





Figures
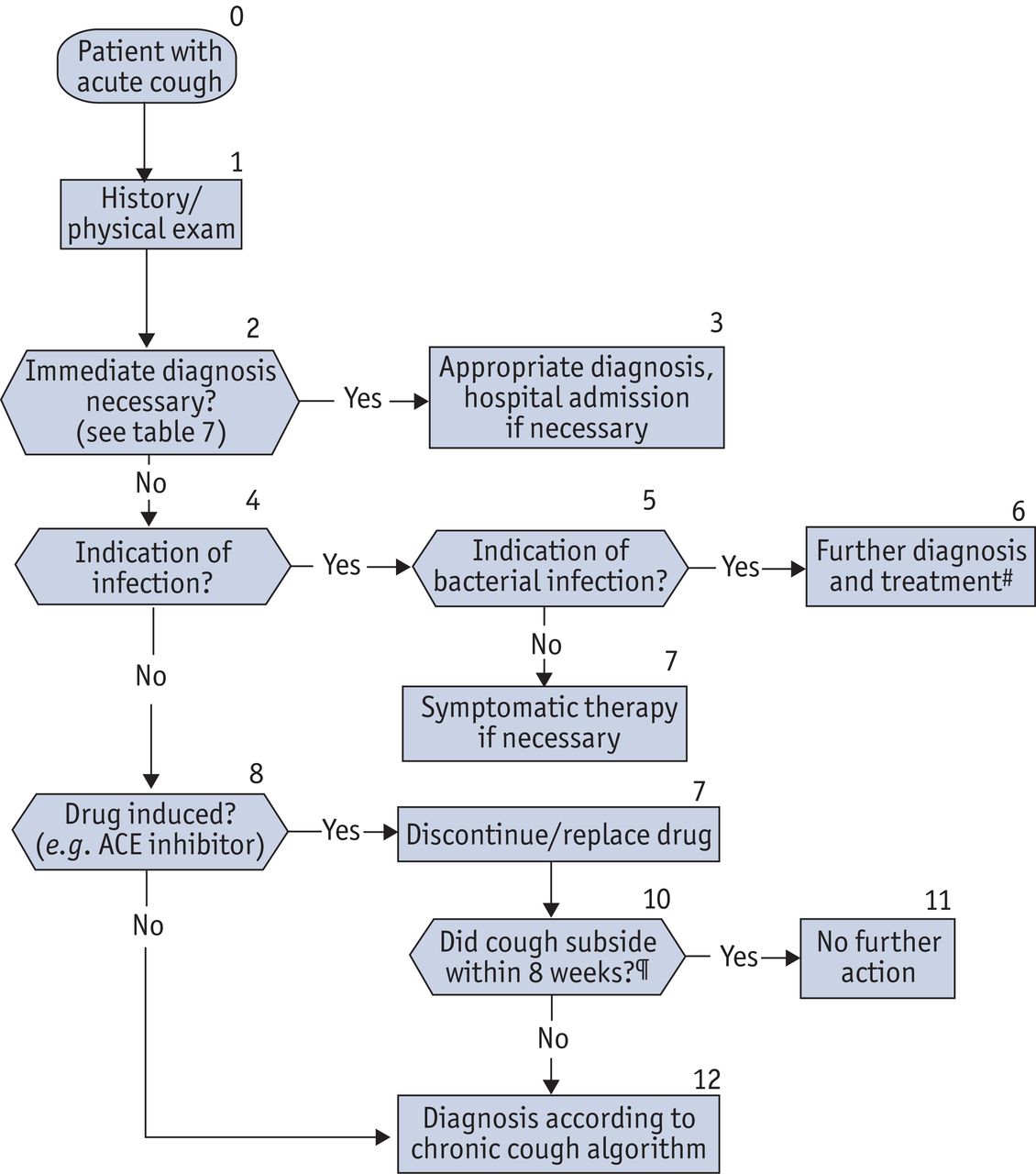
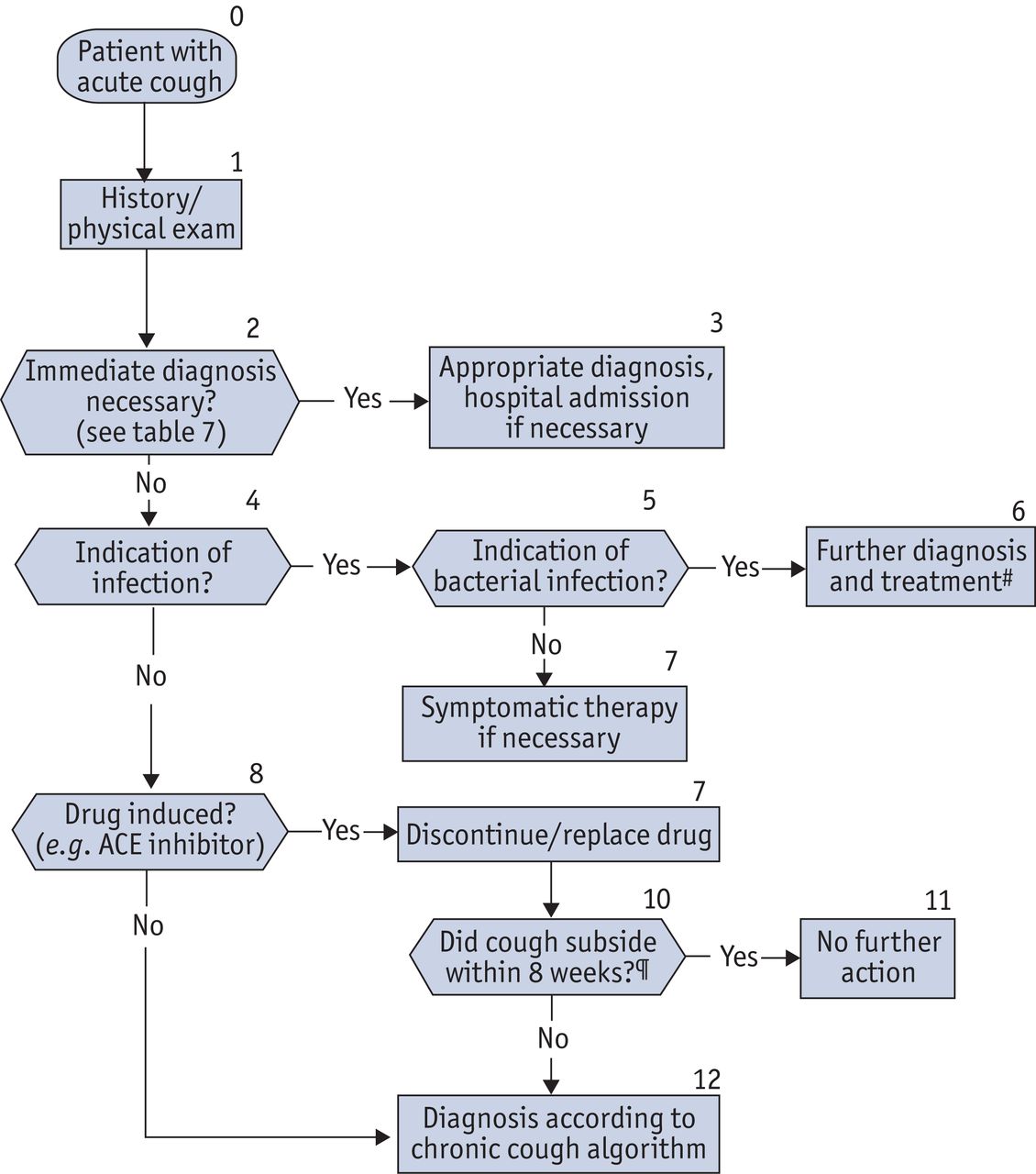
- Figure 1
Clinical algorithm for the diagnosis of acute cough. Cough can persist for ≤8 weeks after an acute infection subsides (post-infectious cough). Except for special circumstances (table 3), further examination according to the algorithm for chronic cough is only necessary after 8 weeks (box 12). #: in otherwise healthy patients, antibiotics are not beneficial even in cases of purulent (green or yellow) sputum [46]; they are only recommended in comorbid or elderly patients with sputum purulence. ¶: caveat is remittent small pulmonary emboli with episodes of remittent cough, palpitations, breathlessness; slight haemoptysis may also occur. Modified from [1] with the publisher’s permission.
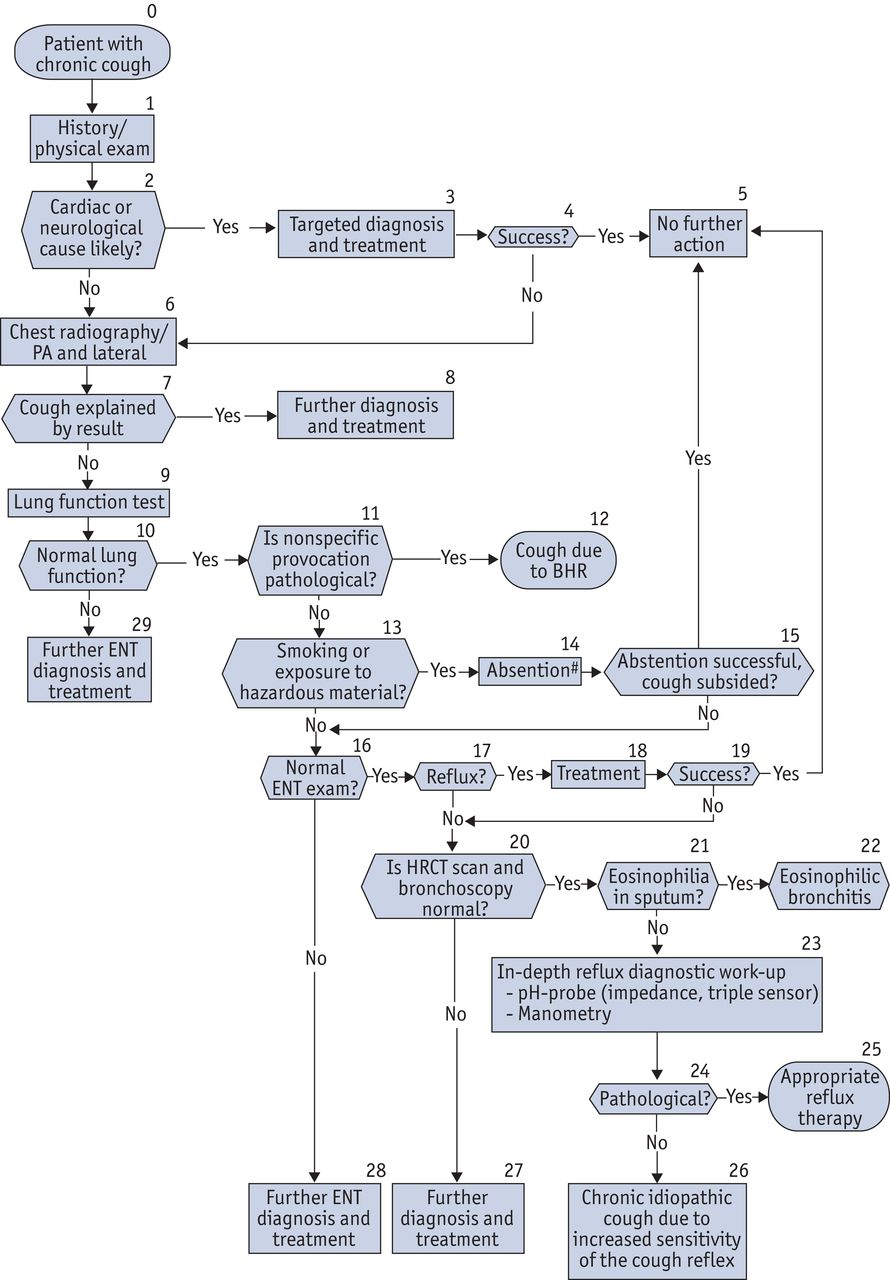
- Figure 2
Clinical algorithm for the diagnosis of chronic cough. Every patient with unexplained chronic cough must have a bronchoscopy performed by the end of the diagnostic algorithm. If a patient complains of cough lasting >8 weeks, diagnostic workup should be initiated immediately. The first steps consist of collecting the patients’ medical history and a physical exam (box 1). If a (primarily) cardiac or neurological cause (e.g. Parkinson syndrome or stroke) of cough is suspected, appropriate diagnostic workup must be initiated (box 3). Establishing the cause of chronic cough is challenging if neither the chest radiograph, nor the lung function test prove conclusive. If bronchial hyperresponsiveness (BHR) can be established by nonspecific inhalative provocation test (box 11), the cough can be treated as probable variant asthma. In smokers with inconclusive chest radiography and normal lung function, smoking-related chronic, nonobstructive bronchitis is the most likely cause of cough. Therefore, a period of smoking cessation is recommended before further diagnostic workup is initiated (box 14). If smoking cessation fails, or abstention remains unsuccessful after 4 weeks, diagnostic workup according to the algorithm should be continued. Provided their chest radiography proves negative, patients with cough and heartburn can be provisionally diagnosed with suspected gastro-oesophageal reflux disease. Proton pump inhibitor (PPI) treatment can commence. In the case of remarkable gastroenterological history, one should proceed according to current gastroenterological recommendations. If, after as long as 3 months high-dose PPI treatment does not resolve the symptoms, continue the algorithm (including high-resolution computed tomography (HRCT) and bronchoscopy; box 20). If the cause of the cough remains unclear, extensive and targeted gastroenterological diagnosis should be performed. This includes endoscopy, oesophageal manometry and triple sensor pH-probe (or impedance for both acid and weakly acid reflux; box 23). At this point, the indication for surgery (fundoplicatio) can be assessed as well. Also, the most commonly missed diagnoses should be considered: early-stage, diffuse parenchymatous lung disease not yet evident on chest radiography, eosinophilic bronchitis (eosinophil cell count in the sputum >3%; box 21) and a psychogenic cough (rare in adults) should all be taken into account. In some patients, the cause of chronic cough will remain unclear despite exhausting the available diagnostic tools. In this case, the patient suffers from chronic idiopathic cough, where the source of an increased sensitivity of the cough reflex cannot be established (box 26). PA: postero-anterior; ENT: ear, nose and throat; HRCT: high-resolution computed tomography. #: based on clinical suspicion, changes in severity and/or characteristics of cough, the patient may require immediate bronchoscopy, thus ignoring the steps of the algorithm. Modified from [1] with the publisher’s permission.
{kind=link}
{kind=link}
Tables
- Table 1 Classification of pulmonary causes of cough
Acute (≤8 weeks) Chronic (>8 weeks) Diseases of the lower airways Diseases of the lower airways and lung parenchyma Asthma Aspiration (commonly children aged 1–3 yrs) Chronic (nonobstructive) bronchitis and COPD Inhalation intoxication (accidents and fire) Asthma and other eosinophilic diseases Post-infectious cough Lung tumours Infectious diseases Diseases of the lungs and pleura DPLD (systemic diseases with diffuse lung involvement) Pneumonia Pleurisy Aspiration and RADS Pulmonary embolism Bronchiectasis and cystic fibrosis Pneumothorax Bronchomalacia Rare, localised disease of the tracheobronchial tree COPD: chronic obstructive pulmonary disease; DPLD: diffuse parencymatous lung diseases; RADS: reactive airways dysfunction syndrome.
- Table 2 Classification of extrapulmonary causes of cough
Acute (≤8 weeks) Chronic (>8 weeks) Diseases of the upper airways Diseases of the upper airways Infectious disease of the upper airways, mostly viral infection (common cold) Chronic rhinitis, sinusitis, pharyngitis and laryngitis Allergic disease Vocal cord dysfunction Cardiac disease with acute pulmonary congestion Obstructive sleep apnoea? Gastro-oesophageal reflux disease Drug-induced cough ACE inhibitors Others Cardiac diseases Any including pulmonary congestion Endocarditis ACE: angiotensin-converting enzyme.
- Table 3 Circumstances requiring an immediate investigation of acute cough
Haemoptysis Severe chest pain Dyspnoea High fever TB Stay in countries with high prevalence of TB Contact with a person stricken with TB Homelessness Illicit drug users Immunosuppressed states Immune deficiency e.g. CVID HIV infection Immunosuppressive therapy History of malignant tumour History of heavy smoking TB: tuberculosis, CVID: common variable immunodeficiency.
- Table 4 Most frequent causes of chronic cough without definite chest radiography or lung function
1 Cough due to upper airway disease 2 Cough-variant asthma 3 Gastro-oesophageal reflux disease (4) (Taking ACE antagonist medication) ACE: angiotensin-converting enzyme.
- Table 5 Chronic or deteriorating cough in patients with diffuse parenchymatous lung disease or autoimmune disease
1 Due to the lung involvement itself (e.g. Sjögren’s syndrome, Wegener’s disease, systemic sclerosis, Churg–Strauss syndrome, idiopathic interstitial pneumonias and sarcoid) 2 Due to the treatment (drug induced cough: methotrexate, cyclophosphamide) 3 Due to infections in the immunocompromised host - Table 6 Rare isolated disease of the tracheobronchial tree
Disease Comments Tracheobronchomegaly (Mounier–Kuhn syndrome) Commonly in male patients Tracheobronchial amyloidal infiltration Local infiltration of the central airways (possibly the larynx) by AL amyloid Relapsing polychondritis Autoimmune inflammatory disease Tracheobronchopathia osteochondroplastica Heterotopic ossification Juvenile recurrent respiratory papillomatosis Adolescents, young adults, casued by human papilloma virus AL: amyloid light chain.
- Table 7 Frequent mistakes in the diagnostic work-up of cough
1 Extensive diagnostic work-up performed in patients taking ACE inhibitors 2 Trivialisation of cough in smokers without diagnostic workup 3 Extrapulmonary causes (ENT, gastric, neurological or cardiac) are disregarded 4 Change of the established sequence of examinations without reason, e.g. performing HRCT before BHR was tested 5 No bronchoscopy though cause of cough was not determined. 6 Multiple causes overlooked 7 Psychogenic cough diagnosed, lung tumour overlooked ACE: angiotensin-converting enzyme; ENT: ear, nose and throat; HRCT: high-resolution computed tomography; BHR: bronchial hyperresponsiveness.










