





Abstract
Summary Nocturnal polysomnography (PSG) is the most important laboratory technique in the management of sleep–wake disturbances and is considered the “gold standard” [1]. New sensor technologies are entering the field, and rapid development in telecommunications and mobile technology has accelerated the introduction of telemedicine as a viable and reliable option [2]. The present broad review is an amalgam of the current knowledge with proposed new sensors and remote control. The reader should note that not all of the techniques discussed here have strong clinical validation, and this should be considered when purchasing equipment.
State-of-the-art technology
Based on the information obtained by electroencephalography, electro-oculography and electromyography (EMG), sleep stages can be defined according to the criteria of Rechtschaffen and Kales [3] and the new American Academy of Sleep Medicine criteria [4]. Ventilation is often measured qualitatively by means of thermistors but is more appropriately measured with nasal pressure cannulae, or by means of a pneumotachograph, connected with a full face mask, or calibrated inductance plethysmography, although calibration of this is difficult [5]. Breathing effort can also be detected by recording movements of the chest and abdomen, surface EMG, snoring, and changes in arterial blood pressure, but most effectively by detection of intrathoracic pressure swings. These swings can be detected by measuring oesophageal pressure. Movements of the chest and abdomen can be recorded with strain gauges (which detect changes in resistance according to length changes), inductance plethysmography or Respitrace (with detection of inductance characteristics of electrical conductors), impedance or even a static charge sensitive bed (which detects respiratory movements). If respiratory effort is detected during an apnoea, this can be explained by occlusion of the upper airways. Oxygen saturation is measured by means of pulse oximetry (SpO2), as well as transcutaneous carbon dioxide tension (PCO2). Sound recording is another method to detect ventilation. Frequency analysis of the sounds (predominantly snoring) can deliver more information on flow limitation. Routinely, body position (position sensor on the chest) is also recorded. The combined application of these measurement techniques allows the assessment of normal and abnormal physiological events in relation to sleep structure [6].
Changing paradigm
Standard signal processing is restricted to visual and semiautomatic analysis, while more in-depth information can be gathered using sophisticated algorithms. Updates of current PSG systems are rare, while the market moves apace with new technologies, such as new sensors, Wi-Fi and remote monitoring (telephone or video). Integration of these new and innovative technologies could contribute to better patient care, while development of algorithms that can differentiate sleep stages from ECG, pulse wave, respiratory dynamics [7] and movement sensors can simplify the diagnostic procedure. The increase in the processing and integration capacity of electronic devices, as well as advances in low-power wireless communications, has enabled the development of unwired intelligent sensors for a wide set of applications.
Technological developments in the assessment of sleep
Different approaches have been explored to develop new technologies primarily for the diagnosis of obstructive sleep apnoea (OSA), based on more advanced analysis of ECG and pulse waves, smart assessment of arousability, and new sensors. Some of these signals have the potential to replace established sensors in the long term.
ECG analysis
Heart rate variability
A one-lead ECG is routinely recorded during PSG to measure heart rate and rhythm, but little analysis is possible. The major challenge is very reliable R-wave detection with proper identification of ectopic beats and artefacts. Monitoring of heart rate, and in particular heart rate variability (HRV), by overnight ECG has long been recognised as a potential diagnostic strategy in patients with suspected sleep disordered breathing [8, 9]. No additional electrodes or additional devices are required except dedicated software to carry out the analysis [10]. Analyses of the HRV components within the very low-frequency (VLF), low-frequency (LF) and high-frequency (HF) domains provide insight into autonomic activation. The VLF component concurs with vasomotor activity and thermoregulation, while the LF component corresponds with both sympathetic and parasympathetic tone and their modulation of the atrial sinus node. In contrast, the HF component primarily reflects parasympathetic tone. Taken together, the ratio of LF to HF power provides insight into sympathovagal balance [11]. Recently, some studies have shown that it is even possible to distinguish slow-wave sleep, rapid eye movement (REM) sleep and wakefulness based on heart rate series by using a detrended fluctuation analysis of the heart beat [11–14].
ECG-derived respiration
Other modalities using overnight ECG include analysis of dynamic changes in ECG morphology accompanying obstructive events, the accuracy of which may be significantly enhanced by the application of sophisticated diagnostic algorithms [15]. This enables the derivation of respiration from the ECG by tracking the amplitudes of the prominent R-wave. The derived respiratory curve is called ECG-derived respiration and correlates reasonably well with respiratory effort based on inductance plethysmography. The combination of ECG-derived respiration and sleep apnoea related HRV has the potential to be a good and reliable detection tool for sleep apnoea, but high-quality, empirical evidence on this subject is so far lacking [16].
Altogether, this indicates the ECG signal is a powerful tool with rich content that can even be used as a simplified screening device [17]. It can also be used to separate obstructive from central apnoea [18].
Cardiopulmonary coupling analysis
The heart beat will slow down and speed up in tune with regular ventilation. During breathing instability, the heart and breathing rates become less synchronised, and the way the two signals are coupled together will change. A Fourier-based analysis technique uses HRV and ECG R-wave amplitude fluctuations associated with respiration to generate frequency maps of coupled autonomic-respiratory oscillations. The resulting sleep spectrogram is able to categorise sleep as stable (high-frequency coupling) or unstable (low-frequency coupling). Wake and REM sleep exhibit very low-frequency coupling (LFC). Elevated LFC is a subset of LFC that is associated with fragmented sleep of various aetiologies [19]. Cardiopulmonary coupling measures can differentiate normal individuals from those with moderate-to-severe OSA [20]. Incorporating cardiopulmonary coupling technology in routine sleep studies could indirectly measure sleep quality.
Parameters derived from the pulse wave
Pulse transit time
The pulse transit time (PTT) is derived from the ECG and the photoplethysmographic arterial pressure wave measured by a finger probe, which has been shown to reflect inspiratory effort [21] and can therefore be used to assess cardiovascular risk. PTT is based on measuring the time required for the arterial pulse wave to travel between two points in the arterial tree: from the moment when the pulse leaves the aortic valve (R-wave on ECG) to the time when it reaches the vessels in the finger as identified by pulse oximetry. Pulse wave speed depends on the vessel stiffness and stiffness is in turn determined by blood pressure. During airway obstruction, increased swings in the intrathoracic pressure modulate blood pressure and induce parallel changes in PTT [1]. Oscillations estimate swings of pleural pressure that occur during the obstructive breaths with high sensitivity and specificity. Up-to-date PSG systems calculate PTT, but it plays a minor role in the decision tree.
Peripheral arterial tonometry and pulse wave analysis
The use of peripheral arterial tonometry (PAT) enables us to take a closer look at the pulse wave itself, which is recognised by a sensor applied to the subject’s finger [22]. The amplitude of the pulse wave is modulated by sympathetic tone and cardiovascular stroke volume. Arousals can easily be recognised by drops in pulse amplitude, while slow-wave sleep and REM sleep can be distinguished based on pulse rate analysis [23]. This method is well known as the WatchPAT device (Itamar, Cesarea, Israel). This approach has been validated in a number of studies, whether used in isolation, or in combination with oximetry and/or actigraphy [23]. Furthermore, this approach has the potential to allow estimation of future cardiovascular risk via the identification of endothelial dysfunction [24]. So far, PAT has not been integrated with PSG but rather positioned as an isolated screening tool. Currently, a compact screening device for the wrist (SOMNOcheck micro; Weinmann Medical Technology, Hamburg, Germany) is available that has implemented pulse contour analysis for this purpose. Combination of pulse wave analysis and respiratory flow signals may allow the differentiation between obstructive and central apnoea, and offer information on the extent of sleep fragmentation. Recently, a novel pulse oximeter-based product has been developed that uses a computer-aided scoring solution (Morpheus Ox; WideMed, Herzliya, Israel). It uses photoplethysmography and measures oxygen saturation and pulse, and applies an automatic sleep scoring software to produce an accurate and reliable sleep analysis, including identification of sleep–wake, apnoea–hypopnoea index (AHI) and Cheyne–Stokes respiration. A mobile telephone application is available, capable of recording and transmitting the data collected during the test. This has opened a whole new dimension to the use of oximetry to screen for sleep-related breathing disorders (SRBDs).
Blood pressure
Elevated blood pressure or absence of blood pressure dip presents the link to the cardiovascular consequences of sleep disorders. Several studies have proven that OSA is an independent risk factor for developing daytime hypertension with an increased morbidity and mortality [25]. In selected cases, arterial blood pressure is measured intermittently by a pneumatic cuff around the upper arm and a sphygmomanometer [26], but these are likely to be too “invasive” to be used routinely in the sleep centre because the patient may arouse when the cuff inflates [27]. In addition, the arm cuff readings cannot keep track of the rapid blood pressure changes that are observed in OSA and during arousals. As an alternative, a continuous measurement of blood pressure can be obtained by finger photoplethysmography [28, 29]. This technique provides beat-by-beat pressure curves that allow assessment of blood pressure variability, which may be increased in SRBDs [30]. The finger photoplethysmographic method consists of a miniature cuff that fits on the finger and provides a continuous blood pressure signal derived from one (Finapres; Finapres Medical Systems, Amsterdam, the Netherlands) or two inflated finger cuffs (Portapres; Finapres Medical Systems). A new approach is noninvasive blood pressure measurement without a cuff (based on PTT), which has been clinically validated (SOMNOtouch; SOMNOmedics, Randersacker, Germany).
Capnography
The recording of PCO2 is performed using capnography based on infrared absorption spectroscopy. The derived readings are end-tidal PCO2 values. The disadvantage of this method is impairment of patient sleep comfort due to the need for a mask or a small tube inserted in the exhaled air connected to the carbon dioxide detection unit. Transcutaneous PCO2 measurement can be used as an alternative and uses heated electrodes on the skin; the electrodes have to be attached carefully because placement and sensor temperature are important modifiers of signal quality and tolerance [25]. Recently, a novel transcutaneous combined sensor for PCO2 and arterial oxygen saturation measurements (TOSCA 500; Linde Medical Sensors, Basel, Switzerland) was introduced into clinical practice [31]. Most studies concluded that these devices are both accurate and practicable in various settings [31–36]. Another carbon dioxide sensor with ultralow-power characteristics was developed by NXP Semiconductors (Eindhoven, the Netherlands) that enables room temperature sensing for carbon dioxide.
Respiratory sound recordings and analysis
Sound recording is generally performed to assess snoring. There is no widely accepted standard for recording sounds during sleep studies [37, 38]. Calibrated and uncalibrated semi-miniature microphones or vibration sensors taped to the skin at the level of the larynx, the suprasternal notch or forehead, and microphones placed at a certain distance from the head have been employed [38–41]. For subsequent analysis, the microphone recordings are only interpreted in terms of relative loudness and, therefore, the recording of this signal does not need to preserve sound signal characteristics [25]. A new approach tries to analyse respiratory sounds in order to derive noninvasive measures of increased respiratory effort [42]. In another system, respiratory sounds are recorded at the throat and signal processing separates cardiac and movement sounds from breathing sounds and snoring. Breathing is then quantified and snoring sounds are investigated in order to determine respiratory events [43]. Combination with oximetry seems even more promising. Wheeze monitoring can also be useful to screen for nocturnal wheezing in patients with bronchial asthma and nocturnal respiratory symptoms.
Audiovisual recording
Continuous video monitoring is also performed and is particularly helpful in the assessment of nocturnal behavioural disorders. Time-synchronised audiovisual recording is part of PSG, using a video camera and a room microphone in the sleep centre. Current standard infrared video cameras with infrared light sources provide images of excellent quality [37]. Acoustic analysis could also be used for at-home screening. Finally, the use of bone-conduction microphones has the potential to record snoring sounds directly and reduce background noise [44].
Body and head position
Continuous recording of body position by an accelerometer is important, as snoring and upper airway obstruction during sleep are influenced by gravitation [45]. Simple sensors encode the angle of the body into a continuous voltage. Other transducers use miniature contacts to convert an angle into a voltage or digital code. Switch or contact-based sensors are usually able to encode not only the angle but also upright or supine position [25]. These devices are calibrated prior to beginning the test, identifying each voltage output with a particular position. OSA may also be dependent on the position of the head. There is evidence that in a significant proportion of patients, trunk and head position during sleep are not the same. Therefore, sleep recording with dual position sensors placed on both the trunk and head should be considered [46]. This can be realised by an electromechanical sensor in the middle of the forehead just above the eyebrows, mainly based on the displacement of a small mercury droplet within the sensor in different positions. This approach can be illustrated with the Ares unicorder (Advanced Brain Monitoring, Carlsbad, CA, USA). From a single site on the forehead, the wireless unicorder records oxygen saturation and pulse rate (reflectance pulse oximetry), airflow (nasal cannula), respiratory effort (using a pressure transducer sensing forehead venous pressure, venous volume by photoplethysmography and actigraphy), snoring levels, and head movement and head position (accelerometers) [47]. Rofouei et al. [48] developed a new platform housed in a soft neck-worn collar, composed of an ear oximeter sensor, a small microphone placed against the neck, and an accelerometer measuring body movement and position of the head.
Specific movement recording
Midsagittal jaw movements
Another novel technique includes estimation of respiratory effort by measuring jaw movements (Jawac; Nomics, Angleur, Belgium) (fig. 1). This approach is based on magnetic distance determination [49]. A magnetic sensor on the chin and another on the forehead allow the operator to continuously determine the relative jaw movements, and indirectly derive respiration and snoring. Recently, it was validated against the gold standard, the oesophageal pressure catheter, in OSA and central sleep apnoea [50]. Moreover, by an advanced analysis of the signals, it is possible to estimate a sleep–wake profile [51]. Combination with oximetry and pulse wave analysis will allow a comprehensive diagnosis of SRBD without full PSG.

Jawac technology: sensing mandibular movements during sleep. Reproduced with permission from Nomics (Angleur, Belgium).
Diaphragmatic muscle activity
Recording diaphragmatic activity from surface skin electrodes seems to have been neglected for a long time. Recently, a new easy-to-handle and noninvasive way of monitoring respiratory muscle activity by means of surface electrodes was introduced (Dipha; Inbiolab, Groningen, the Netherlands), which can be used as an indirect measure to assess respiratory mechanics during wake and sleep [52] (fig. 2).

Dipha device for transcutaneous diaphragmatic muscle activity. Reproduced with permission from Inbiolab (Groningen, the Netherlands). RMS: root mean square of the myoelectric signal.
Temperature
New flow sensor
A new type of thermal sensor using polyvinylidene fluoride (PVDF) film (Dymedix Corp., Minneapolis, MN, USA) has been developed with a faster response time than those of traditional thermal devices. Thermocouples have a response time of ∼1 s, whereas the PVDF response time is on the order of 0.005 s. The signal produced by PVDF film is 150 000 times stronger than the signal produced by a thermocouple and appears to estimate changes in airflow more accurately. The PVDF signal is proportional to the difference in temperature between the two sides of the film. A single PVDF device can detect both nasal and oral flow [53, 54].
Body temperature and metabolic activity
Temperature regulation in the body can also be used to monitor sleep quality. Skin temperature increases during sleep onset and decreases during wakeup [55].
Core body temperature measured from an indwelling rectal probe provides information on the internal circadian rhythm generator (clock) [56] and gives insights on the actual circadian phase of the patient. Core body temperature is closely linked to the circadian system and its recording will allow the evaluation of delayed or advanced sleep phase problems. The normal difference between maximum and minimum body temperature in the diurnal rhythm is close to 0.5°C. Rectal or ear temperature probes are most appropriate [25]. The sleep switch device is a small device held between the index finger and thumb, the subject’s galvanic skin response closing the electric circuit being scored as wake. Subjects falling and being asleep would release the pressure from the device and open the electric circuit [57]. The Q Sensor (Affectiva, Waltham, MA, USA) is a wireless logging biosensor that measures skin conductance, skin temperature and motion comfortably from the wrist [58]. A taxonomy of autonomic sleep patterns will be developed based on electrodermal activity. Integration of movement sensors with temperature and (eventually) humidity sensors, will allow the differentiation of the sleep stages, based on new algorithms. The SenseWear BMS sensor system (BodyMedia Inc., Pittsburgh, PA, USA) is designed to continuously monitor energy expenditure, motor activity and sleep efficiency. Several sensors are incorporated into a single device that is worn on the back of the upper right arm over the triceps muscle and held in place by a Velcro armband. The sensors are a two-axis accelerometer, a heat flux sensor, a galvanic skin response sensor, a skin temperature sensor and a near-body ambient temperature sensor. Data from these parameters are used to estimate energy expenditure using proprietary equations developed by the manufacturer [59]. A simple system has been described that continuously measures the body temperature at the ear with an electronic temperature sensor that is coupled to a Bluetooth transmitter that sends the data to a mobile phone where the data are stored [60].
Smart noncontact systems
Image processing technologies and mattress sensor techniques are proposed as new respiratory monitoring techniques which do not restrain the patient.
Doppler radar technique
A potentially attractive alternative approach involves the use of a noncontact device (SleepMinder; BiancaMed, Dublin, Ireland) set up next to the patient’s bed [8]. It uses the reflection of radio waves to derive sleep, respiratory effort, body movement and even cardiac movement from a distance via a sophisticated signal analysis algorithm [61] that separates these signal components. This enables the identification respiratory events. The available data suggest this device may prove to be a useful addition to the current diagnostic armamentarium [62], with the AHI correlating strongly with PSG measurement [63].
Thermal infrared imaging
Measurement of breathing rates is feasible at a distance using thermal infrared imaging. This method is based on the presence or absence of a hot expiratory plume in the vicinity of the nostrils. When analysing the thermal imaging signal, the full breathing waveform can be extracted (rate and amplitude). Consistent segmentation of the nostril area and facial-tracking algorithms enable sustained monitoring of breathing, resulting in functionality equivalent to that of a thermistor, delivered in a contact-free manner [64]. The centrepiece of the system is a midwave infrared camera and the acquired imaging signals are processed by real-time custom software.
Passive infrared technology
The breath motion detecting system (CHR Namur, Namur, Belgium) was developed based on passive infrared (PIR) sensor technology for a contactless detection of respiratory movements. This sensor is a dual-element pyroelectric sensing device that reacts only to heat source variation (such as the movement of the human body). All objects emit infrared radiation that is invisible to the human eye but can be measured by electronic devices. When exposed to infrared radiation, the material of the pyroelectric sensor generates a surface electric charge. The term passive in this instance means that the PIR device does not emit an infrared beam but merely passively accepts incoming infrared radiation. The ideal distance appears to be 20–50 cm between the patient and the sensor. The pilot study in 169 patients demonstrated the ability of the PIR technology to detect respiratory movements in adults [65].
Fibre-grating vision sensor
A fibre-grating vision sensor is a noncontact respiratory monitoring system to detect changes in volumes by measuring the movement of laser spots on the body surface. The system measures the up-and-down motion in ≥100 sampling points on the upper half of the body and outputs the sum as respiratory movement [66]. The system is able to discriminate OSA from central sleep apnoea.
Mattress sensor technology
The static charge-sensitive mattress (BioMatt; Biorec, Turku, Finland) was developed to analyse body movements, respiration and cardiac pulses (ballistography) by recording these with a very sensitive pressure mattress that was placed underneath the actual mattress [67]. These devices were not widely adopted, except in Scandinavian countries.
Recently, a smaller (32×62×0.4 cm) electromechanical film transducer sensor (Emfit, Vaajakoski, Finland) was validated that is placed under the thoracic area of the sleeping patient. Based on advanced signal processing, respiratory effort, AHI and sleep stages could be calculated [68].
Kogure et al. [69] developed a highly sensitive pressure bed sensor that is placed under a mattress. It can identify an “in-bed/out-of-bed” state from the vibrations of the mattress. Combined with wrist actigraphy, it enables convenient long-term sleep-related evaluation.
Merilahti et al. [70] proposed the bed occupancy sensor, which consists of a thin pressure-, light- and temperature-sensitive layer used as an additional sensor to actigraphy. The use of pressure-sensitive sensors installed in a bed enables respiration monitoring during sleep, employing the combined use of a pressure sensor, and a multipoint electric sensors (polypiezofilm sensing) and pneumatics-based methods that use a thin, air-sealed cushion and a mattress. In addition, silicon rubber tubes and plastic optical fibre sensors have been proposed due to their flexibility, light weight, immunity to electromagnetic interference and ease of installation in a bed. These sensors can detect bending on an optical intensity basis [71].
Technologies based on air tubes at the same initial pressure, connected with a sensitive differential pressure sensor, were validated in a pilot study [72]. Both tubes are placed in parallel between the subject’s shoulders and hips underneath a mattress topper. The signal obtained with the sensor can be subdivided into a respiratory and a heart rate signal by means of a Butterworth bandpass filter. Additionally, the signal is processed with a differential and integration filter, followed by peak detection, which enables the detection of heart rate and breathing frequency in an unobtrusive manner [72].
Zhu et al. [73] used a similar system based on polyvinyl tubes, 30 cm in length and 4 mm in diameter, filled with air-free water preloaded at an internal pressure of 3 kPa. One end was connected to a liquid pressure sensor head, and enabled derivation of a static pressure component corresponding to the weight of the head and a dynamic pressure component reflecting changes due to respiratory motion and heart beats [73].
Several other authors have presented results on detecting heart rate and breathing rate from signals off-body, using air tubes placed below the thorax or pillow, piezopolymer sensor mats or force sensors in the bed legs [74–76]. These sensors avoid disturbing the patient during sleep and allow for long-term monitoring, even in the home setting, at the same time.
Migliorini et al. [77] performed HRV analysis and automatic sleep stage classification through bed sensors. However, commercially available pressure mats are unable to accurately reproduce indentation and deformation based on the measurement of pressure distributions.
The IdoShape (Custom8, Leuven, Belgium) is a sensor mat that detects movement and measures real deformation of the mattress surface, and can be used to evaluate the fit between the human body and its biomechanical support. The μCliMat (Custom8) sensor mat monitors temperature and humidity in a mattress system using 512 sensors, and generates thermodynamic analyses of heat flow and moisture transport (fig. 3).
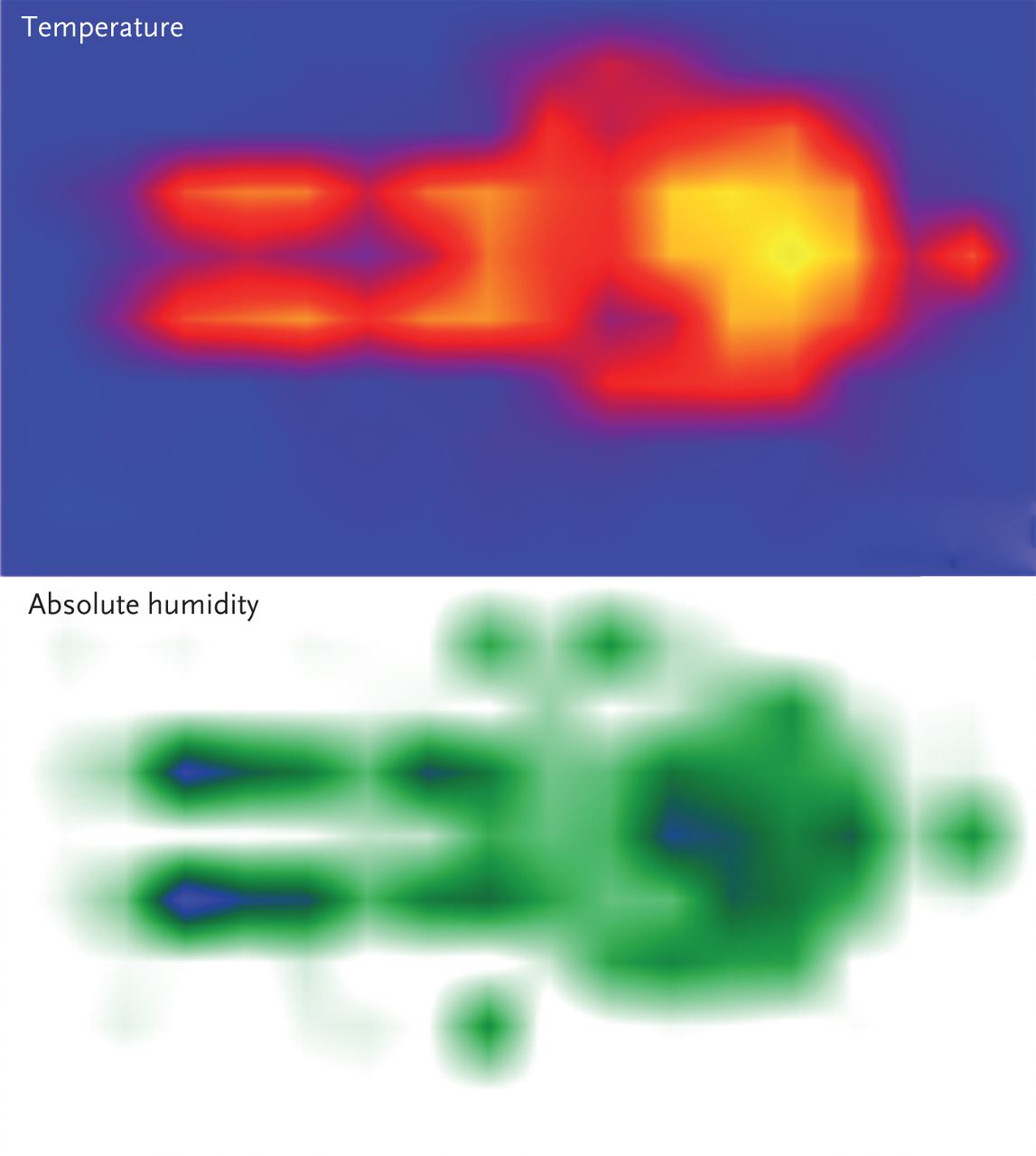
μCliMat sensor mat monitors temperature and humidity. Reproduced with permission from Custom8 (Leuven, Belgium).
Brink et al. [76] reported the application of four high-resolution force sensors installed under the bedposts. The recoil movement of the body at each heartbeat, as well as the lifting and lowering of the thorax while breathing, causes very small shifts of the centre of gravity of the bed and the subject. These shifts are reflected in the altering force distributions across the four sensors. The signals from the different load cells are combined to create a breathing signal and, again, cardiac and respiratory parameters can be calculated.
Beattie et al. [78] demonstrated the feasibility of using unobtrusive load cells installed under the bed to measure AHI. Calibrated cells can even be used to monitor a patient’s weight as well as the lying position of an individual. Similar studies with bed-installed load-cell sensors were performed to derive HRV.
Intelligent textile technology
Smart garments
Textile technology was proposed as an innovative tool for the development of devices for vital sign monitoring [79]. In particular, textile sensors can now be embedded in smart garments for collecting a variety of biological signals (ECG, bioimpedance, skin resistance, respiratory frequency, etc.). Prototypes of smart garments are available in various research laboratories around the world. For details, see the review by Lymberis and Dittmar [80]. From a methodological point of view, the development of these devices implies the minimisation of the weight and size of electronics, reduction of power consumption, and design of specific algorithms for signal conditioning. However, the most crucial issue to be addressed in dealing with smart garments is the minimisation of motion artefacts. The SD-101 (Kentzmedica Co. Ltd, Saitama, Japan) is a nonrestrictive, sheet-like medical device with an array of pressure sensors to detect SRBD by sensing gravitational alterations in the body corresponding to respiratory movements [81].
Conductive fibres
The SD-101 vest also integrates a textile-based piezoresistive plethysmograph that detects changes in the thorax circumference from which respiratory frequency is derived. This plethysmograph was obtained by a processing of the conductive fibres. Pathways made of the same conductive fibres connect the above transducers with the electronic module, which is hooked to the vest at waist level by a Velcro strip. The electronic module includes a three-axis accelerometer to detect subjects’ movements, stores data on a local memory card, and can transmit all signals via Bluetooth to an external computer for data visualisation, storage on disk and, possibly, a relay transmission through Wi-Fi or universal mobile telecommunications system connections to a remote monitoring station [79, 82].
Telemedicine
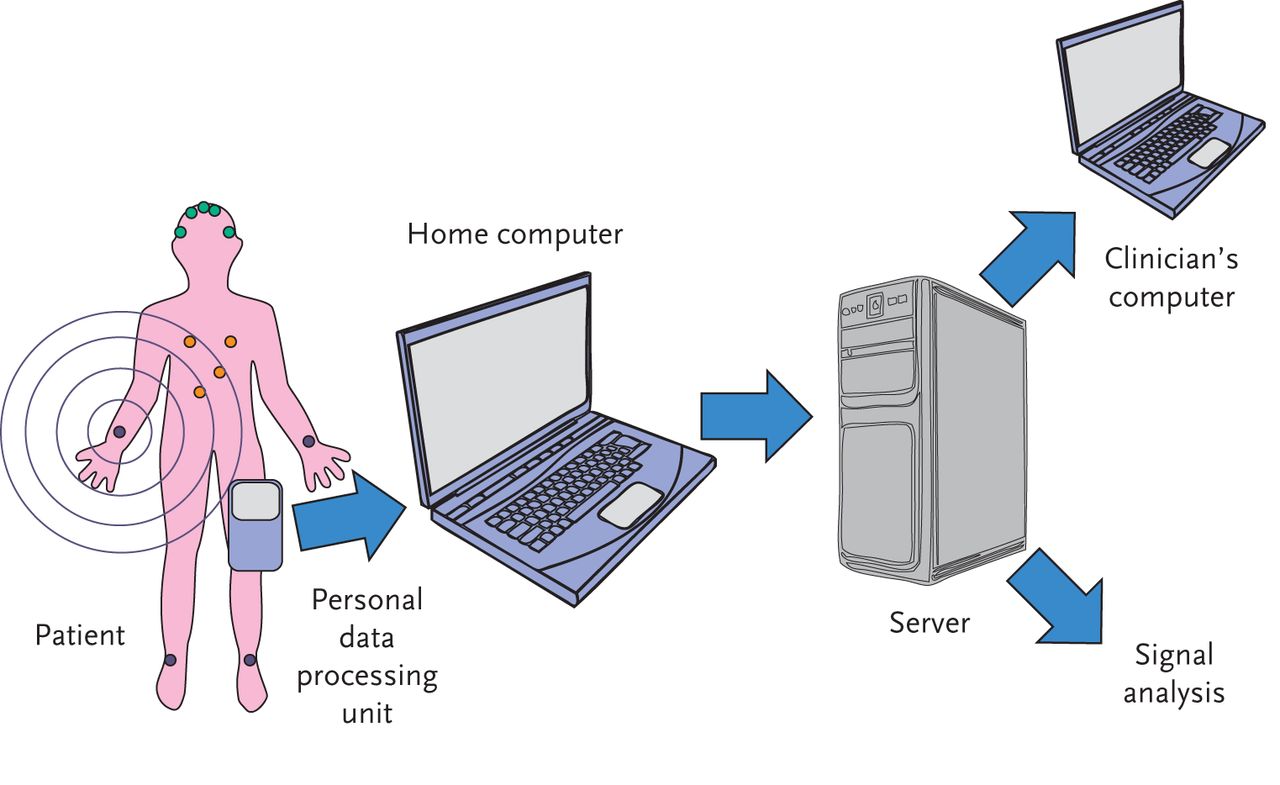
Application of telemedicine in SRBD allows support of the patient in order to improve treatment compliance, to remotely download previously recorded data [83–87] or to transmit real-time physiological parameters while the patient is sleeping (fig. 4) [88, 89]. Telemonitored PSG has the promise to overcome the disadvantages of home recordings and could provide an organisational solution to the overloading of specialised sleep centres. Technicians can regularly verify, at a distance, the quality of the PSG recordings by means of periodic access to the PSG monitoring device. From their telemonitoring control panel, they are able to insert comments in the recording, adjust transducer gain and, in the event of a technical accident, inform the patient by telephone [90]. Gagnadoux et al. [91] reported that PSG performed in a local hospital and telemonitored by a sleep laboratory was clearly superior to unattended home PSG. The major problem encountered with home sleep studies is the potential loss of data in 4.7–20% of the cases [92], which leads to less cost savings than expected. Using the Sleepbox technology (Medatec, Brussels, Belgium), which is a wireless system able to communicate with the polysomnograph and with the Internet through a Wi-Fi/3G interface, and making use of communication via Skype (Microsoft, Redmond, WA, USA), the authors were able to deliver recordings of excellent quality in 90% of the cases. Pelletier-Fleury et al. [90] comparatively evaluated the cost and effectiveness of PSG telemonitoring and PSG by conventional unsupervised home monitoring, demonstrating that remote telemonitoring made the procedure clearly superior from a technical point of view and was preferred by the patients. They calculated a cost of USD 244 for PSG telemonitoring, whereas the PSG with conventional unsupervised home monitoring cost USD 153. Healthcare infrastructure savings also have to be taken into account. If we add up, for instance, the travelling costs avoided by the patients and the working days that they did not lose, we could estimate that the real cost would be similar to or lower than that of conventional PSG [93]. In any case, remote monitoring opens an interesting perspective to decrease the failure rate of home sleep studies. Kristo et al. [94] presented a telemedicine protocol for the online transfer of PSGs from a remote site to a centralised sleep laboratory. Their system was based on the transmission of data using FTP (file transfer protocol). Seo et al. [95] developed a nonintrusive home-based health-monitoring system to monitor patients’ ECG results, weight, movement pattern and snoring. Choi et al. [96] presented a ubiquitous health monitoring system in a bedroom, which monitors ECG, body movements and snoring with non-conscious sensors. A centralised framework is used in most home telehealth systems, in which a centralised database is used for data storage and analysis [97]. In 2008, Kayyali et al. [98] proposed a new compact telemetry-based sleep monitor (PSG@Home), consisting of a 14-channel wearable wireless monitor and a mobile phone-base gateway to transfer data, including video, in real time from the patient’s home to a remote sleep centre. The receiver is a separate unit attached to the back of the display. Internal Bluetooth receivers, often included in many laptops, can also be used instead of a dedicated external Bluetooth receiver.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Model for telemonitoring in sleep medicine. Data flow is initiated at the body area network of sensors on the left and eventually reaches the clinician’s workstation on the right.
Mobile telephones
Mobile telephones are a very attractive application platform, as most of them incorporate a lot of interesting characteristics, namely computing power, long battery life, many built-in sensors and wireless connectivity. Mobile applications may also simplify sleep diagnostics by using a smartphone’s built-in sensors. The parameters that can be measured by such applications are breathing pattern and movement patterns, which are recorded using the built-in microphone and accelerometer, respectively. Consequently, the recorded data are sent to a server for analysis in dedicated software like MATLAB (MathWorks, Natick, MA, USA) in order to diagnose patients [99]. Sleep Cycle (Maciek Drejak Labs, Gothenburg, Sweden) is a popular iPhone (Apple Inc., Palo Alto, CA, USA) “app” that uses the accelerometer in the iPhone to monitor body movements and determine the user’s sleep stage. The user just needs to put the iPhone in a suitable place on the bed. However, the iPhone can accidently fall off the bed and it needs to be connected to the charger for the whole night. Tablet computers or mobile telephones also enable an online signal check by sending a screenshot of the recording. Transfer times and periods can be programmed individually.
Conclusions
Traditional sleep monitoring methods use a variety of leads and probes on the patient’s face and body to gather data. Additional information can be achieved from these signals by advanced processing based on complex algorithms. Moreover, a number of signals that are not traditionally used in clinical PSG will become of interest for specific patient categories. We are also faced with the development of innovative noncontact systems based on movement detection using radar and infrared technology. The idea of automatic sleep evaluation and monitoring through signals that are integrated into the environment (a sensorised bed) or through wearable textile technology will change the traditional paradigm of clinical polysomnography. Implementation of wireless applications and remote monitoring will lead to new platforms and evolve towards low-threshold sleep telemedicine. The available evidence base has, however, lagged far behind.
Footnotes
Statement of Interest
J. Verbraecken has acted as a consultant for Takeda and has received payments for lectures including service on speakers bureaus from AstraZeneca, Ikaria, NVKVV, Therabel Pharma, Estée Lauder and Philips. He has received payment for development of educational presentations and for contribution to ERS Buyers Guide from the European Respiratory Society.
A version of this article appeared in the ERS Buyers' Guide 2013/2014 under the title “Evolving technologies to study sleep and respiration: finding the dream”.
- ©ERS 2013
References










