





Case
A 21-year-old male with Ehlers-Danlos type IV (EDS IV) presented to the emergency department with sudden onset right-sided pleuritic chest pain.
On examination, some of the typical features of EDS IV including large eyes and small chin were noted, although other features such as sunken cheeks, thin nose and lips, and lobeless ears were not noted [1]. His respiratory rate was 20 breaths·min−1, saturations were 93% on air increasing to 98% on 28% oxygen via a venturi mask. Pulse was 115 beats·min−1 in sinus rhythm and his blood pressure was 112 over 64 mmHg.
There was decreased air entry in the right hemithorax, with decreased vocal resonance. The trachea was central and there was no surgical emphysema.
Task 1
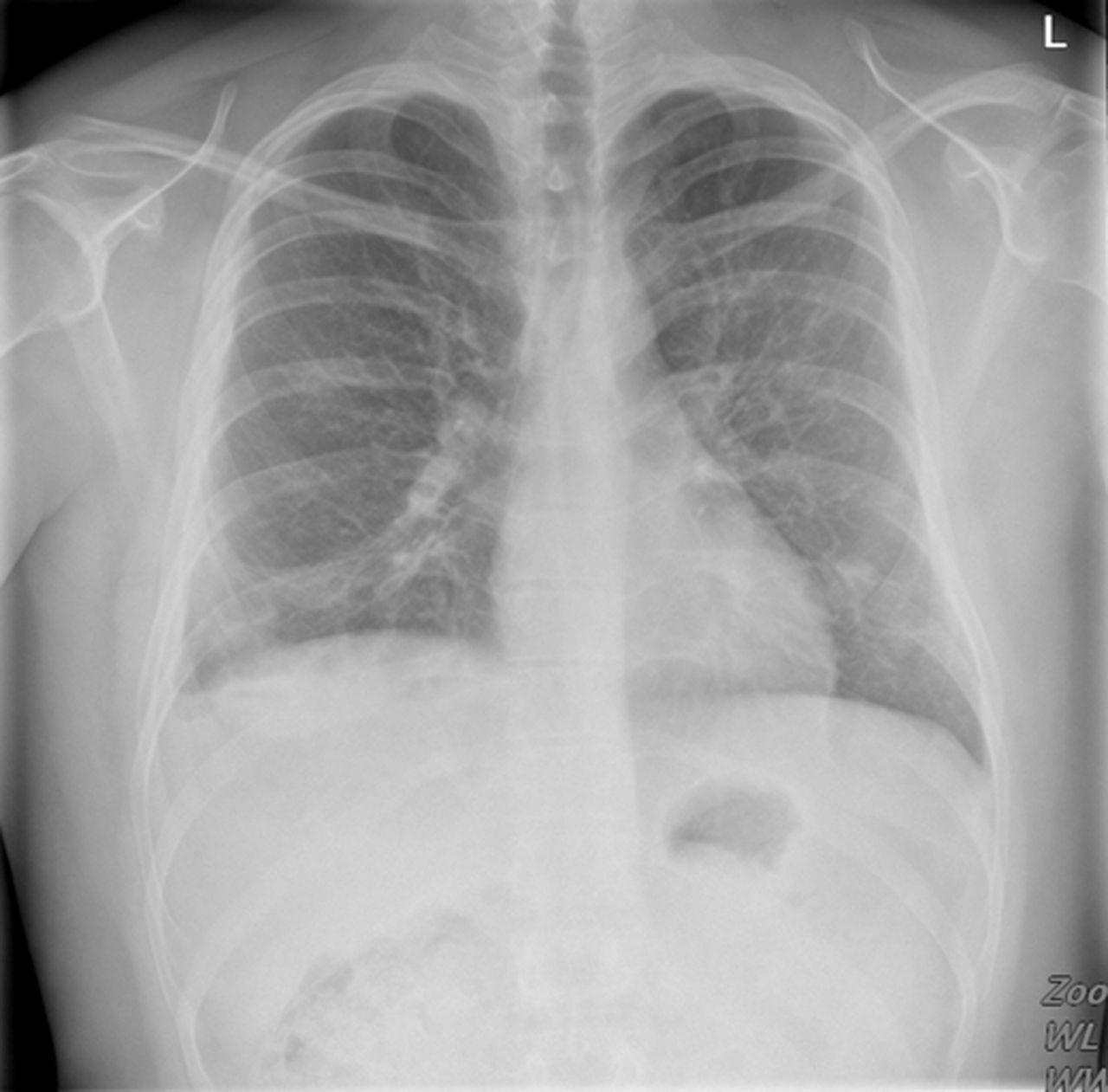
1. What is the best description of the chest radiograph (fig. 1)?

Chest radiograph on admission.
-
A right-sided tension hydro-pneumothorax
-
A right-sided hydro-pneumothorax
-
A right-sided cavitatory pneumonia
-
A right-sided pneumo-peritoneum
2. What would the next therapeutic step be?
-
Simple observation and high flow oxygen
-
Aspiration of pneumothorax
-
Insertion of a small 12-French bore Seldinger chest drain
-
Insertion of a large-bore chest drain
Answer 1
The chest radiograph shows a right-sided hydro-pneumothorax and the next therapeutic step would be insertion of a small 12-French bore Seldinger chest drain.
Local anaesthetic was instilled into the second intercostal space and it was possible to aspirate air via the green needle. A 12 French intercostal drain was inserted using the Seldinger technique with no immediate complications and connected to an underwater seal bottle which immediately began to bubble.
British Thoracic Society guidelines [2] advocate the insertion of small-bore chest drains for primary pneumothoraces and that was the initial diagnosis.
As the drain was being sutured, 50 mL of blood poured into the bottle.
The patient remained haemodynamically stable and oxygen saturations were 99% on 28% via a venturi mask.
Task 2
What is the next appropriate step in the clinical management?
Answer 2
An urgent computed tomography(CT) scan
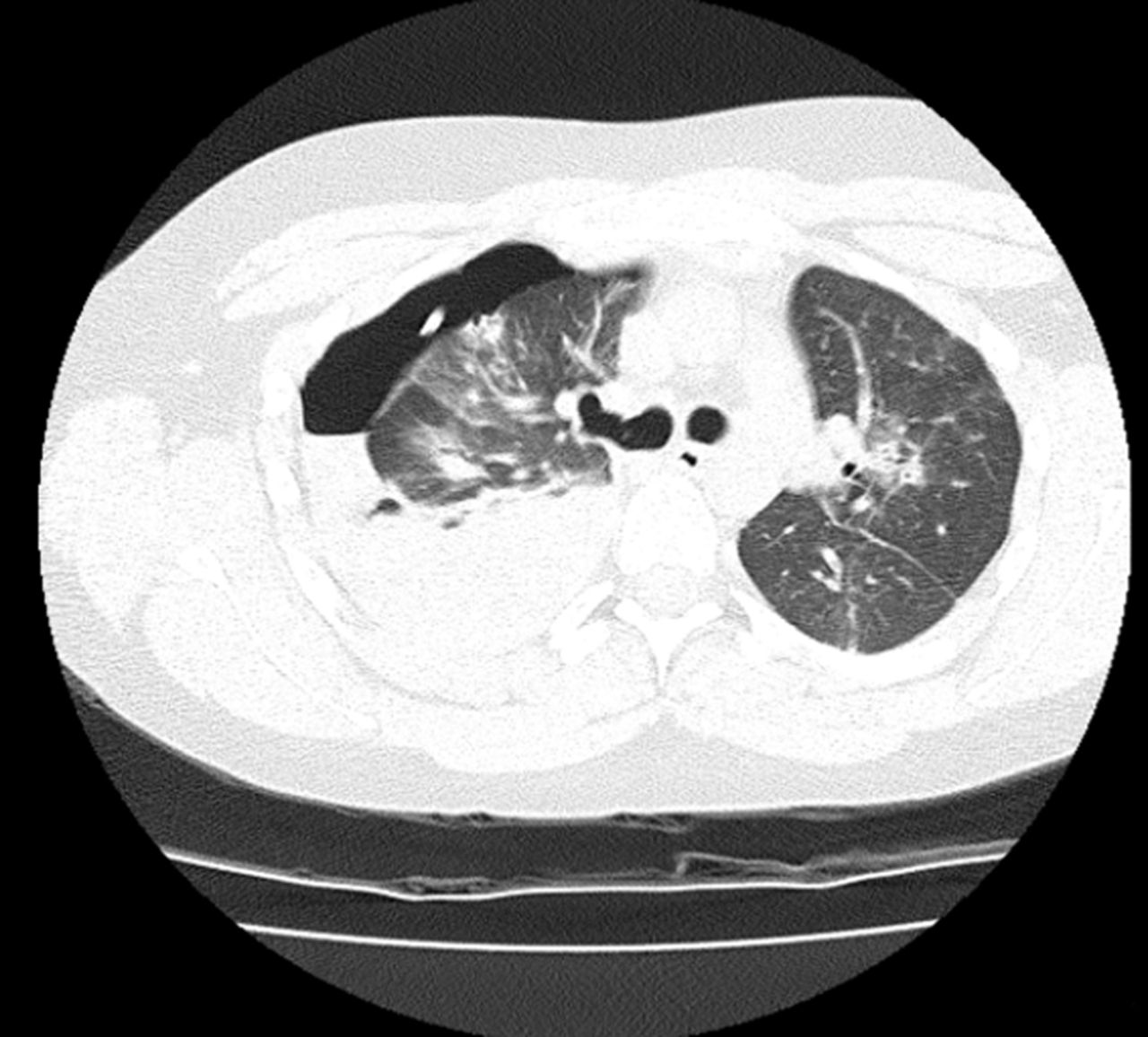
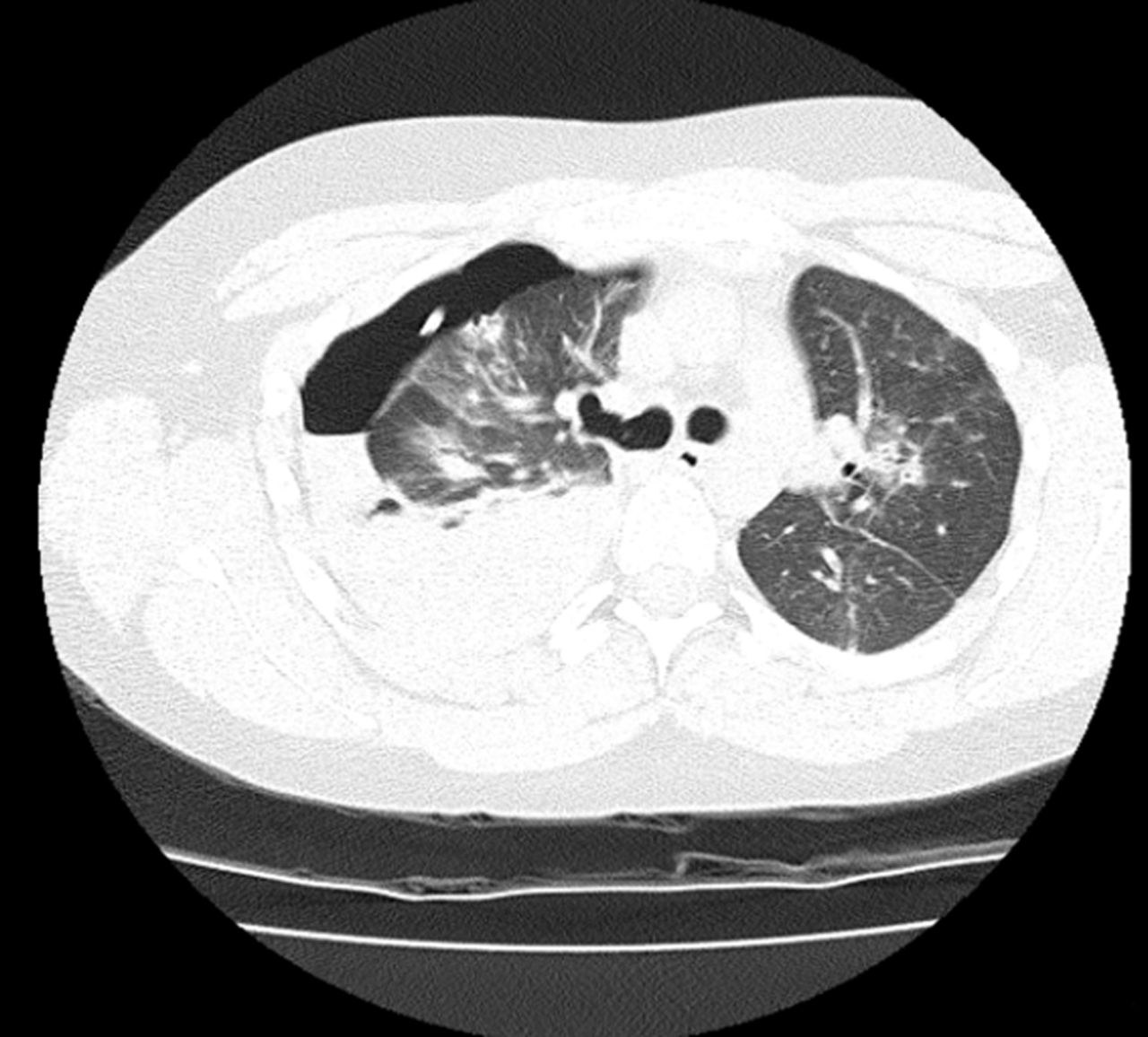
CT scans were performed and the images are shown (figs 2–6).

High-resolution CT image

High-resolution CT image

Mediastinal CT image
High-resolution CT image

Mediastinal CT image
Task 3
What do the CT images show? (fig. 2–6)
-
Right pleural fluid of high attenuation
-
Puncture of the right subclavian artery
-
Right pneumonia with empyema
-
Multiple pulmonary metastases metastases
Answer 3
a) Right pleural fluid at high atteniation
The report of the CT scan confirmed that the seldinger chest drain was in the right-sided pleural space, through the midline anteriorly into the first intercostal space. It avoided all major thoracic vessels, including the right subclavian, and right internal mammary arteries.
There was a large right-sided mixed attenuation pleural fluid collection, consistent with haemorrhage. No obvious bleeding point was identified. A moderately large right anterior pneumothorax was seen with mediastinal shift to the left. Patchy nodular consolidation throughout both lungs was demonstrated, worse on the right. Multiple right-sided bullae were noted.
A cardiothoracic opinion was sought and the insertion of a large-bore chest drain advised. After subsequent review by a respiratory specialist, in the absence of any haemodynamic compromise, and with the patient's symptoms having improved, the small-bore drain was left in. There was now only minimal drainage of blood into the underwater seal bottle.
Due to the nature of his underling connective tissue disease, consensus opinion was sought from local and international experts who all agreed that his subsequent management should involve the least invasive procedures possible given the inherent increased risk of bleeding.
His admission was complicated by the development of haemoptysis which settled with anti-fibrinolytics and antibiotics. Surgical emphysema then ensued which improved with ongoing drainage and suction. The drain was removed upon cessation of bubbling and when there was no change in the clinical and radiological picture upon clamping. The patient was discharged with early follow up and the pneumothorax resolved slowly over a period of a few months. Follow-up CT images are shown (figs 7 and 8).

Chest radiograph at follow-up

High-resolution CT image at follow-up
Answer 4
The most recent shows complete resolution of any pneumothorax as well as of the cavitatory lesions, with negligible residual pleural thickening.
Discussion
Ehlers–Danlos syndrome (EDS) represents a heterogeneous group of generalised connective tissue disorders resulting from defects in collagen synthesis and/or processing. They can present with a triad of joint hypermobility, hyper-elasticity of the skin and fragility of the skin and blood vessels. Symptoms can include back pain, easy bruising, flat feet, easy scarring and poor wound healing, joint dislocations, vision impairment and rupture of major organs.
Type I and II of EDS, also known as classical EDS, have an autosomal dominant inheritance and have a predominant skin involvement. Type III (hypermobility syndrome) is either autosomal dominant or recessive, and mainly causes joint laxity. Types VI, VIIA, VIIB and VIIC are all very rare and respectively cause kyphoscoliosis, joint dislocations and extreme skin fragility and sagging [3].
Type IV EDS (ED4) or the vascular type is caused by an autosomal dominant defect in type 3 collagen synthesis affecting the COL3A1 gene, affecting approximately 1 in 100,000–250,000 people.
Histology of structures show arterial wall thinning, reduced collagen content and a distorted architecture [4, 5]. This leads to spontaneous haemorrhages, cerebral, gastro-intestinal, uterine and pulmonary, from aneurysmal degenerations or arterial tears.
20 patients with EDS (10 type 1, six type II and four type IV were studied by Ayres et al. [6]. Haemoptysis occurred in 25%, two patients with EDS IV had bullous lung disease and one had three pneumothoraces and associated tracheomegaly. A follow-up study by Oderich et al. [7] of 31 patients (15 male and 16 female) over 30 years showed 24 patients developed 132 vascular complications, with 15 patients needing surgery. Within these patients, three deaths occurred from massive haemorrhage, with a 37% occurrence of post-operative bleeding and a 20% rate of re-exploration due to bleeding. Such incidents shortened life and as such, it is recommended that a more conservative approach to bleeding should be adopted, although the clinician should take into account the unique clinical picture and assessment of such a patient.
The presentation and CT scan findings in this case are in keeping with what has previously been described in patients with EDS IV with respect to their pulmonary manifestations. Herman and McAlister [8] described an 18-year-old patient with EDS IV with recurrent large, thick-walled lung cavitatory lesions, due to focal lung rupture. Wanatabe et al. [9] described a 16-year-old female with haemoptysis, cavitatory lesions and a heamothorax. Fragility of lung tissue was demonstrated on lung biopsy which showed almost absence of lung tissue.
Intervention in patients with EDS IV requires careful and individual assessment of risks versus benefits. A minimally invasive approach should ideally be adopted due to increased risk of haemorrhagic complications. In this case the presence of mediastinal shift warranted early intervention but a more conservative approach was warranted when the pneumothorax was slow to resolve. We have demonstrated a good outcome in with this approach.
It is recommended that patients with EDS IV should carry a European Ehlers–Danlos syndrome passport, which explains their clinical condition and the potential vascular complications as well as documenting their blood group [10].
Footnotes
Statement of Interest
S. Doe has traveled to the European CF Society conference with Novartis who arranged travel and accommodation.
The ERS designates this educational activity for a maximum of 1 CME credit. Please visit www.ers-education.org/e-learning/cme-tests.aspx formore information.
- ©ERS 2013











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}