





Introduction
In the previous two issues of Breathe, the case of a 6-yr-old boy who had been admitted to the paediatric department of the University of Heraklion has been covered. After treatment, he was discharged in excellent condition.
12 months later, the boy was readmitted to the hospital for gradually increasing productive cough for 9 days and fever (up to 39.5°C) for 3 days.
He was in good condition. His blood temperature was 38°C, respiratory rate was 24 breaths·min−1, heart rate was 120 beats·min−1 and O2 saturation was 91%. On chest auscultation he had decreased breath sounds over the right lower hemithorax. Cardiac examination was normal, throat examination showed small exudates on tonsils and review of remaining systems was normal.
Chest radiograph (CXR) is shown in figure 1.

Task 1
How would you interpret this CXR?
Answer 1
The posteroanterior (left) and lateral (right) CXRs show opacification/consolidation of the right lower and middle lung lobes. There was blunting of the right costophrenic angle with small fluid collection. Right hemidiaphragm was not seen (positive “silhouette” sign).
Blood test results are shown in table 1. Chemistry lab tests were normal and blood cultures were sent.
Task 2
What is your diagnosis?
Answer 2
Bacterial or viral pneumonia.
Due to symptoms, radiographic findings, leukocytosis with increased neutrophils, ESR and CRP the diagnosis of bacterial pneumonia was made. The patient was treated with intravenous ampicillin–sulbactam 150 mg·kg−1·day−1, oral clarithromycin (1 g·day−1) and inhaled bronchodilators. Chest auscultation revealed wet crackles which were gradually diminished to normal breath sound. Fever subsided on the 4th day. Intravenous antibiotics were given for 10 days.
Repeat lab tests are shown in table 2. Blood cultures were negative. Cold agglutinins for mycoplasma and pneumococcus antigen in the urine were negative. Stain of sputum showed increased white cells. Sputum culture was negative.
Repeat CXR 10 days later is shown in figure 2.

Task 3
How would you interpret the CXR?
Answer 3
The CXR shows normal chest.
The patient was discharged. A sweat test was performed to rule out cystic fibrosis and a return appointment within a week was scheduled. In case of recurrence of symptoms, bronchoscopy and test for primary ciliary dyskinesia (PCK) would be performed.
Results of lab tests showed: Μycoplasma pneumoniae immunoglobulin (Ig)G: 14.9 (positive); IgM: 7.6 (negative); Chlamydia pneumoniae IgG and IgM: negative; Ricketsia Conorii IgG and IgM: negative; IgG: 1,230 mg·dL−1 (normal); IgM: 128 mg·dL−1 (normal); IgA: 140 mg·dL−1 (normal); serum complement C3c: 189 mg·dL−1 (increased); serum complement C4: 32 mg·dL−1 (normal); IgE: 16.2 IU·mL−1 (normal). RAST results were pending and sweat test was negative.
The patient was referred to the Pediatric Allergy Pulmonary Outpatient Clinic. Detailed history revealed that he had frequent cough episodes attributed to viral colds. He was treated for a short time with inhaled steroids and salbutamol unsuccessfully. In the past, he was evaluated for nasal symptoms and was diagnosed with allergic rhinitis. He was given antihistamines on a pro re nata basis.
His mother reported allergic skin rashes and positive RAST to olive tree pollen. A parental cousin had frequent bronchitis episodes until the age of 14 yrs. Parental grandfather has chronic obstructive pulmonary disease. The patient had a cat at home and was exposed to dogs, chicken, pigeons, a pheasant and a peacock in his grandparents’ environment.
On physical examination the patient appeared well; he had normal chest auscultation, no clubbing and the rest of the examination was normal.
RAST results to known allergens (house dust mites, olive pollen, parietaria, grass mix, mold mix, H1 and H2) were negative. RAST to cat, dog, chicken, pigeons and peacock were ordered.
Task 4
Would you now order: 1) CXR; 2) chest computed tomography (CT); 3) spirometry; 4) metacholine test; or 5) bronchoscopy.
Answer 4
-
CXR is not needed now, since there are no symptoms since last discharge.
-
Chest CT is not needed, for the same reason.
-
Spirometry, before and after bronchodilator, is indicated due to the history of bronchitis and of three admissions for recurrent pneumonia.
-
Metacholine test is not indicated before spirometry is performed.
-
Bronchoscopy is indicated due to the history of recurrent pneumonias in the same lobe/region. This procedure can detect dynamic airway collapse, can reach distal regions and can obtain samples from airways or alveolar spaces for culture and cytologic examination; however, bronchoscopy should not be done before noninvasive methods fail to identify the cause of recurrent symptoms.
Spirometry before and after bronchodilator is shown in figure 3.

Spirometry before and after bronchodilator
Task 5
What do the spirometry data suggest and can you propose a diagnosis?
Answer 5
Flows (maximum midexpiratory flow (MMEF) and forced expiratory flow between 25 and 75% of forced vital capacity (FEF25–75)) show a degree of obstruction, which is not reversed after bronchodilators. Peak expiratory flow (PEF) showed a reversibility of 18.5%. Despite the lack of reversibility of forced expiratory volume in 1 s (FEV1) and given that spirometry is not a sensitive test, particularly in children, the diagnosis of asthma was considered based to the patient’s history and CXR findings.
The patient was given inhaled steroids, long acting β2 agonists for 1 month and was asked to record his daily symptoms.
1 month later, the patient’s diary showed cough induced by exercise, crying, intense odours and occasional nasal congestion. His IgE was normal, his additional RAST results were negative. A sinus radiograph showed sinusitis. He was prescribed antibiotics and nasal corticosteroids for sinusitis. He was asked to continue his asthma treatment for 2 months and return for assessment. At his next visit, he had improved but was still experiencing some symptoms. An anti-leukotriene receptor antagonist was added to the treatment and, with this adjustment, the patient was entirely asymptomatic. He would only experience exercise-induced cough when he forgot his medication.
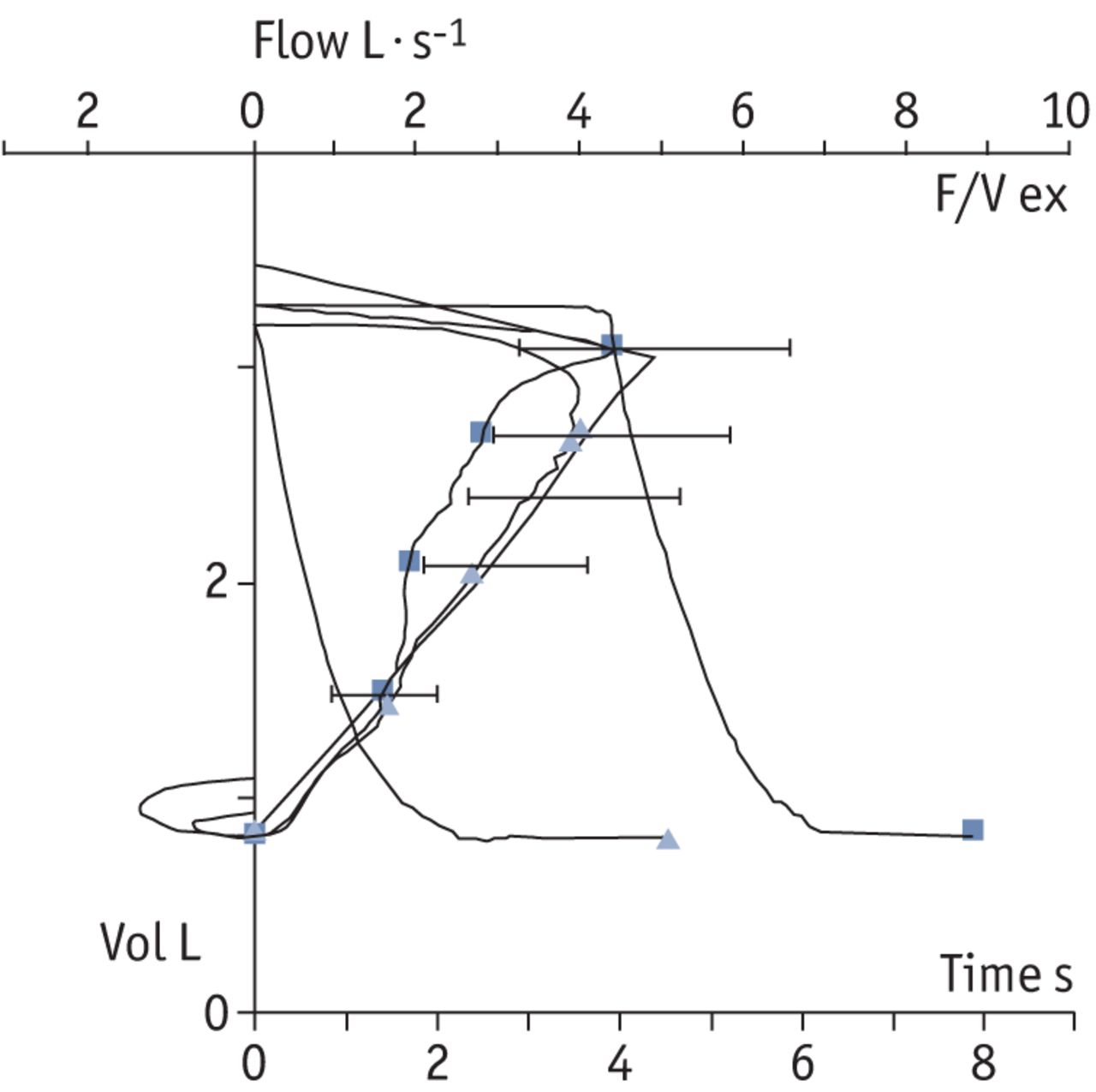
Repeat spirometry, performed 1 yr later, is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Repeat spirometry
Task 6
What do the spirometry data and flow–volume curve suggest?
Answer 6
Mild-to-moderate obstruction of small airways. Reversibility of MMEF, FEF25, FEF50 and FEV0.5 after bronchodilators suggestive of mild-to-moderate asthma.
Discussion
This report describes a child with three episodes of pneumonia. The patient meets the criteria for recurrent pneumonia (RP) which is defined as ≥2 episodes in a single year or ≥3 episodes ever, with clearing of x-ray densities between episodes [1]. Recurrent pneumonia occurs in 7.7–9% of all children with pneumonia [2–5].
The aetiology of RP varies depending upon the location of pneumonia, which can involve a single or various lobes or lung regions. This patient’s three episodes of pneumonia occurred in the same lung region.
Recurrent pneumonia involving a single lobe or segment, is caused by localised pathology, such as local compression, malformation or inflammation, whereas, pneumonias affecting more than one lobe, suggest a more generalised abnormality, such as mucociliary clearance dysfunction, aspiration, immunodeficiency or asthma. The patient’s recurrent infiltrates occurred in right middle and right lower lobe.
Recurrent pneumonia and atelectasis of the right middle lobe make up a unique entity known as “right middle lobe syndrome”. This lobe is prone to infection and collapse because the bronchus arises from the bronchus intermedius at an acute angle and is relatively long before it subdivides into segments [6]. Furthermore, there is no collateral ventilation between the right middle lobe and other lobes [7]. The most common noninfectious cause of right middle lobe syndrome is asthma [8]; the most common infectious cause is tuberculosis.
We considered that the patient may have asthma because his abnormal chest radiographs were similar, affecting the right middle and right lower lobe, all of his three episodes happened during spring, he had history of allergic rhinitis and of recurrent bronchitis. The latter may mask asthma [9].
Several studies have shown association between RP and asthma. Older children with asthma may develop recurrent chest infiltrates/pneumonias [3, 4, 10]. In a study of 125 asthmatic children, 14 of them experienced 70 episodes of recurrent pneumonia [11]. Moreover, undiagnosed or uncontrolled asthma was diagnosed ≤80% of children evaluated for recurrent pneumonia [12], which can also be the initial manifestation of asthma [8].
Chest radiograph densities, shown during asthma exacerbations, may be due to infections, atelectasis or both [6, 13, 14]. The patient’s recurrent chest radiograph densities could represent asthma exacerbations and could be due to infections or atelectasis or both. Fast clearing of his radiographic findings, within a week, documented during hospitalisations, was favouring atelectasis rather than pneumonia.
The rate of resolution of infiltrates caused by viruses or bacteria is longer that one week; it ranges between 2–3 weeks for respiratory syncytial virus, 6–8 weeks for pneumococcus [15], or ≤12 months for adenovirus [16].
Asthma exacerbations are frequently triggered by acute viral respiratory infections [12, 17, 18] which may present with fever, increased mucus secretions, plugging of bronchi, atelectasis or occasionally with secondary bacterial infection. However, in some patients mucus induced atelectasis, without infection, can cause recurrent chest infiltrates, dyspnoea and fever [10] similar to the symptoms of our patient.
In the hospital, the patient was diagnosed with bacterial pneumonia due to fever, respiratory symptoms, the CXR report of “consolidation” and the increased values of white blood cells, polymorphonuclear neutrophils, erythrocyte sedimentation rate and C-reactive protein suggesting bacterial infection. Accordingly, he received antibiotics and asthma medication, due to previous bronchitis, and the laboratory indices improved. Paediatricians tend to treat a nonwheezing child with antibiotics if the radiograph report states “focal airspace consolidation” or “focal infiltrate” [19]. It is unclear whether atelectasis alone without infection could cause laboratory indices mimicking bacterial infection and whether these indices would improve without antibiotics.
At the specialty clinic, we attributed the patient’s symptoms and chronic cough, triggered by viral stimuli, to bronchial hyper-reactivity caused by asthma. The initial spirometry, however, did not show reversibility, despite the presence of CXR infiltrates, possibly representing inflammation. A study of young adults with mild-to-moderate asthma, showed that only 36% had positive spirometry suggesting asthma, while 59% had negative spirometry, but positive radiograph showing “increased markings” representing inflammation [20]. A negative spirometry test does not exclude the diagnosis of asthma in children [6].
If spirometry is normal, a metacholine test to detect bronchial hyperactivity should be considered [21]. Metacholine testing was not done in our patient since, due to his young age, he could not collaborate. In very young children, for whom spirometry or metacholine cannot be performed, diagnosis of asthma requires an experienced paediatrician or a specialist.
Due to our inability to confirm the diagnosis of asthma through spirometry, we tried a 4-week treatment with inhaled corticosteroids and bronchodilators. Clinical improvement and recurrence of symptoms after cessation of therapy confirmed the diagnosis of asthma [12].
During the patient’s admission several diagnoses were discussed as the underlying cause of RP.
Clearing of chest radiograph and absence of symptoms without treatment between admissions, were against extraluminal compression, congenital structural abnormalities of airways or lung parenchyma and foreign body aspiration which was not considered due to the older age (>3 yrs) of the patient.
Immune deficiency could cause RP; however, infections usually start at younger age and may involve more than one lobe or systems. Normal serum immunoglobulins ruled out B-cell deficiency. Adequate granulocyte count and quick resolution of CXR findings were against neutrophil dysfunction which usually presents with persistent staphylococcal or aspergillus infections. Cystic fibrosis (CF), another cause for RP, was ruled out due to normal sweat test. Nevertheless, normal nourishment, absence of gastrointestinal malabsorption, normal CXR between episodes were not suggestive of this diagnosis [6].
Investigation for primary ciliary dysfunction (PCD) was discussed during the 3rd admission. This functional inability to clear secretions, presents with purulent rhinitis, recurrent middle ear disease, situs inversus in one-half of patient’s and possibly bronchiectasis [6], none of which were present in our patient or shown in chest CT.
A few series have reported RP in children showing that an underlying cause of RP is usually identified and can vary greatly in different geographic locations [22].
In Spain, the most common underlying causes for RP included asthma (30.4%), congenital cardiac defects (29.3%), and aspiration syndrome (27.1%) [23]. In the USA, 40% of patients with RP had asthma, 10% aspiration and 5% immunodeficiency syndromes [10]. In Turkey, the most common underlying causes of RP were asthma (32%), gastro-oesophageal reflux (15%), and in children younger than 2 yrs old, immunodeficiency (10%) and aspiration syndromes (3%) [4]. In contrast, in series from Canada [3] and India [5], aspiration was the leading cause [6].
Diagnosis of asthma, even if it can frequently cause recurrent pneumonia, was not initially considered in our patient, because he did not have the classic symptoms of episodic wheezing, atopy, nocturnal or exercise-induced cough. Instead, prior to hospital admissions he had fever, cough and dyspnoea. These symptoms and not wheezing may be the initial presentation of asthma [12, 24–26].
We considered this case unusual because of the: presentation of asthma, nonreversibility of spirometry despite recurrent CXR inflammation, absence of atopy, laboratory tests suggesting bacterial pneumonia, while fast clearing of CXR infiltrates was suggesting atelectasis. However, the response of the patient to appropriate anti-asthma treatment was excellent. Interestingly, 2 years after the treatment started, he is entirely asymptomatic with his spirometry showing reversibility of obstruction in small bronchi.
Footnotes
Competing interests
None declared.
- ©ERS 2011
References










