





Abstract
Summary Ventilation/perfusion single photon emission computed tomography (V/P SPECT), is the scintigraphic technique of choice for the diagnosis of pulmonary embolism (PE) and other conditions that affect lung function. In the study of ventilation, hydrophobic radioaerosol Technegas shows advantages over radiolabelled liquid aerosols because of its more even distribution and better peripheral penetration; this is very important in patients with COPD. Macro-aggregated human albumin is the imaging agent for perfusion scintigraphy. V/P SPECT is recommended as a one-day protocol and the whole study is conducted in 20 minutes under a gamma camera. An optimal combination of nuclide activities for ventilation and perfusion, general purpose collimators and a 64×64 imaging matrix yields an adequate sensitivity and ensures that radiation doses are kept very low. It is important that the patient remains in an unchanged supine position to allow reconstructed images of matching ventilation and perfusion slices in all projections as well as in rotating volume images. Probabilistic interpretation applied earlier for planar technique is replaced by a holistic interpretation strategy. This has resulted in a decrease in the number of nondiagnostic findings to less than 3%. To reduce costs and radiation exposure, pre-imaging assessment of clinical probability is recommended. PE is diagnosed when there is more than one subsegment showing a ventilation/perfusion mismatch conforming to an anatomic vascular lung unit. Apart from PE, other pathologies should be identified and reported, e.g. COPD, heart failure and pneumonia.
Comparison of V/P SPECT with multidetector CT (MDCT) showed higher sensitivity for V/P SPECT, similar specificity and a similar number of nondiagnostic findings. The advantage of V/P SPECT is a 25-times lower absorbed radiation dose to the female breast and its applicability to all patients. The advantage of MDCT is its wider availability.
Hybrid SPECT/CT imaging is a novel technique primarily developed to improve sensitivity and specificity of oncological diseases and it is not recommended as the primary tool for PE diagnosis in all patients with suspected PE. The application of SPECT/CT may be relevant in the case of COPD patients where small tumours may be identified as part of the diagnosis; in addition, it may help in the classification of COPD degree.
Aims
-
To increase awareness of the importance of optimal V/P SPECT and familiarity with the procedure.
-
To explain the value of the new holistic, as opposed to probabilistic, interpretation in the diagnosis of PE.
-
To show how the quantification of ventilation/perfusion defects can be used to define patient-specific treatments.
-
To understand the role of V/P SPECT scintigraphy in other cardiopulmonary diseases, in addition to PE.
-
To outline the pros and cons of angio-CT and V/P SPECT in the diagnosis of PE.
-
To introduce the role of V/P SPECT and low-dose CT hybrid system in patients with suspected PE.
Pulmonary embolism
The diagnosis of pulmonary embolism (PE) is still a big challenge because the clinical symptoms and signs, which are frequently observed in, and hence may be indicative of, PE, are also a feature of other conditions. Accordingly, the initial diagnosis needs to be confirmed or negated using a conclusive imaging test. Multidetector CT (MDCT) is suggested as the initial imaging study by many authors although the latest evidence shows that the optimal test is ventilation/perfusion single photon emission computed tomography (V/P SPECT) interpreted with holistic principles according to European Guidelines [1]. The guidelines suggest, in the first instance, the use of a clinical predictive model for PE as suggested by Wells et al. [2] or a more precise predictive model developed by Miniati et al. [3]. Easy-to-use software is available for computation (palm computer; www.ifc.cnr.it/pisamodel).
The measurement of D-dimer, a breakdown product of cross-linked fibrin clot, is widely used in the investigative workup of patients with suspected venous thromboembolism [2, 4]. However, D-dimer has a low specificity (40%) because a number of conditions, other than venous thromboembolism, may cause it to be elevated: e.g., acute myocardial infarction, stroke, inflammation, active cancer and pregnancy. The specificity declines even further with age and, in the elderly, may reach only 10% [4]. Due to the low predictive value, a positive quantitative D-dimer test does not modify the pretest probability. A negative quantitative d-dimer test combined with a low clinical probability is associated with a low risk of thromboembolic disease. At moderate-to-high pretest clinical probability, D-dimer has no incremental value.
Basic principles of PE diagnosis with V/P SPECT
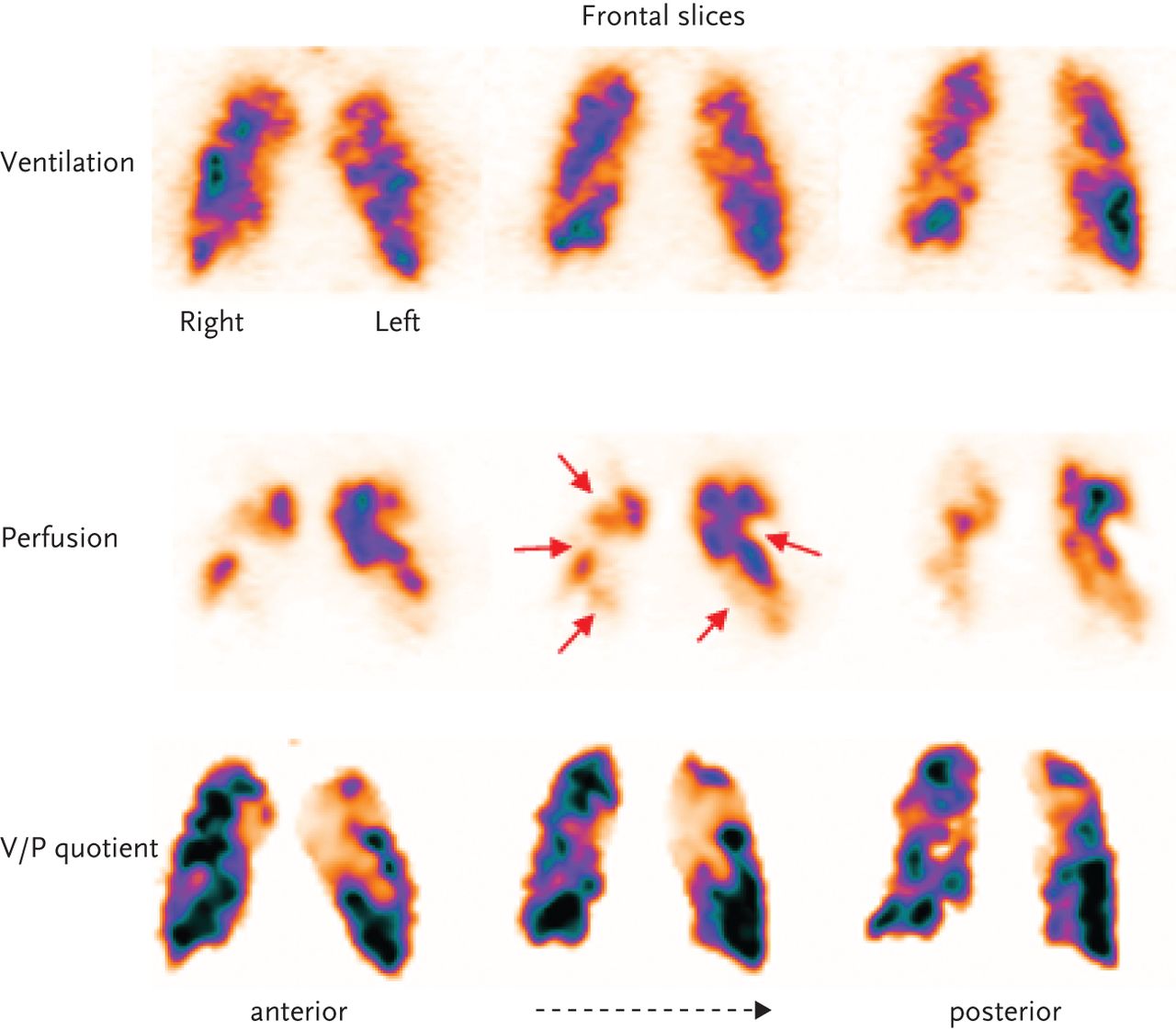
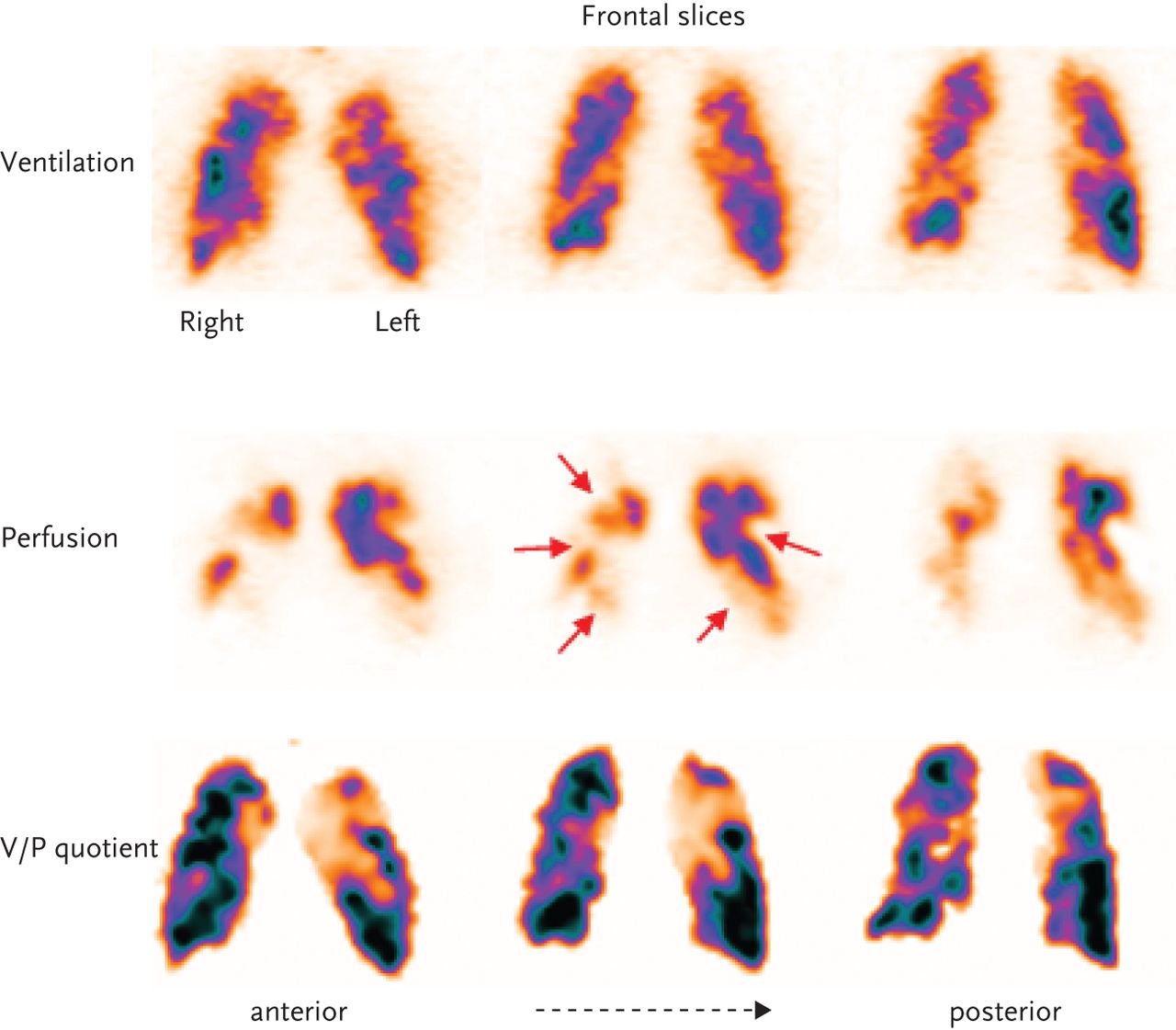
The lung circulation has a distinct architecture where each bronchopulmonary segment and sub-segment is supplied by a single end-artery. The arteries supply a conical zone with apex towards the hilum and base along the pleural surface. Emboli, which are usually multiple, occlude the arteries causing segmental or sub-segmental perfusion defects within still ventilated regions, causing mismatch (fig. 1). During the process of resolution/breakdown of emboli, perfusion may be only partially restored, in which case the V/P mismatch becomes less distinct. PE is often a recurring process giving rise to multiple emboli in various stages of resolution.

Patient with PE. Frontal slices; ventilation with corresponding perfusion images and quotient images. Multiple areas with absent perfusion (arrows) and preserved ventilation, clearly visible as mismatch on V/Pquotient images.
In clinical practice, a test that is both fast and conclusive is essential. To avoid the risks associated with untreated disease, it is recommended that imaging tests for PE diagnosis should be carried out as soon as possible, preferably within 24 hours of the onset of symptoms.
Imaging protocols
V/P SPECT acquisition
Administration of ventilation and perfusion agents should be performed with patients in a supine position, so as to minimise gravitational gradients. During inhalation, activity over the lungs should be monitored to ensure adequacy of pulmonary deposition.
The procedure starts with ventilation scintigraphy which is usually based upon inhalation of a radio-aerosol. The aerosol particles may be liquid diethylenetriaminepentaacetic acid labelled with technetium (99mTc-DTPA) or solid 99mTc-labeled solid graphite particles (Technegas), which are generated in a furnace at high temperature and are suspended in air. The deposition of the particles depends on the aerodynamic properties of the particles, mainly their size.
Large particles, >2 μm, are deposited mainly by impaction in large airways. Very fine particles, <1 μm, are mainly deposited in alveoli by diffusion. In comparison with liquid aerosols, Technegas showed significantly reduced problems of central airway deposition and peripheral hotspot formation in patients with obstructive lung disease [5]. Accordingly, there is a risk that PE may be overlooked in COPD patients when 99mTc-DTPA is used.
Perfusion tomography follows immediately after ventilation without changing the patient position. The nearly universally used agent for perfusion scintigraphy is technetium-labelled particles of macroaggregates of human albumin (99mMAA). After i.v. injection, the particles of size 15–100 μm are lodged in the pulmonary capillaries and in the precapillary arterioles in proportion to perfusion.
To achieve adequate imaging quality, with low radiation exposure, in a short time, relationships between activities, acquisition times, collimators and matrices for SPECT imaging must be optimised. This problem was systematically analysed by Palmer et al. [6] in the context of a dual-head gamma camera. Doses of 25–30 MBq for ventilation studies and 100–120 MBq for perfusion studies were found to be optimal. Using a general purpose collimator, a 64×64 matrix was adequate. This allowed a total acquisition time of only 20 minutes. A matrix of 128×128 required higher doses and/or longer acquisition times. This is not advocated as it did not yield images of significantly higher quality.
Many centres are using much higher doses. As ethical concerns and good medical practice are crucial issues, radiation exposure should be minimised to the lowest level consistent with satisfactory image quality. The total number of projections should be about 120–128 (60–64 with each camera head). For ventilation, each step lasts 10 s. For the perfusion study that follows immediately after the ventilation study, each step lasts 5 s. During the examination, it is important that the patient retains the same supine position, carefully maintained between ventilation and perfusion acquisitions.
For V/P SPECT it is important to use iterative reconstruction. Recommended is ordered subset expectation maximization (OSEM) with eight subsets and two iterations. Standard software can be used for image presentation in frontal, sagittal and transversal projections as well as for presentation of rotating 3-dimensional images. We have developed a way of calculating and displaying ventilation/perfusion quotient images. This is based upon acquisition as described above. Ventilation is normalised to perfusion counts, and then the V/P quotient images are calculated. V/P quotient images facilitate diagnosis and quantification of PE extension. Using this protocol, attenuation correction is not needed [6, 7].
An overview of ventilation and perfusion in frontal and sagittal slices is useful for quality control and fast orientation. For review of the study, it is important to present the images so that ventilation and perfusion are carefully aligned to each other (fig. 2). This is greatly facilitated by the one session protocol with the patient in unchanged position. The option to triangulate between frontal (coronal), sagittal and transverse slices is valuable for identification of matching and non-matching ventilation and perfusion changes. Proper alignment is also a prerequisite for V/P quotient images. These facilitate the interpretation and quantification of PE extension. However, quotient images are not crucial for high quality V/P SPECT.

Overview image of ventilation and perfusion in frontal and sagittal slices. Ventilation and perfusion are carefully aligned to each other.
Volume images based upon maximum intensity projection are available with standard software. Such rotating images give a good overview of ventilation and perfusion changes, facilitating the evaluation of the segmental or non-segmental character of changes.
Reporting findings
Ventilation/perfusion patterns
For V/P SPECT, a new holistic principle for reporting is as important as the imaging technique itself. This goal was not achieved with previous probabilistic reporting methods according to PIOPED (Prospective Investigation of Pulmonary Embolism Diagnosis) or modified PIOPED [8, 9]. Large V/P SPECT studies have shown that interpretation of all patterns representing ventilation together with perfusion achieves this result [10–14]. Conclusive reports were given in 97–99 % of cases.
Criteria for acute PE
Recommended criteria for reading V/P SPECT with respect to acute PE are the following [1]:
-
PE is reported if there is V/P mismatch of at least one segment or two sub-segments that conforms to the pulmonary vascular anatomy;
-
No PE is reported if there is (are) normal perfusion pattern conforming to the anatomic boundaries of the lungs matched or reversed mismatch V/P defects of any size, shape or number in the absence of mismatch, mismatch that does not have a lobar, segmental or sub-segmental pattern;
-
Non-diagnostic for PE is reported if there are multiple V/P abnormalities not typical of specific diseases.
Crucially with PE, a mismatch has its base along the pleura and conforms to known sub-segmental and segmental vascular anatomy as stressed in the PISAPED (Prospective Investigative Study of Acute Pulmonary Embolism Diagnosis) study [15]. Applying these principles of interpretation, recent V/P SPECT studies amounting to over 3,000 cases report a negative predictive value of 97–99%, sensitivities of 96–99%, and specificities of 91–98% for PE diagnosis and rates of non-diagnostic findings were 1–3% [10, 12, 13].
An important step in the diagnostic procedure is to quantify the extent of embolism. V/P SPECT is particularly suitable for this because of its greater sensitivity compared to alternative planar scintigraphy and MDCT [10, 11, 14]. As suggested by Olsson et al. [16], the number of segments and sub-segments indicating PE typical mismatch are counted and expressed in % of the total lung parenchyma. Furthermore, areas with ventilation abnormalities were recognised and this allowed the degree of total lung malfunction to be estimated. The study showed that patients with up 40% PE could be safely treated at home if ventilation abnormalities engaged not more that 40% of the lung. Since 2004, more than 1000 (50%) of patients with PE, have been safely treated at home in the University Hospital of Lund.
Importance of ventilation SPECT in diagnosis of other lung diseases
COPD
A common alternative or additional diagnosis is COPD. The characteristic is a general unevenness of ventilation. Focal deposition may be observed in central or peripheral airways even when using Technegas [5]. A very important fact is that COPD patients are at high risk of PE. The rate of PE in patients hospitalised for acute exacerbations of COPD may be as high as 25% [17]. Different from PIOPED study with V/P SPECT, PE can be diagnosed even in the presence of COPD [1, 10, 18]. PE accounts for up to 10% of deaths in stable COPD patients [19]. The degree of unevenness of aerosol distribution correlated with lung function tests [20]. Significantly, as there are no contraindications to V/P SPECT, even very sick and breathless patients can be studied. Figure 3 shows frontal slices in a patient with COPD and PE. Mismatch is highlighted in V/P quotient images.
Patient with COPD and PE. Frontal slices; very uneven distribution of ventilation with deposition of aerosols in small airways (upper row). Multiple segmental and subsegmental perfusion defects (arrows) in ventilated areas, well delineated on V/Pquotient images.
Pneumonia
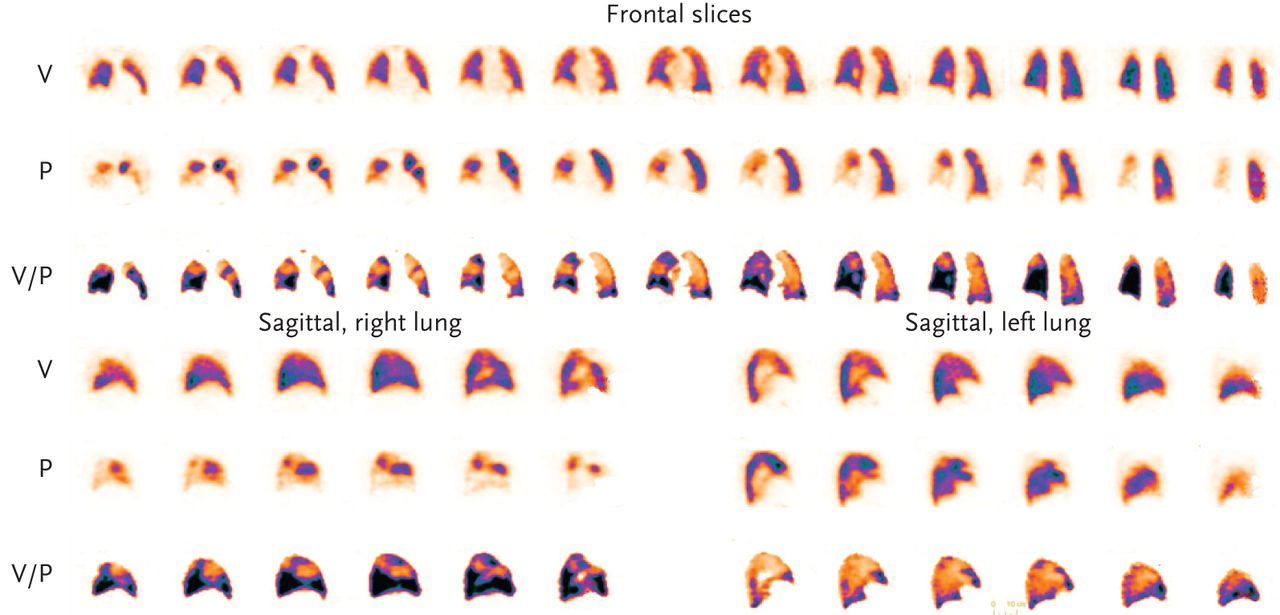
Pneumonia is also frequent in patients investigated for suspected PE [10]. A typical finding is a ventilation defect in an area usually with better preserved perfusion, known as reverse mismatch [21, 22]. One of the typical patterns, which strongly support the diagnosis of pneumonia, is the “stripe sign”. This refers to maintained perfusion along the pleural surface, peripheral to a central matched defect as observed on fig 4. Moreover, this patient had also a PE in medial lobe. V/P SPECT allows diagnosis of both, PE and pneumonia.

Patient with pneumonia in the right lung and PE. Sagittal slices show reduced–absent ventilation posteriorly with reduced perfusion in the same area. Preserved perfusion adjacent to the pleura (stripe sign; blue arrow). Moreover, absent perfusion with preserved ventilation in the medial lobe (red arrow).
Left heart failure
Left heart failure is another diagnosis that is often observed among patients suspected of PE. The typical pattern is anti-gravitational redistribution of perfusion [23, 24]. In consecutive patients with suspected PE, V/P SPECT showed anti-gravitational redistribution of perfusion in 15% of the cases indicating left heart failure [25]. The positive predictive value for heart failure in this study was at least 88%. As ventilation is usually less redistributed than perfusion, V/P mismatch may be observed in dorsal regions. This V/P mismatch has a non-segmental pattern and should not be misinterpreted as PE (fig 5a). Follow up, 10 days later, showed normalisation of gravitational distribution of ventilation and perfusion. However, the patient had developed a clearly delineated pattern of pneumonia in the upper right lobe (fig 5b).
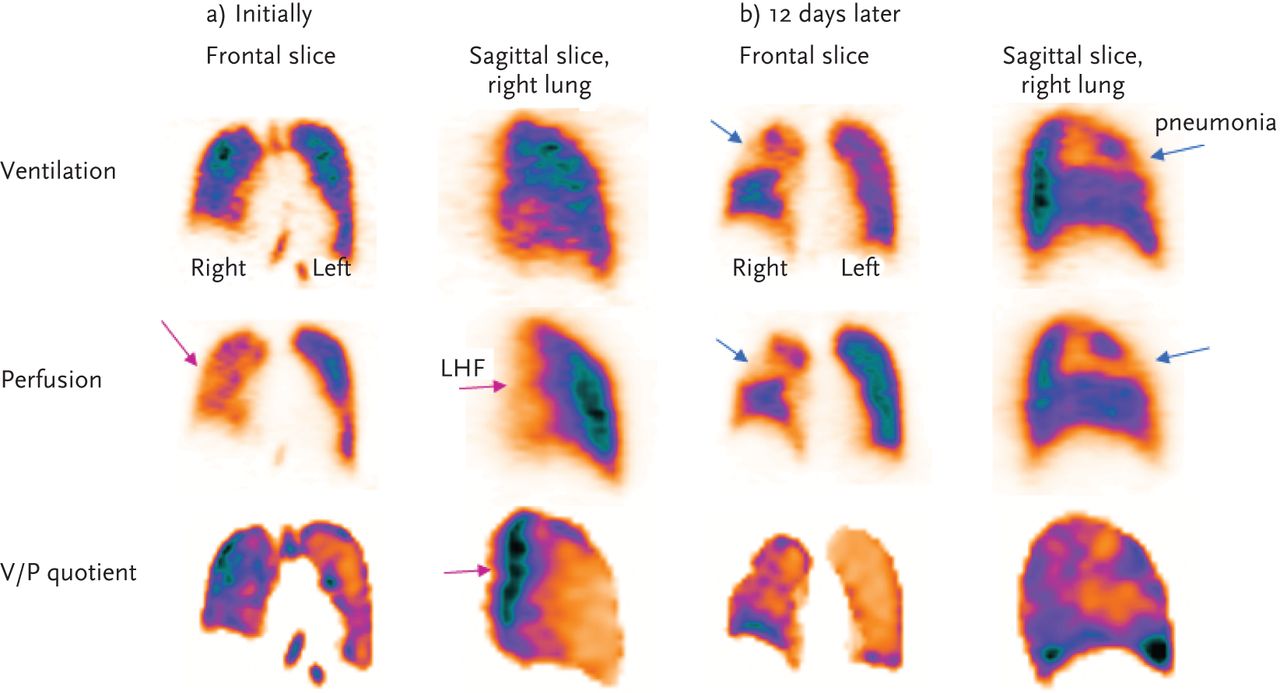
a) Patient with left heart failure in the initial acute stage. Frontal and sagittal slices; antigravitational distribution of ventilation and more so of perfusion, causing non-segmental V/P mismatch in dorsal regions (purple arrows). b) The same patient, follow up after 12 days of treatment for left heart failure. Normalisation of gravitational distribution of ventilation and perfusion. However, the patient had developed a clearly delineated pattern of pneumonia in the upper right lobe, absent ventilation and perfusion with “stripe sign” (blue arrows).
Pitfalls in the interpretation
Several diseases and conditions lead to mismatch. It is essential to be able to recognise the characteristic patterns of mismatch for the different diseases and conditions in order to avoid misdiagnosis).
In non-acute PE that is partly resolved, perfusion defects often lose their characteristic clear segmental pattern and this may lead to a false negative diagnosis.
Mismatched defects are observed in lung cancer, mediastinal lymphadenopathy, postradiation pneumonitis, vasculitis and heart failure, etc. In general, such mismatches have a non-segmental character. Some emboli, such as saddle embolus [26], do not lead to mismatch because they do not cause vascular occlusion. Nevertheless, a normal perfusion scintigraphy excludes PE according to wide experience. Accordingly, missed major non-occlusive emboli do not lead to clinical consequences like sudden death. The reason for this is probably that such emboli are accompanied by small occluding emboli, which are detected with V/P SPECT, so that PE is diagnosed and treated. Hence, it is important not to overlook small emboli.
Unilateral whole lung mismatch without any mismatch in the other lung is usually not due to PE [27, 28]. In such cases, an MDCT is recommended to reveal much more likely pathologies such as tumour and other mediastinal processes or extremely rarely congenital pulmonary vascular abnormalities or aortic aneurysm.
V/P SPECT versus MDCT
MDCT is often recommended as the first line test for PE diagnosis [29]. However, the principal study evaluating the use of MDCT as an imaging tool for PE diagnosis shows that sensitivity is not more than 78% and that there are a high number of false positive results when clinical probability is not high [30]. In this study the positive predictive value for a PE within a lobar pulmonary artery was 97% but fell to 68 and 25% in segmental and subsegmental pulmonary vessels, respectively.
Advocates for MDCT stress that this method has the advantage over V/P SPECT by allowing also alternative diagnoses. However, V/P SPECT provides evidence about alternative diagnoses as well. In a V/P SPECT study comprising 1,785 patients an alternative diagnosis was reported in 39% of patients without PE, while among patients with PE an additional pathology was reported in 22% [10]. Actually, a properly performed V/P SPECT interpreted on the basis of all patterns of ventilation and perfusion, frequently allows diagnosis of other pulmonary disease with or without PE and a comprehensive understanding of the patient's symptoms. This added value of V/P SPECT appears at least as high as for additional diagnosis as with MDCT. Further studies are needed in order to demonstrate the clinical impact of alternative diagnoses obtained by both methods.
The lack of a satisfactory gold standard for PE diagnosis poses difficulties for the assessment of sensitivity, specificity and accuracy of all diagnostic methods for PE. The best available point of reference is an adequate follow up of the patients to identify a recurrence of PE or alternative diagnoses as seen in figure 5a and b.
After a negative single slice CT, PE occurred in 1.4% of patients in a meta-analysis of 4,637 patients [31]. After a negative pulmonary angiography study this was 1.6% [32] and after a negative MDCT 1.5 % (n = 318). After a negative ventilation/perfusion scintigraphy, occurrence of PE during follow up was 0.4% in a total of 1,877 patients [33]. Freeman et al. [34] stated that the results from the PIOPED II study “do not clearly support the superiority of CT angiography over ventilation/perfusion scanning for the diagnosis of PE”. However, this conclusion was based upon ventilation/perfusion planar technique and probabilistic interpretation. A direct comparison between V/P SPECT 4-slice and 16-slice MDCT respectively showed a higher sensitivity by V/P SPECT [11, 14]. Further prospective comparisons between up-to-date V/P SPECT and MDCT are needed. In interpreting V/P SPECT, low inter-observer variability has been shown by a kappa value of 0.92 [10]. Moreover, PIOPED II [30] as well as the study by Gutte et al. [11] illustrate well the limited clinical utility of CTPA. In 50% of eligible cases, MDCT could not be performed because of kidney failure, critical illness, recent myocardial infarction, ventilator support and allergy to the contrast agent. Furthermore, 6% of performed MDCT studies were of insufficient quality for conclusive interpretation. In about 1% complications, such as allergy, contrast extravasations and increased creatinine level, were observed [11, 30]. By contrast, VP SPECT has no contraindications and was performed in 99 % of patients referred in the study of Bajc et al. [10]. Complications do not occur and technically suboptimal studies are very rare. It is possible to accommodate patients who are mechanically ventilated by connecting a nebuliser to the inspiratory ventilator line. In rare cases, when V/P SPECT cannot be performed, planar technique is the alternative.
Radiation doses
Based upon data from ICRP reports [35], the effective dose for V/P SPECT with the recommended protocol is about 35–40% of the dose from MDCT [36]. The dose to the female breast for V/P SPECT is only 4% of the dose from MDCT with full-dose saving means according to Hurwitz et al. [37]. This may have particular importance in pregnant women with proliferating breast tissue [38]. During the first trimester of pregnancy, the fetal dose of MDCT is greater than or equivalent to that of V/P SPECT [39]. The advantage of V/P SPECT increases after the first trimester.
Follow up
Follow up of PE using imaging is essential to:
-
assess the effect of therapy
-
differentiate between new and old PE where there is a suspicion of PE recurrence
-
explain physical incapacity after PE
These demands for follow up are only met with V/P SPECT. Obviously, the same method should be used for diagnosis and for follow up.
Appropriateness for research
The suitability of an imaging technique for research into PE and its treatment and clinical follow up are in principle the same. However, in research, there are even stronger, ethical, grounds for the use of non-traumatic procedures associated with lowest possible risks.
Clinical use of hybrid V/P SPECT–CT
The hybrid V/P SPECT–CT system is a dual imaging modality technique whose clinical application is particularly relevant in oncological diseases as it leads to improved sensitivity and specificity, combining co-registration of anatomical and functional data. It may lead to improved staging and treatment monitoring. As nuclear medicine procedures have the ability to visualise early functional changes much sooner than structural changes occur, additional CT procedure may improve correction for photon attenuation and allow co-registration of morphology and function. However, V/P SPECT–CT acquisition of the chest constitutes a challenge due to respiratory movements, which can cause image artefacts and thus decrease diagnostic accuracy.
V/P SPECT–CT protocol
In our department we are using a Philips Precedence system which combines dual head gamma camera with a Brilliance 16-slice CT.
The procedure starts with CT overview image and continues with diagnostic low dose CT. (120 kV, 20 mAs per slice, 16×1.5 collimator, 0.5-s rotation time and pitch of 0.813) not used for attenuation correction but to exactly co-localise the morphological and functional changes visualised in either of the two modalities. Thereafter, follows the protocol for V/P SPECT as described earlier and according to the European Guidelines [1, 40]. Low-dose CT delivers approximately 1 mSv when used for alignment and attenuation correction. However, as a diagnostic tool in this hybrid system, it delivers 2–3 mSv and V/P SPECT 2, 1 mSv.
Some authors have recently recommended V/P SPECT low-dose CT as a first line procedure in patients with suspected PE. This was based on their prospective study performing V/P SPECT and low-dose CT and making head-to-head comparison with MDCT. In a total of 81 simultaneous studies 38% of patients had PE. They showed 97% sensitivity and 88% specificity when only V/P SPECT was used. However, adding low-dose CT the sensitivity was unchanged but specificity increased to 100%. Interestingly 18% of patients had false positive PE diagnosis when V/P SPECT alone was interpreted. A reason for this may be that they were interpreting every mismatch as PE and not only mismatches that conform to segmental lung circulation as recommended by European Guidelines [1, 40].
At our department, we use V/P SPECT as a primary tool in patients with suspected PE. Since 2003, more than 11,000 examinations have been performed. In a retrospective study of 1,785 patients who were followed up clinically, sensitivity for V/P SPECT was 99%, specificity 98%, and 1% of nondiagnostic findings [10]. Similar results have been shown by other authors as well [12, 13].
Based on our experience, we do not recommend hybrid V/P SPECT–CT as a first-line procedure for all patients with suspected PE. It is not ethical to advocate higher radiation dose (2–3 mSv) for every patient with suspected PE where prevalence of PE is about 30% at our hospital. So, in our opinion, the recommendation to use a hybrid system for PE diagnosis is premature. Coco et al. [41] showed that CT utilisation has increased dramatically in the evaluation of patients with suspected PE, without improving rate of PE or other clinically significant diagnoses. Moreover, the patients are exposed at risks of radiation [42, 43]. Therefore, it is important to validate the V/P SPECT–CT system and not to adopt it too quickly, without fully assessing the benefits and risks.
We believe however, that the dual modality will have impact in some groups of patients.
V/P SPECT–CT may make a significant contribution to the diagnosis of COPD patients where the architecture of the lung is changed and remodelled. COPD is a heterogeneous disease as observed by morphological, physiological imaging and as clinical manifestations such as dyspnoea, productive cough and exacerbations. As COPD patients are prone to complications, such as PE, pneumonia, left heart failure and tumour, V/P SPECT–CT may facilitate the diagnosis of these. Despite this extensive heterogeneity, the definition and severity of COPD is currently assessed based solely on forced expiratory volume in 1 s (FEV1) [44]. FEV1 measures the degree of airflow limitation but provides no information about the underlying pathophysiology. Therefore, FEV1 cannot capture and explain the complex clinical consequences of COPD. High-resolution computed tomography (HRCT) may provide morphological information about the extent of emphysema, its type and localisation, but gives no functional evaluation. HRCT is not routinely recommended in COPD patients and correlation with FEV1 is not very strong [18, 44]. Better tools to understand and categorise different phenotypes of COPD are required.
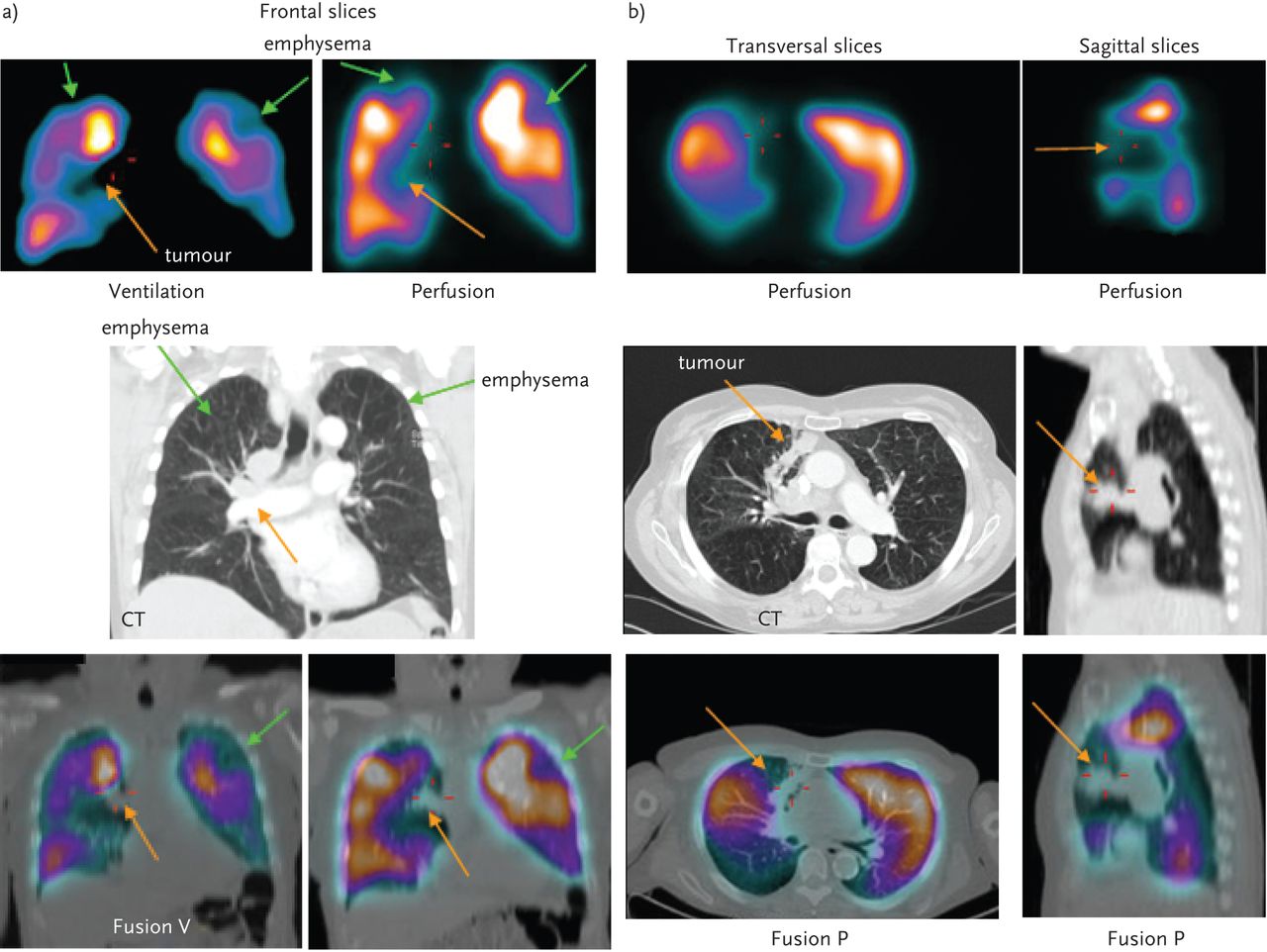
As we have already shown in an earlier study [18], it may be easier to understand and interpret the correlation of perfusion defects on perfusion slices with specific pulmonary arterial branches seen on CT slices and heterogeneous defects on ventilation slices caused by airways changes when applying both modalities. In figure 6, we can see images of a patient with COPD who was referred for further assessment of the disease. V/P SPECT showed matched defects in both upper lobe suspected to be emphysema (green arrows) and this was confirmed by CT images. Moreover on CT, a mediastinal tumour growing in lung parenchyma (orange arrows) was observed. Tumours cause decreased/absent ventilation and perfusion with a larger extent than morphological changes seen on CT. Here we can see added value of CT as it shows the exact location of the tumour and its propagation and V/P SPECT which shows the extension of total functional impairment. Sometimes, in COPD patients, we can observe small tumours and only CT may enable us to observe and diagnose them (fig. 7). Due to the uneven distribution of ventilation and perfusion in this group of patients tumours that are too small to be suspected and identified, only using V/P SPECT. However, aligning CT image with corresponding perfusion slice small distinct perfusion defect is observed caused by tumour (fig 7).

a) Patient with COPD and tumour. In the top row, coronal slices display uneven distribution of ventilation with deposition of Technegas typical for COPD. Perfusion follows ventilation pattern. Matched ventilation and perfusion defects (green arrows) are observed in the both upper lobe and in the mediastinum right (orange arrow). In medial row of on the corresponding frontal CT slice, emphysema is observed in both these upper lobes (green arrows) and tumour in the mediastinum (orange arrow). In lower row fusion images of CT and ventilation SPECT on the left and CT and perfusion SPECT on the right. b)The same patient: Left upper row: Transversal slice of perfusion with corresponding CT slice in the middle row. A large perfusion defection is caused by a tumour which can be clearly seen in the fusion image in the lower row. On the right; sagittal slice shows an extensive area with absent perfusion (orange arrow) caused by the tumour seen on CT (middle row) and on fusion image (lower row).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient with COPD, left heart failure and small tumour. On the left; upper row frontal slice of ventilation SPECT showing uneven distribution of ventilation with central deposition of Technegas typical for COPD. Middle row corresponding perfusion SPECT image and lower row corresponding CT image. Blue arrow on CT image shows thickening of the airway wall typical of COPD. In the middle transversal slices of ventilation SPECT upper row, with corresponding perfusion SPECT in the middle row. On CT image in lower row small tumour (1 cm) is visualised. Aligning both modalities small perfusion defect is observed in this area (arrow). On the right column; sagittal slice upper row presents Fusion ventilation SPECT/CT, middle row with corresponding fusion perfusion SPECT/CT slice that shows antigravitational redistribution os perfusion, typical for left heart failure (violet arrow) not visible on CT nor ventilation (non segmental mismatch).
Increased knowledge will improve future interpretation. Moreover V/P SPECT - CT might help with better classification of COPD patients, by improving the estimate of obstructivity [18]. A study is in progress to validate this.
Conclusions
V/P SPECT should be used as a primary tool for the diagnosis of PE because it has the highest sensitivity and accuracy and neither contraindications nor complications. In addition, it produces very few non-diagnostic reports (1–3%). Furthermore, radiation doses are very low. This is particularly important for women in the reproductive period and during pregnancy. To take full advantage of the V/P SPECT potential, it is crucial to apply an optimal protocol for a single session imaging of both ventilation and perfusion using low nuclide activities. Furthermore, full use should be made of display options, which are integrated in modern camera systems. Most important of all is holistic interpretation, giving a clear report with respect to PE, its extension as well as other diagnoses based on ventilation/perfusion patterns typical for various diseases. The above mentioned advantages of V/P SPECT for studying PE imply that it may be the most suitable technique both for follow up in patients with PE as well as for research regarding its treatment and pathophysiology.
V/P SPECT CT has further potential in COPD patients by enabling:
-
The evaluation of total lung function
-
The quantification of pathological extensions
-
The categorisation of the severity of functional changes and obstructivity
-
The identification of co-morbid diseases, frequent in this group
Acknowledgments
This work is partially financed by the Region of Scania (ALF) and Scania University foundations.
Footnotes
Statement of interest
None declared.
- ©ERS 2012
References











Jump To
- Article
- Abstract
- Pulmonary embolism
- Basic principles of PE diagnosis with V/P SPECT
- Imaging protocols
- Reporting findings
- Importance of ventilation SPECT in diagnosis of other lung diseases
- V/P SPECT versus MDCT
- Follow up
- Appropriateness for research
- Clinical use of hybrid V/P SPECT–CT
- Conclusions
- Acknowledgments
- Footnotes
- References
- Figures & Data
- Info & Metrics