as 4.9, and evaluated the ability to avert delayed intubation-induced mortality [71]. When tested in patients with COVID-19 pneumonia, they seem to have similar performance but are humbler than what was reported in the original development and validation papers. In more detail, for a ROX index cut-off point of 5.6 a sensitivity of 62% and a specificity of 65% were reported, while for a HACOR scale of 5.5 a sensitivity of 66% and a specificity of 65% were noted [72]. The ROX index has also been tested in COVID-19 patients receiving CPAP with promising results in short-term follow-up: a ROX index <6.64 after 24 h of CPAP shows excellent accuracy in predicting treatment failure [73].
Monitoring the trends of all these scores in conjunction with clinical judgement may be a more useful and cautious approach rather than focusing on a single figure of a score.
Physiological “invasive” measurements
In recent years, there has been increased interest in the concept of alveolar damage induced by spontaneously breathing patients with increased respiratory drive, also known as P-SILI. Under respiratory distress, a spontaneously breathing patient may exhibit huge swings in transpulmonary pressure. Some conflicting data (and opinions) have been flowing in the medical literature in the past few years [74]. The gradient between the alveolar pressure and the pleural pressure (approached by the oesophageal pressure measurement (Peso)), known as the transpulmonary pressure, reflects the expenditure of pressure to distend the chest wall and the lung. High transpulmonary, dynamic driving pressures are linked to the development of P-SILI. Inadequate settings of CPAP or NIV and/or persistent high inspiratory effort may be detected by monitoring Peso, allowing for a timely decision on when IMV and muscle relaxation may be needed. Some physiological studies have focused on the ability of NIV, in contrast with HFT and CPAP, to decrease inspiratory effort, thus, maintaining transpulmonary pressure within safe levels with adequate levels of PEEP [75]. Tonelli et al. [48] showed that the magnitude of inspiratory effort relief, as assessed by Peso variation within the first 2 h of NIV, represents an early and accurate predictor of NIV outcome at 24 h. Coppola et al. [76] demonstrated that, with continuous measurement of Peso, the early predictors of failure (measured on the first day of treatment) under CPAP or pressure support treatment were the PaO2/FIO2 ratio, the intensity of changes in Peso, and the total lung stress. This last concept, which was the only independent factor related to failure in the multivariate analysis, is equivalent to the total transpulmonary pressure. Classical approaches to pulmonary mechanics are limited in the non-intubated patient (i.e. an occlusion manoeuvre cannot be performed), but Peso can be a useful tool to determine the bounds of safety for noninvasive respiratory support therapies.
Imaging techniques: lung ultrasound and electrical impedance tomography
In recent years, there has been a progressive increase in interest in lung ultrasound (LUS) applied to acute respiratory failure. LUS can identify regional areas of atelectasis, can guide recruitment, and is simple, easy to use and to learn, broadly available and is a non-radiation technology. However, it may have some operator-dependent results, and it cannot evaluate the lung as a whole in a single view. Some authors have explored the utility of LUS to guide noninvasive respiratory support therapies, focusing on assessment of recruitability. As an example, it can guide the indication for prone positioning in patients receiving HFT [77].
Electrical impedance tomography (EIT) is also a non-radiation, noninvasive technology that provides dynamic lung aeration imaging. It is based on the difference in resistance to electrical currents between air and other tissues and can generate continuous imaging of the way the lung inflates and deflates through multiple respiratory cycles. EIT allows for the differentiation of regional differences in lung strain and stress and may guide the correct level of external pressure, avoiding regional overdistension [78]. Although it has been mostly used in a small number of patients, EIT can identify those patients where there is still an ability to recruit the lung under positive pressure. End-expiratory lung impedance may be the variable that can help to titrate the optimal level of positive pressure needed. It can also drive the use of complementary interventions, such as the “awake prone position”, providing a more accurate evaluation of their usefulness [79].
Noninvasive respiratory support therapies trends during the COVID-19 pandemic
Noninvasive respiratory support therapies were widely used during the COVID-19 pandemic, with a marked variability worldwide, in an attempt to avoid the need for IMV despite the lack of consensus towards their use [80, 81]. A recent, pre-pandemic network meta-analysis conducted by Ferreyro et al. [16] revealed that noninvasive respiratory support therapies might be more effective than COT alone for the management of patients with AHRF. The meta-analysis showed that treatment with NIV delivered by both helmet and mask was significantly associated with a lower risk of death, and the use of both NIV and HFT decreased the risk of endotracheal intubation compared with COT in adults with AHRF. However, most of the studies included in this meta-analysis enrolled patients with AHRF due to community-acquired pneumonia, and the pathophysiological abnormalities underlying hypoxaemia in patients with pandemic viral illness might be different.
Recently, a growing number of randomised controlled trials (RCTs) have tried to provide evidence on the effectiveness of noninvasive respiratory support therapies in the management of COVID-19-associated AHRF. The first study comparing noninvasive respiratory support therapies in patients with COVID-19-associated AHRF was the Italian multicentre HENIVOT trial [82], which compared helmet-NIV (delivered as bilevel positive airway pressure (BIPAP)) and HFT and reported no difference in days free of respiratory support within 28 days (20 (IQR, 0–25) versus 18 (IQR, 0–22) days). However, the intubation rate in the helmet group was significantly lower compared to HFT (30% versus 51%, unadjusted odds ratio (OR) 0.41 (95% CI 0.18–0.89)) [82].
A large multicentre RCT conducted in 48 hospitals in the UK, the RECOVERY-RS trial, recruited 1273 hospitalised COVID-19 patients with an oxygen saturation of 94% or less despite receiving a FIO2 of at least 0.40. Patients were randomised to receive either CPAP, HFT, or COT, in a parallel group, open label, three arm, adaptive RCT [54]. CPAP, when compared with COT, significantly reduced the combined primary endpoint of tracheal intubation or mortality within 30 days (36.3% versus 44.4%; unadjusted OR 0.72 (95% CI 0.53–0.96), p=0.03). Most of the difference in the primary outcome was driven by a decrease in the intubation rate (33.4% versus 41.3%, OR 0.71 (95% CI 0.53–0.96)), while CPAP did not reduce mortality compared with COT (16.7% versus 19.2%, OR 0.84 (95% CI 0.58–0.96)). There was no significant difference between HFT versus COT in the primary outcome. However, the study did not meet the pre-planned sample size, and this may have reduced the precision in the estimate of the treatment effect with CPAP and the study may have been underpowered for the comparison between HFT and COT.
The HiFLo-COVID RCT [83], conducted in three centres in Colombia, demonstrated that among patients with severe COVID-19 (PaO2/FIO2 <200 mmHg) HFT significantly reduced the risk of intubation (hazard ratio (HR) 0.62 (95% CI 0.39–0.96), p=0.03) and time to clinical recovery (HR 1.39 (95% CI 1.00–1.92), p=0.047) compared with COT. However, a recently published international multicentre RCT, the COVID-HIGH trial [84] performed on patients with COVID-19 pneumonia and mild hypoxaemia (PaO2/FIO2 >200 and <300 mmHg), demonstrated that the use of HFT did not significantly reduce the likelihood of escalation of respiratory support (absolute risk difference −8.2% (95% CI −18–1.4%); risk ratio 0.79 (95% CI 0.59–1.05), p=0.09) or the likelihood of clinical recovery (69.1% versus 60.8%; absolute risk difference 8.2% (95% CI −1.5–18.0%), risk ratio 1.14 (95% CI 0.98–1.32)) compared with COT. Thus, the attractive pathophysiological effects of HFT are unlikely to significantly affect the clinical course of COVID-19 pneumonia-related mild hypoxaemia compared with COT. However, the study power was limited; therefore, a clinically meaningful benefit from HFT in this patient population could not be definitely ruled out. HELMET-COVID [85] was a multicentre RCT conducted in Saudi Arabia investigating the use of helmet-NIV (delivered as BIPAP) compared with usual respiratory support (mask NIV, HFT and COT) in 320 adults with AHRF related to COVID-19. Helmet-NIV did not significantly reduce 28-day mortality compared with usual respiratory support (27.0% in the helmet group versus 26.1% in the usual respiratory support group; risk difference 1.0% (95% CI −8.7–10.6%); relative risk 1.04 (95% CI 0.72–1.49), p=0.85). However, the lack of a clinically important treatment effect for helmet-NIV compared with the usual respiratory support group might be related to a reduced study power due to a lower-than-expected event rate. The SOHO-COVID trial [86] was a RCT conducted in 34 ICUs in France that compared the use of HFT and COT in 711 patients with AHRF due to COVID-19. HFT did not significantly reduce the mortality rate at day 28, which was 10% (36 out of 357) with HFT and 11% (40 out of 354) with COT (absolute difference −1.2% (95% CI −5.8– 3.4%), p=0.60). The COVIDICUS trial [87] was a RCT including 546 patients and comparing those receiving high-dose dexamethasone with standard of care dexamethasone and assessing HFT or CPAP compared with COT. No significant difference for the cumulative incidence of IMV criteria at 28 days among oxygenation strategies compared with COT was found (COT versus CPAP: HR 1.08 (95% CI 0.71–1.63); COT versus HFT: HR 1.04 (95% CI 0.69–1.55)).
Noninvasive oxygenation strategies algorithm
For early screening of noninvasive respiratory support therapies failure, some authors have proposed specific nomograms [88] or algorithms [59]. Despite the accumulated evidence supporting the use of different noninvasive respiratory support therapies in COVID-19-related AHRF, when to start, escalate and de-escalate therapy, and which is the best respiratory support option for the different timing/phenotype of the disease still needs to be completely defined. A balance between the benefits of maintaining spontaneous breathing and avoiding IMV while preventing the risk of prolonged exposure to strong inspiratory effort and treatment failure is strongly advised. A noninvasive oxygenation strategy algorithm is proposed in figure 2. To allow better tolerance, HFT can be used between CPAP/NIV sessions [20], with close monitoring for approximately 3 h, with a focus on the ROX index [67], other respiratory strain scales [89] and, whenever possible, tidal volumes [90].

{kind=link}
{kind=link}
Noninvasive oxygenation strategy algorithm. COT: conventional oxygen therapy; SpO2: peripheral oxygen saturation; HFT: high-flow oxygen therapy; CPAP: continuous positive airway pressure; NIV: noninvasive ventilation; PaO2: arterial partial pressure of oxygen; FIO2: fraction of inspired oxygen; IMV: invasive mechanical ventilation; RR: respiratory rate; ROX index: the ratio between RR and SpO2/FIO2; HACOR score: heart rate, acidosis, consciousness level, oxygenation, and RR; WOB: work of breathing; LUS: lung ultrasound; EIT: electric impedance tomography.
Noninvasive respiratory support therapies in COVID-19-related AHRF: important indicators
Reviewing the seven recent RCTs addressing the application of noninvasive respiratory support therapies in COVID-19 [54, 82–87], the protocols employed, methodology and data collected in the published studies are somewhat heterogeneous. To better interpret the results of these trials, a full set of parameters and clinical details are essential (table 2). In fact, in one study PaO2/FIO2 ratio was not available [87]. The majority of the studies were undertaken in the ICU [82, 83, 85–87] and only four had specific and uniform equipment [82, 85–87], with one [85] allowing six different ventilators in the helmet arm. Sedation was implemented in two trials [82, 85] and pronation was used with differing percentages in all except one trial [87]. Excluding the COVID-HIGH trial [84] (that included less severe patients), efficacy of noninvasive respiratory support therapies to avoid intubation at 28 days was maximal in the helmet arm of the HENIVOT trial [82] and minimal in the HFT arm of the SOHO-COVID trial [86]. Mask on time was reported in three trials [82, 85, 86] and was clearly detailed (in hours) in the HELMET COVID trial [85].
Relevant outcomes in randomised controlled trials
Complementary interventions
Combined HFT and NIV
In clinical practice, it is not common to employ a single respiratory support strategy throughout the course of the disease. A stepwise increase from a first-line HFT approach to a step up to positive pressure therapy in cases with a lack of response has been proposed. This may have the pitfall of rescuing very few patients, as most of those who fail HFT will also fail in a positive pressure trial and may need intubation after all [91]. Thus, it has been considered an inappropriate strategy by expert group recommendations [92], suggesting that HFT failure may prompt direct intubation. More interesting is the sequential and combined use of both positive pressure and HFT. Patients may need to pause NIV for oral intake, hygiene, or even due to a need for a rest from the mask to avoid pressure sores, and HFT may be an excellent tool to maintain oxygenation and some (small) degree of positive pressure that may ameliorate de-recruitment [9].
Self-proning
Prone position (PP) in non-intubated patients has been proposed to increase oxygenation. In intubated ARDS patients, PP has multiple advantages as a tool that increases oxygenation, improves ventilation of dependent (collapsed) areas, and helps lung recruitment. A mean session duration of 16 h each day is recommended [93]. In the pre-COVID-19 era, it was also proposed as a feasible intervention in non-intubated patients based on some observational studies of moderate severity ARDS [94]. Thus, when COVID-19 was recognised as an ARDS condition, multiple observational studies showed feasibility and improvements in oxygenation after pronation of non-intubated patients, with or without noninvasive respiratory support therapies. Subsequently, some cohort observational studies gave more insights on the utility of this technique, demonstrating persistent oxygenation improvement after shifting from supine to prone in at least half of the patients [95, 96]. Therefore, experts recommended self-proning whenever patients needed supplemental oxygen to maintain oxygen saturation above 90% [97]. The POSITIONED study by Jagan et al. [98] found that self-prone positioning was associated with a decrease in intubation rates and mortality in patients without noninvasive respiratory support therapies.
However, in a retrospective study, Padrao et al. [99] found no differences in outcomes between self-proning and standard therapy in patients on COT. The APRONOX study compared outcomes of patients with different oxygenation support who underwent PP for at least 2 h duration [100]. A mean duration of 12 h per time of admission was achieved and SpO2/FIO2 ratio improved from 183 to 212 mmHg, with fewer patients requiring IMV in the prone group (23% versus 40%). In a meta-trial that included patients from six different trials under HFT with a mean PaO2/FIO2 at randomisation of around 150 mmHg, Ehrmann et al. [101] compared patients in the prone arm with the standard treatment arm. While prone time was hugely variable among participants and trials (with a mean of 5.6 h), patients in the prone group had a lower rate of a composite outcome (treatment failure or death). A number needed to treat of 15 to avoid treatment failure was demonstrated. No differences between groups were noted in terms of 28-day mortality, nor a worse outcome between those who failed in both groups (indirectly showing that treatment failure under a prone protocol has not got a worse prognosis than that under standard treatment).
Combining noninvasive respiratory support therapies with PP may be demanding both technically and in terms of human resources, but it seems to offer an advantage in reducing intubation rate in patients with moderate ARDS, especially when combining NIV and PP [102]. In contrast, other authors found no differences when using awake PP in patients requiring HFT [103]. Nevertheless, there are some shadows in the use of the “self-proning” strategy, despite the well documented benefits on oxygenation. A high proportion of patients do not tolerate this position [95, 104, 105]. Recent systematic reviews have also demonstrated an improvement in oxygenation, but no effect on intubation rates [106].
Due to some difficulties in the PP with NIV interfaces, such as the helmet, some variants that may also increase oxygenation have also been proposed. A so-called “Rodin's thinker” position [107], named after the famous sculpture, with the patient resting his chest on a chair in a semi-prone position, was found to improve oxygenation in 25 patients, maintaining its benefits after “re-supination”. Retucci et al. [108] proposed a trial of helmet CPAP mixing lateral and PP, but very few improvements were found, and benefits were lost after re-supination.
Duration of PP is also controversial. While it is known that in intubated patients, benefits are obtained with at least 16 h of PP [93, 109], there is great variability in the length of prone in the published experience; however, it seems that periods of less than an hour may not achieve relevant results. This heterogeneity in results and methods for the “self-proning” intervention has led to conflicting recommendations, such as recommendations from the Society of Critical Care Medicine, which considered that there was not enough evidence to recommend it [110]. Finally, the most recent meta-analysis, including more than 130 studies, with thousands of patients included, concluded that PP was able to improve oxygenation and reduce intubation rates, so it was recommended in patients with AHRF due to COVID-19 and a need for advanced respiratory support [111]. To date, PP seems to be a promising strategy that needs further evaluation in future high-quality research [112].
Automated controlled oxygen delivery
Oxygen control while on noninvasive respiratory support therapies may be a critical factor to ensure success. It is well known that hyperoxygenation may have deleterious effects, especially in hypoventilation patients, such as some COPD patients. But also, hypoxaemia may develop progressively, and SpO2 may frequently change over time, and the response to adequately titrate oxygen therapy may not be fast enough.
To address this need for fast response titration, automated oxygen delivered systems have been developed. A meta-analysis showed that automatic oxygen titration was associated with a reduction in length of both hospital stay and oxygen therapy, but no effects were found in terms of intubation rates or mortality [113]. For noninvasive respiratory support therapies, closed-loop oxygen titration systems have been integrated into respiratory support devices. In the HILOOP trial, Roca et al. [114] demonstrated that an automated oxygen titration system was able to ensure that SpO2 was kept between pre-set targets for more time, with lower intervention and workload for healthcare workers than manual titration. Similarly, Harper et al. [115] found that patients using the automated oxygen delivery spent more than 96% of the time within the oxygenation range limits, while in the manual group, it was 71% of the time.
In pandemic scenarios, with overwhelming human workload demands and a shortage of oxygen supplies, these new automated methods may allow us to decrease the need for human interventions in oxygen delivery adjustments, and optimise oxygen consumption, rationalising its supply.
Conclusions
In COVID-19-related AHRF, noninvasive respiratory support therapies should be considered safe and effective in the proper setting and with experienced teams. A window of opportunity with adequate monitoring should be considered before switching to IMV. Alternating and sequential noninvasive respiratory support therapies could optimise results associated with timely awake proning, in selected patients.
Key points
Rigorous protocols, adequate devices and experienced teams are key to achieve the best results with noninvasive respiratory support therapies in COVID-19-related AHRF.
When using noninvasive respiratory support therapy circuits with antiviral filters, an increase in dead space and patient–ventilator asynchrony may arise and may impact effectiveness.
Using noninvasive respiratory support therapies (especially NIV) in patients with high respiratory effort can induce P-SILI and contribute to worsening ARDS.
Evolution of the disease and patient phenotypes may guide initiation and escalation of noninvasive respiratory support therapies.
Self-evaluation questions
Considering the different noninvasive respiratory therapies in COVID-19-related AHRF, which of the following statement(s) is/are true?
HFT is better than CPAP
NIV may increase the risk of P-SILI
Helmet-NIV does not increase duration of therapy
All noninvasive respiratory support therapies increase aerosolisation of virus
Which clinical assessment tool can be used for prediction of noninvasive respiratory support therapies failure in AHRF?
HACOR and ROX index
SOFA score
HACOR, ROX index and WOB scale
HACOR, ROX index and SOFA score
Prone positioning combined with noninvasive respiratory support therapies:
has no advantages
determines only a transient improvement in oxygenation
reduces the risk of intubation and mortality
reduces the risk of intubation but not mortality
Regarding noninvasive respiratory support therapies in COVID-19-AHRF, which of the following statement(s) is/are true?
Sedation does not improve tolerance to noninvasive respiratory support therapies
HFT is not as well tolerated as CPAP
Oxygen supplementation does not need careful titration
Including a viral filter in the circuit may alter patient–ventilator synchrony
Suggested answers
b.
c.
d.
d.
Footnotes
Conflict of interest: C. Crimi reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from ResMed, Fisher & Paykel, GSK, AstraZeneca and Sanofi, outside the submitted work; C. Crimi is Secretary of ERS Assembly 02.02 on Noninvasive ventilatory support. P. Murphy reports grants or contracts to his institution from Fisher & Paykel, Resmed, Breas Medical, and Philips Respironics, outside the submitted work; consulting fees from Resmed, outside the submitted work; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Philips Respironics, Resmed, Fisher & Paykel, Chiesi, Genzyme, and Breas Medical, outside the submitted work; support for attending meetings and/or travel from Breas Medical, outside the submitted work; and loans of equipment to his institution from Philips Respironics, Resmed, Fisher & Paykel, and Breas Medical, outside the submitted work. M. Patout reports grants or contracts from Fisher & Paykel, Resmed, and Asten Santé, outside the submitted work; consulting fees from Philips Respironics, Resmed, Asten Santé, and GSK, outside the submitted work; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Philips Respironics, Air Liquide Médical, Resmed, Antadir, Fisher & Paykel, Elivie, SOS Oxygène, Loewenstein, Asten Santé, and Chiesi, outside the submitted work; support for attending meetings and/or travel from Asten Santé, outside the submitted work; participation on a Data Safety Monitoring Board or Advisory Board for Resmed, Philips Respironics, and GSK, outside the submitted work; stock or stock options from Kernel Biomedical, outside the submitted work; and receipt of equipment, materials, drugs, medical writing, gifts or other services from Philips Respironics, Resmed, and Fisher & Paykel, outside the submitted work. J. Sayas reports grants or contracts from SEPAR+Philips, outside the submitted work; participation on Advisory Boards for RESMED, and Philips, outside the submitted work; and receipt of equipment from Resmed, Breas, Philips, and Maquet (temporal use of NIV devices for teaching and evaluating purposes), outside the submitted work. J.C. Winck reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Philips Respironics, Sentec, Breas, Vitalaire, and Fisher & Paykel, outside the submitted work; and support for attending meetings and/or travel from Vitalaire, outside the submitted work.
- Received January 24, 2023.
- Accepted April 17, 2023.
- Copyright ©ERS 2023
Breathe articles are open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Description of noninvasive respiratory support therapies
- Noninvasive respiratory support therapies in AHRF: evidence before the COVID-19 pandemic
- Noninvasive respiratory support therapies: an aerosol-generating procedure?
- The issue of patient self-inflicted lung injury and how to make spontaneous effort non-injurious during noninvasive respiratory support therapies
- Monitoring of noninvasive respiratory support therapies in AHRF
- Noninvasive respiratory support therapies trends during the COVID-19 pandemic
- Noninvasive oxygenation strategies algorithm
- Noninvasive respiratory support therapies in COVID-19-related AHRF: important indicators
- Complementary interventions
- Conclusions
- Footnotes
- References
- Figures & Data
- Info & Metrics