





Introduction
Indirect challenges to assess bronchial hyperresponsiveness are being increasingly used both for research and for assessment in the routine pulmonary function laboratory. “Indirect challenges act by causing the release of endogenous mediators that cause the airway smooth muscle to contract with or without inducing microvascular leakage. Because the responses to these challenges are modified or completely inhibited by inhaled steroids, the airway response to the challenges may be a closer reflection of active airway inflammation” (fig. 1) [1]. In contrast, the direct tests, inhaled aerosols of histamine and methacholine act directly on receptors on the bronchial smooth muscle to cause contraction. While sensitive for detecting bronchial hyperresponsiveness a positive response to these agents is not specific for identifying asthma particularly at the higher concentrations. The best known of the indirect challenges is exercise. Other indirect challenges include eucapnic voluntary hyperpnoea, mannitol, adenosine monophosphate and hyperosmolar saline. All these indirect challenges are associated with release of mediators of bronchoconstriction. For this reason they have the potential to be used to identify presence of inflammatory cells particularly mast cells [2].

The events that lead to airway narrowing and a reduction in forced expiratory volume in 1 s in response to different indirect challenge tests. While hyperpnoea, mannitol and 4.5% saline all act to increase osmolarity that causes mediators to be released, adenosine acts to release mast cell mediators through a specific receptor on the mast cell. ASL: airway surface liquid; FEV1: forced expiratory volume in 1 s. Modified from [2] with permission from the publisher.
Exercise
Usefulness
Exercise testing is used to diagnose exercise-induced bronchoconstriction (EIB). The term EIB describes the transient increase in airways resistance that follows vigorous exercise. EIB is thought to result from transient dehydration of the airway surface in response to conditioning the inspired air. The diagnosis of EIB is made on measurement of changes in lung function in response to exercise. The type, duration and intensity of exercise and the water content of the air inspired and the time since EIB was last provoked are important factors when identifying EIB and its severity [3, 4].
Objective testing with exercise for EIB is clinically very useful because the symptoms often associated with vigorous exercise are similar to those reported by asthmatics. Importantly healthy people without EIB can have these “asthma” symptoms and those with EIB may not have these symptoms. Clinically, having a properly performed exercise test to identify EIB avoids both the over diagnosis and under diagnosis of EIB when symptoms are relied upon to make the diagnosis. In addition it is important to have objective evidence of EIB for people seeking occupations (defence, police) or for recreation (diving) where EIB would not be desirable.
EIB is identified by documenting a fall in forced expiratory volume in 1 s (FEV1) of 10% (or 15%) or more from the pre-exercise value within 20–30 mins after exercise [3, 5, 6]. The lowest values are usually measured within 5–12 mins. The FEV1 is measured two or three times at various time intervals after exercise for example, 1, 3, 5, 10, 15, 20, 30 minutes and the highest of the acceptable values (using ERS/ATS criteria) is recorded at each interval [3, 4]. Recovery from EIB is spontaneous and FEV1 usually returns to 95% of the baseline value within 30–60 mins.
Availability
The availability to perform vigorous exercise is relatively easy outside the laboratory. Exercising in the field performing the same exercise routine that produces the subject’s symptoms is very useful. The ready availability of hand-held spirometers has made testing in the field easier than ever before. While peak expiratory flow (PEF) was once commonly used for identifying EIB it is not as repeatable as FEV1 and is no longer recommended. In very young children measurement of FEV0.5 can be useful [7]. Field testing with sports specific exercise for athletes usually means performing the actual sport for as long as it takes to provoke the symptoms. This period may be as short as a few minutes for ice skating or as long as 20–30 mins for cross-country skiing [8]. Field testing performing running exercise has been used for evaluating school children for EIB [6].
The ability to perform vigorous exercise in the laboratory is dependent on the availability of suitable ergometers. Whilst exercise equipment is frequently available in lung function laboratories, the choice of ergometers is usually limited to treadmill and bicycle. It may not be informative to run or to cycle a subject who has their symptoms whilst rowing or swimming or skiing. However, it is usually easier to have the right inspired air conditions during exercise in a laboratory as most have available medical grade air that is dry. Finally, the appropriate equipment for measuring the intensity of exercise, i.e. by measuring ventilation (rather than heart rate), is more readily available in a laboratory and even some simple household gas meters can be used for this purpose. All laboratories performing bronchial provocation tests would be expected to have the appropriate spirometers and safety equipment, and personnel readily available for resuscitation.
Limitations
The limitation to field exercise is having the right equipment that includes a spirometer, a measure of exercise intensity such as a heart rate meter, a nose-clip for exercise, safety equipment and the ability to measure temperature and humidity to ensure that the water content is <10 mg of water per litre of air. This represents ∼50% humidity at 23°C [6]. At temperatures <10oC the air will always be sufficiently dry. As severe falls in FEV1 can occur it is important to have available a bronchodilator, oxygen and a hand-held pulse oximeter.
The greatest limitation to exercise testing for EIB in the laboratory is the wide variety of exercise protocols that are used, some of which are simply inadequate to provoke EIB. Most laboratories report a low prevalence of positive tests for EIB and this is the major reason for the switch to using other tests. The exercise required to diagnose EIB is not suited to a continuous increase in intensity and it is necessary to reach the maximum work load rapidly within a few minutes and lower the load later if needed. Starting with very a low work-load or using the classic progressive exercise protocols for assessing maximum working capacity will lead to many false negative results. The reason probably relates to release of broncho-dilating substances, such as prostaglandin E2, at low ventilation that serve to protect the airways from bronchoconstriction.
To avoid false negative tests and give the greatest likelihood to identify EIB, the intensity of exercise needs to be sufficient to raise the ventilation and heart rate close to the desired value within the first 2–3 min of exercise. This intensity needs to be maintained for ≥4 mins in children and 5 or 6 mins in adults. This is usually easier to achieve by running on a treadmill than cycling. Specific protocols for guidance are published [6, 8–12] and two examples of these are summarised in tables 1 and 2. Some of these protocols involve running while others involve cycling or involve exercise in the field. In brief, the study protocols recommend breathing dry air with a nose clip in place while running or cycling at a ventilation to reach ∼17.5–21 times FEV1 during the first 2–3 mins of exercise or a load sufficient to raise the heart rate to 80–90% of predicted maximum (∼220 - age in yrs). Severity of EIB for an individual is dependent on rate of water lost from the lower airways which is why ventilation is the primary determinant of EIB and why the inspired air needs to be dry. The higher the ventilation, the dryer the air the greater the number of airways recruited into the conditioning process and the greater the chance of identifying EIB [13, 14].
There are many factors, other than intensity and duration of exercise, that can affect the response to exercise. These include, recent intake of asthma medications, recent or intermittent warm up exercise and all increase the likelihood of a false negative. In contrast recent exposure to inhaled or ingested allergens may increase the severity of the response the subject may normally have. Furthermore, there is inherent variability in EIB (25–50% variation in the % fall) such that a diagnosis of EIB may be “missed” if only one test is performed (fig. 2) [10]. Exercise is thus not the best laboratory test for identifying potential for EIB in the field or to identify the bronchial hyperresponsiveness of asthma.

Response to two identical exercise tests (T1 and T2) in 278 adults and 95 children with signs and symptoms of asthma but no definite diagnosis. Note that for 89 subjects, the exercise test was positive on only one of the two tests. For 44 subjects, the negative test was the first one and thus on one test exercise-induced bronchoconstriction would have been missed. FEV1: forced expiratory volume in 1 s Modified from [10] under creative commons.
Eucapnic voluntary hyperpnoea
Usefulness
The many variables that need attending in order to minimise the likelihood of a false negative test and the safety issues related to exercise testing itself led to the development and use of the eucapnic voluntary hyperpnoea (EVH) test [15, 16]. This test is also known as eucapnic hyperventilation or isocapnic hyperventilation. There are advantages in using EVH in the laboratory. The EVH test requires less equipment and fewer personnel and it is quieter and less stressful to perform than exercise at the equivalent level of ventilation. The duration of the ventilation and the condition of the air inspired can be varied if required to evaluate the conditions under which exercise is performed i.e. cold air etc. An abnormal response is a ≥10% fall in FEV1 from the baseline value and it is recommended that the fall be sustained for two consecutive readings over 5 mins after completion of the hyperpnoea.
EVH is the most useful test to identify EIB in athletes [17, 18] and defence force recruits [15] with normal lung function. For this application the standard protocol of 6 mins of a target ventilation of 30-times FEV1 is more sensitive than laboratory-based exercise tests and the frequency of false negative test results is low [19, 20]. This standardised protocol is not recommended for identifying EIB in known asthmatics who are symptomatic or uncontrolled or whose lung function is not normal. The clinical utility of using a lower ventilation (21-times FEV1 for 6 mins) has been reported in patients referred for routine testing for EIB and was diagnostic in 81% of subjects. The clinical usefulness of testing with EVH is in reducing the over- and under-diagnosis of EIB that arises from relying on symptoms.
Availability
Although EVH for 4 mins with cold air was frequently performed in laboratories in the early 1980s [21], today EVH is mostly used to test elite athletes [22–26]. The reason for this change may have related to the perceived need to cool the air and the definite requirement to control the end-tidal carbon dioxide in order to maintain eucapnia over a wide range of ventilation. Both of these needs added to the cost of the test. The technical issues, but not the cost issue, have in part been overcome by using a commercially prepared gas mixture of 4.9–5% CO2, 21% O2 and balanced N2 inhaled at room temperature for 6 mins. Under these conditions, eucapnia is maintained at ventilations between 40 and 105 L·min−1 [27]. Machines are commercially available to mix gases.
Limitations
The major limitation in using the EVH tests is the need to maintain eucapnia over a wide range of ventilation. The FEV1 needs to be ≥1.5 L and ventilation needs to be 40–105 L·min−1 to use the prepared gas mixture. If the FEV1 value is lower or the ventilation is outside the limits, then the endtidal CO2 needs to be monitored for eucapnia. This is important because hypocapnia is a bronchoconstricting stimulus in itself and hypercapnia is dangerous because it produces acidosis.
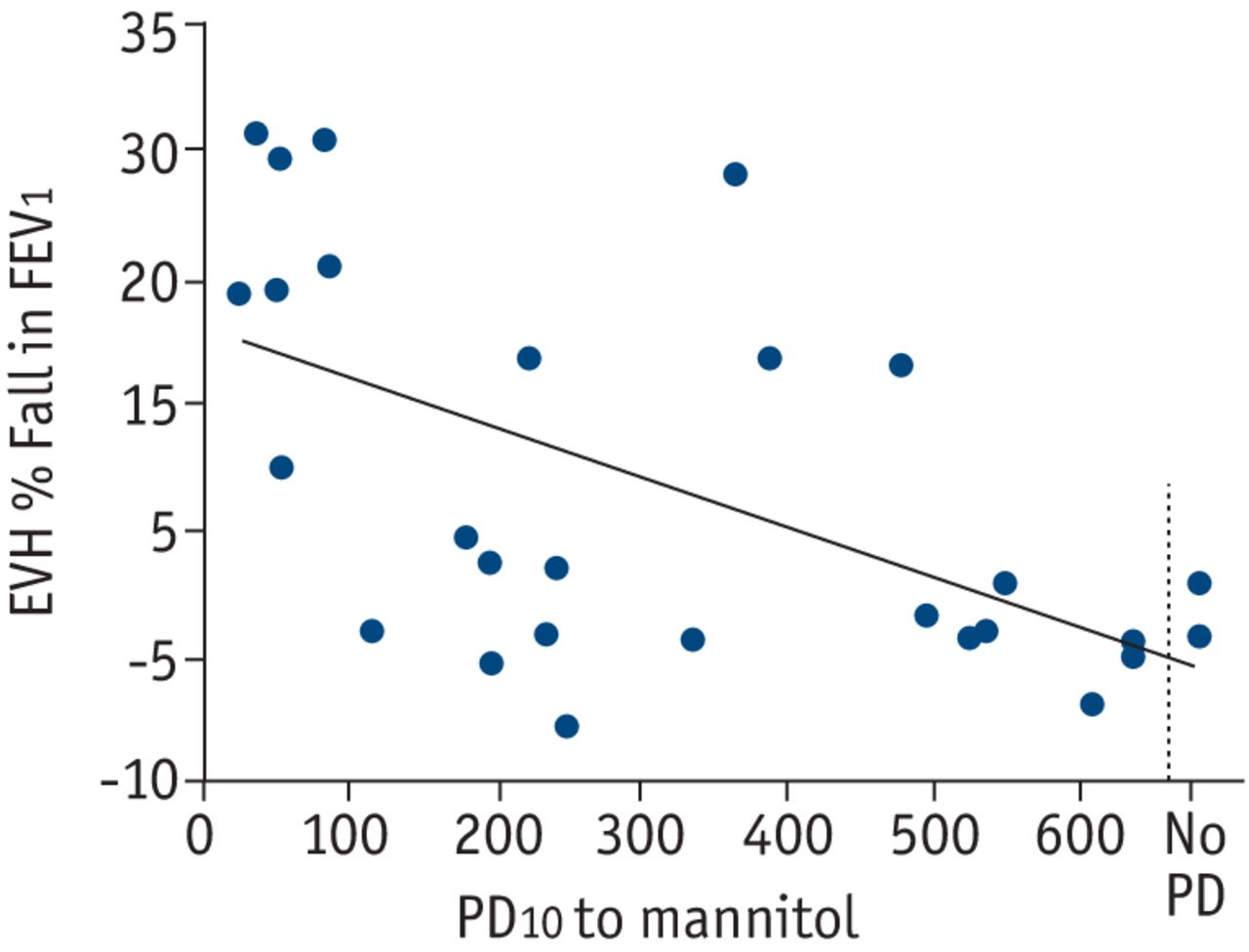
A second limitation is the potential to induce rapid and severe (>30%) fall in FEV1 postchallenge (fig. 3) [28]. The EVH test uses one level of ventilation for 6 mins and, as with exercise, the bronchoconstriction rapidly follows cessation of the hyperpnoea. For this reason, the original standardised protocol of 30-times FEV1 for 6 mins is only appropriate for identifying EIB who perform exercise regularly and at high intensity and is not the test of choice in known asthmatics. If EVH is the only test available then ventilation of 21-times FEV1 rather than 30-times FEV1 is recommended [29, 30] and consideration should be given to shortening the duration to 4 mins rather than 6 mins. This lower level of ventilation is equivalent to 60% of maximum voluntary ventilation and is similar to what would be reached during intense exercise in the average healthy athletically untrained person [9].

% decrease in forced expiratory volume in 1 s (FEV1) to eucapnic hyperpnoea (EVH) in relation to the provoking dose to cause a 10% fall in FEV1 after mannitol inhalation (PD10) in elite athletes. Note the high % fall in FEV1 after EVH in some subjects. Modified from [28] with permission from the publisher.
There is a report that the EVH is uncomfortable to perform [24]. There may be several reasons for this. First, because the ventilation needs to be very high, the resistance of the equipment needs to be very low. If there is just one part of the apparatus that is too narrow, the resistance will increase and it will be difficult for the subject to inhale at the high flow rates required. Secondly, the dry air is difficult for some subjects who may be troubled by cough. Finally, for athletes with an FEV1 greater than normal, the target ventilation of 30-times FEV1 may simply be too high and should be reduced to a comfortable level that still exceeds 21-times FEV1.
Dry powder mannitol
Usefulness
Mannitol is highly specific for identifying the bronchial hyperresponsiveness that is consistent with asthma. In well-defined groups there are few false-positive test results [31–34]. As with other indirect challenges, mannitol does not cause the bronchial smooth muscle to contract directly, as inhalation of histamine or methacholine do, but rather, it acts indirectly on inflammatory cells (most likely the mast cell) to induce release of mediators, such as prostaglandin D2, leukotriene E4 and histamine. In those with hyperresponsiveness, bronchial smooth muscle exposure to these mediators will stimulate specific receptors on the muscle causing it to contract and the airways to narrow [35]. Thus, in addition to a hyperresponsive muscle, a positive response to mannitol indicates that there are sufficient numbers of inflammatory cells, with a sufficient concentration of mediator to cause airway narrowing. In a person negative to mannitol one or more of these three components will be missing. It is important to remember that most stimuli that provoke an attack of asthma in daily life act indirectly. Normal variation in cell numbers, concentration of mediators and responsiveness of the muscle mean that the airway responses will vary over time and in response to treatment with anti-inflammatory agents.
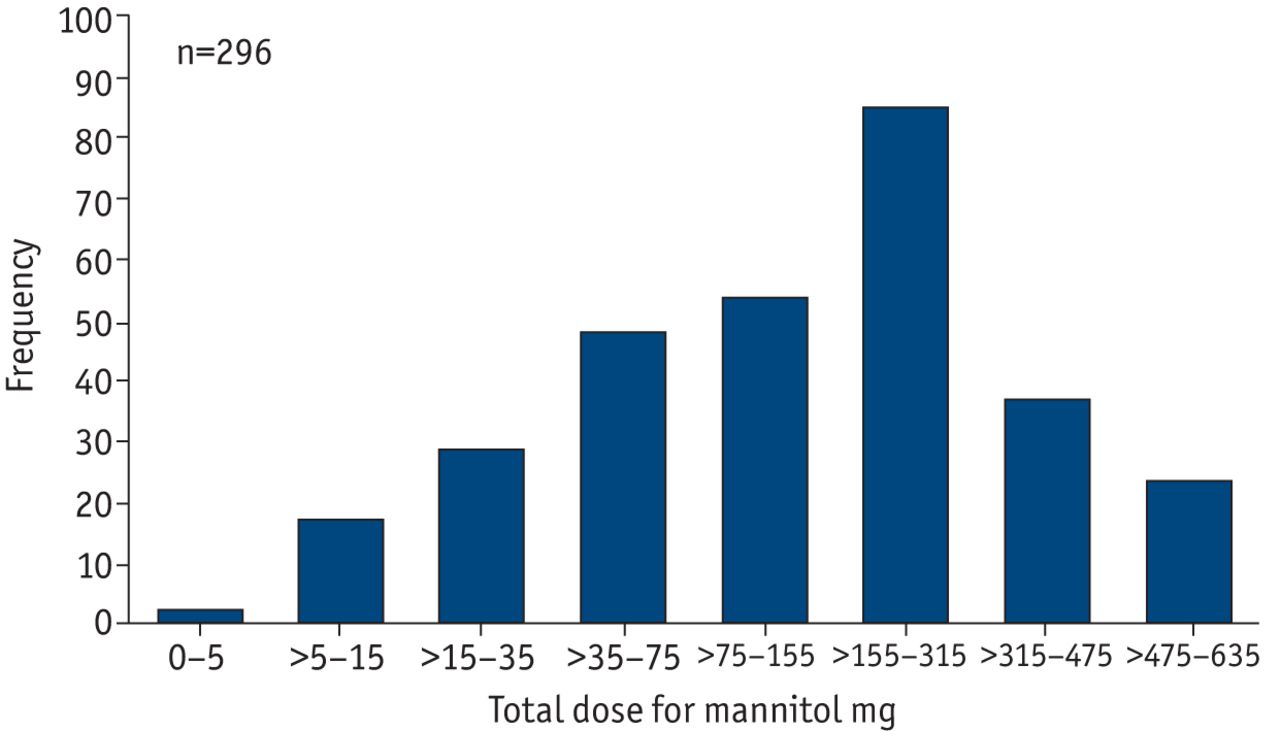
Mannitol was chosen as an osmotic stimulus because it is stable as a dry powder at high relative humidity, has many medical applications and is generally regarded as a safe molecule. The mannitol inhalation test has one standard protocol and dry powder device for delivery. The FEV1 is measured 60 s after each dose of mannitol (0, 5, 10, 20, 40, 80, 160, 160, 160 mg). The dose of 80 and 160 mg are given as multiples of 40 mg capsules. The subject is asked to exhale completely before taking a controlled deep inspiration from the device (flow rate best kept at 60–90 L·min−1) and to hold their breath for 5 s then exhale through their mouth before removal of the nose clip. The test result is expressed as the provoking dose to induce a 15% fall in FEV1 (PD15). The 15% cut-off point from the post 0 mg capsule is based on the mean % fall in FEV1 plus 2 standard deviations documented in healthy non-asthmatic subjects (fig. 4) [31, 36]. PD15 is a measure of sensitivity. In phase-3 trials, 80% of subjects with a positive response to mannitol responded after 10 capsules or six dose steps (fig. 5) [31].

The values for the provoking dose of mannitol to cause a 15% decrease (PD15) in forced expiratory volume in 1 s (FEV1) showing the different levels of bronchial hyperresponsiveness to mannitol and the values obtained in normal healthy subjects. Modified from [36] with permission from the publisher.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The number of asthmatic subjects, with a 15% decrease in forced expiratory volume in 1 s to mannitol at each dose interval, in the initial Phase 3 trial [31]. Note that 80% of the 296 subjects responded with a positive test result with a cumulative provoking dose of mannitol less than 315 mg or 10 capsules. Modified from [31] under creative commons.
The progressive nature of the protocol for the mannitol test to achieve a 15% fall in FEV1 means that the large falls in FEV1 often observed with exercise and EVH are avoided. The mean final fall in FEV1 is ∼21% [31, 37]. Recovery of FEV1 is spontaneous and the median time to recovery to 95% baseline value is reported as 21.6 mins. The response–dose ratio (RDR) is a measure of reactivity and is defined as the % fall in FEV1 per mg of mannitol. RDR have been used to compare responses to exercise and for diagnosis of asthma [32, 38].
The reported mean time for a positive mannitol test is <18 mins and for a negative test is <27 mins [31]. Repeatability of the test is ±1.0 doubling dose in adults and children [39, 40]. The mannitol test kit using dry powder has overcome many of the technical and hygiene issues related to the use of wet aerosols for bronchial provocation and collection of sputum [41, 42].
Availability
Bronchial provocation tests using dry powder mannitol, known as AridolTM or OsmohaleTM, have been approved by regulatory authorities in Europe, Asia, Australia and the USA and are available in 23 countries. The mannitol test comes in a kit, containing prepacked capsules and an inhaler device.
Limitations
As with any osmotic challenge, inhalation of mannitol will provoke a person to cough. The large phase-3 trials of 592 people reported that 85% of subjects experienced cough [31]. The majority (71%) of the subjects had only occasional cough that did not delay the administration of the next dose. For 13.2% of subjects however there was some delay to the next dose. In only 1.3 % of subjects was the challenge stopped for cough. Other adverse events on the day of study included pharyngeal pain (2.6%), throat irritation (1.1%), and nausea (1.1%). The first two are alleviated by sips of water during challenge [31].
The rationale for inhaling mannitol as a surrogate for exercise to identify EIB is based on the stimulus i.e. increasing osmolarity of the airway surface liquid to mimic dehydration and the mechanism for bronchoconstriction i.e. via inflammatory mediators being common to both. In those with clinically recognised asthma, not taking inhaled steroids, the sensitivity for mannitol to identify EIB provoked by exercise or EVH is high and the severity of airway narrowing can be predicted from the PD15 to mannitol [28, 43, 44]. The relationship is not as clear for people with signs of asthma without a definite diagnosis [37, 45]. In one study, 30% with EIB (>15% fall in FEV1) were not identified either with mannitol or with methacholine [37]. However, in the same study, the frequency of bronchial hyperresponsiveness to mannitol, defined as a 15% fall in FEV1, was 1.6-times that found with a single exercise test. Similar results were recently reported in 99 children referred for possible diagnosis of asthma with 21 positive to exercise and 29 to mannitol with a test agreement of 84% [45]. A similarly high frequency of responsiveness to mannitol (92%) with a lower response to exercise (36%) has also been reported by others [46].
The response to mannitol is dependent on progressively increasing an osmotic gradient. To achieve this, the subject needs to inhale each dose of mannitol as quickly as possible after the last dose. The sensitivity of mannitol to identify EIB is greater when the test time is <35 mins [37] and for optimal use the test should be no greater than 35 mins for the full 635 mg.
Conclusion
Exercise testing in the laboratory, to identify EIB has limited clinical utility. The reason is that it is hard to control the many factors that affect the severity of the airway response and, as a result, there is great variability and a high rate of false negative test results. Many of these factors were overcome by the development of the eucapnic voluntary hyperpnoea test and this is considered the best test to identify EIB in the laboratory. The reason is that EVH requires breathing dry air at a ventilation rate beyond the maximum achievable by most people, during exercise so the occurrence of false-negative tests is minimised. As EVH provides a potent stimulus and large falls in FEV1 can occur, the test is most appropriately used to identify EIB in subjects with normal lung function who perform exercise regularly and at high intensity. The response to both exercise and EVH is reported as maximum % fall in FEV1 which is a measure of reactivity. Dry powder mannitol, delivered by inhalation as an aerosol, provides a similar stimulus to the airways, as exercise and EVH, in that the same inflammatory mediators are released in response to the challenge. Challenge with mannitol differs from exercise and EVH in that the airway response is measured after each dose, a technique that avoids large falls in FEV1. With mannitol, both sensitivity (PD15) and reactivity (RDR) are measured. The same mannitol test kit and inhaler device has regulatory approval in four continents. The standardised protocol and published data on safety and efficacy in large numbers of subjects give mannitol the opportunity to become the “gold standard” over other indirect challenge tests (exercise, eucapnic voluntary hyperpnoea, adenosine monophosphate, hyperosmolar saline) for identifying bronchial hyperresponsiveness and the potential for EIB in the routine laboratory.
Footnotes
This article is based on a post-graduate course from the Barcelona 2010 ERS Annual Congress
Competing interests
S.D. Anderson is the inventor of the mannitol test that is used for bronchial challenge testing. The intellectual property (IP) is owned by her employer, Sydney South West Area Health Service (SSWAHS), which licensed the IP to Pharmaxis Ltd in 2001. S.D. Anderson purchased shares with her own money at the time the company went public in 2003. She owns 30,000 shares and holds no options. SSWAHS receives royalties for sales of the mannitol test (Aridol and Osmohale). S.D. Anderson receives a 10% share of the royalties paid to SSWAHS. S.D. Anderson’s department at Royal Prince Alfred Hospital received money for Phase 3 trials for the mannitol that contributed to the registration of the mannitol test with the regulatory authorities. The same department now receives 30% of the royalties paid to SSWAHS. Since leaving full-time employment in March 2009, S.D. Anderson acted as a paid consultant from time to time for Pharmaxis Ltd. She also gives lectures for Pharmaxis Ltd and its distributors, for which she has received honoraria. She has no other conflict of interest.
- ©ERS 2011
References










