Predictors of Mortality in Neonates and Infants Hospitalized With Sepsis or Serious Infections in Developing Countries: A Systematic Review
 Li(Danny) Liang1
Li(Danny) Liang1  Naima Kotadia2
Naima Kotadia2  Lacey English3
Lacey English3  Niranjan Kissoon4,5
Niranjan Kissoon4,5  J. Mark Ansermino5,6,7
J. Mark Ansermino5,6,7  Jerome Kabakyenga8,9
Jerome Kabakyenga8,9  Pascal M. Lavoie10
Pascal M. Lavoie10  Matthew O. Wiens5,6,9*
Matthew O. Wiens5,6,9*- 1Faculty of Medicine, University of Toronto, Toronto, ON, Canada
- 2Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
- 3School of Medicine, University of North Carolina, Chapel Hill, NC, United States
- 4Department of Pediatrics, University of British Columbia, Vancouver, BC, Canada
- 5Center for International Child Health, British Columbia Children's Hospital, Vancouver, BC, Canada
- 6Department of Anesthesiology, Pharmacology and Therapeutics, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
- 7Department of Anesthesia, British Columbia Children's Hospital and University of British Columbia, Vancouver, BC, Canada
- 8Maternal Newborn and Child Health Institute, Mbarara University of Science and Technology, Mbarara, Uganda
- 9Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
- 10Division of Neonatology, Department of Pediatrics, University of British Columbia, Vancouver, BC, Canada
Background: Neonates and infants comprise the majority of the 6 million annual deaths under 5 years of age around the world. Most of these deaths occur in low/middle income countries (LMICs) and are preventable. However, the clinical identification of neonates and infants at imminent risk of death is challenging in developing countries.
Objective: To systematically review the literature on clinical risk factors for mortality in infants under 12 months of age hospitalized for sepsis or serious infections in LMICs.
Methods: MEDLINE and EMBASE were systematically searched using MeSH terms through April 2017. Abstracts were independently screened by two reviewers. Subsequently, full-text articles were selected by two independent reviewers based on PICOS criteria for inclusion in the final analysis. Study data were qualitatively synthesized without quantitative pooling of data due to heterogeneity in study populations and methodology.
Results: A total of 1,139 abstracts were screened, and 169 full-text articles were selected for text review. Of these, 45 articles were included in the analysis, with 21 articles featuring neonatal populations (under 28 days of age) exclusively. Most studies were from Sub-Saharan Africa and South Asia. Risk factors for mortality varied significantly according to study populations. For neonatal deaths, prematurity, low birth-weight and young age at presentation were most frequently associated with mortality. For infant deaths, malnutrition, lack of breastfeeding and low oxygen saturation were associated with mortality in the highest number of studies.
Conclusions: Risk factors for mortality differ between the neonatal and young infant age groups and were also dependant on the study population. These data can serve as a starting point for the development of individualized predictive models for in-hospital and post-discharge mortality and for the development of interventions to improve outcomes among these high-risk groups.
Introduction
Significant progresses have been made over the past two decades in reducing global under-5 mortality from 91 deaths per 1,000 live births in 1990 to 43 deaths per 1,000 live births in 2015 (1). However, mortality in neonates (under 28 days of age) and infants (under 1 year of age) remains disproportionately high, representing over two-thirds of under-5 deaths in children below 5 years of age (2). Of these deaths, 90% occur in developing countries (3), with the highest neonatal mortality rates occurring in Sub-Saharan Africa. Thus, interventions among neonates and infants are urgently needed in these countries if the recent UN Sustainable Development Goals are to be achieved, targeting to decrease under-5 mortality to < 25 per 1,000 live births and neonatal mortality to < 12 per 1,000 live births by 2030 (4, 5).
Reducing mortality in neonates and young infants has lagged significantly behind that of older pediatric populations (6). Although no consensus has been made, some studies suggest preterm birth, intrapartum complications, and sepsis are leading causes of death among neonates (7). The relative risk of death from these events ranges from 10 to 36 times greater in LMICs, as compared to high income countries (3).
A population-based health survey in 56 countries from 1990 to 2002 identified main factors contributing to infant mortality around the world, including first births, shorter birth interval, male sex, gestational multiplicity, and rural setting (8, 9). Infants of mothers with less education or who lived further away from health care resources were also at greater risk of death (8, 9).
However, in spite of this knowledge, our ability to develop effective interventions for this age group remains limited, as causes of death are multi-factorial and often involve a greater social context. Published systematic reviews have attempted to discern more age-specific factors, but these studies have largely focused on high resource settings (10). Given that the greatest burden of neonatal and infant deaths occur in LMICs, this is an important limitation (11). Finally, underserved populations tend to have limited research, making the benefits of systematic reviews in the identification of gaps in these cases all the more impactful (12, 13).
The objective of this systematic review was to develop an evidence base of studies assessing risk factors for mortality among newborns and infants who are hospitalized in LMICs. The focus of this literature review was serious infections and sepsis, as they are the most commonly identified, and potentially highly preventable (14), causes of neonatal and infant deaths in LMICs.
Methods
Study Eligibility Criteria and Systematic Search
This systematic review focused on children < 1 year old evaluated for sepsis or other serious infections in LMICs. Study eligibility was defined according to the conventional Populations, Interventions, Comparators, Outcomes, and Study Design (PICOS) criteria, determined a priori (Table 1).
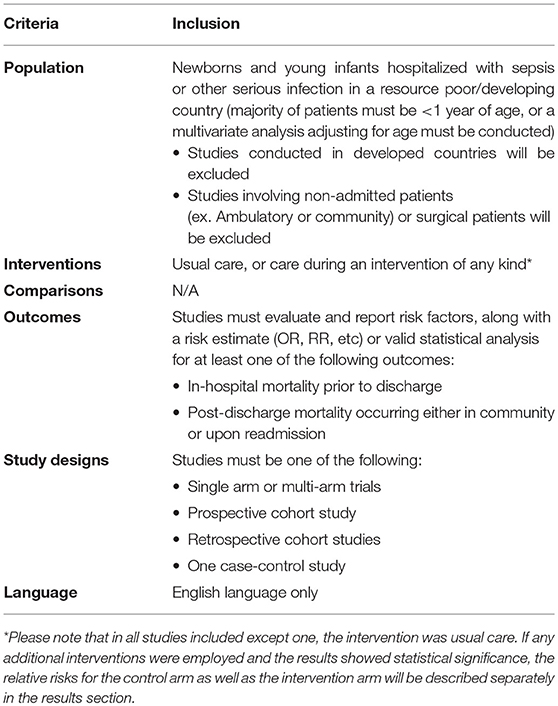
Table 1. PICOS criteria outlining study eligibility.
A study was included if (i) it presented original data from either a prospective or retrospective cohort study or from a randomized controlled trial, (ii) the majority of the subjects were under 1 year of age or a multivariate analysis adjusting for age was conducted, or a subgroup analysis for specific mortality risk factors was collected for patients < 1 year old, (iii) the study was conducted in a developing country (defined as countries classified by the United Nations Development Program (UNDP) in its 2016 report as having a low or medium Human Development Index (15)), and (iv) published in English.
Studies were excluded if (i) some or all of the patients were not admitted (ex. ambulatory or community health facilities), (ii) it represented a surgical population since mortality risk factors for surgeries would likely differ from those of acute illness, or (iii) the study population included nosocomial infections (Table 1).
MEDLINE and EMBASE databases were searched with the assistance of a medical librarian (Appendix 1 and Appendix 2), using the Ovid platform. The search dates were from database inception to April 2017.
Study Selection and Data Extraction
Two investigators (LL and NK) independently conducted two rounds of review to determine study eligibility among identified articles. Articles were first screened based on the abstract using the PICOS criteria defined in Table 1, where articles clearly meeting exclusion criteria were immediately discarded. A second round of review involved screening the remaining manuscripts in full text, to determine final eligibility. At both stages, discrepancies were resolved by consensus or by arbitration by a third investigator (MW).
For all included articles in the analysis, the following study characteristics were extracted, including: country/region, study period, study design, study population, number of subjects, number of deaths, proportion of participants under 12 months and under 1 month of age, type of analyses conducted for risk factors (i.e., multivariate vs. univariate) and length of post-discharge follow-up. All variables included in the mortality risk factor analyses were recorded. If both univariate and multivariate analyses were performed, only the results from the multivariate analysis were recorded. Data extraction was completed by one investigator and checked by a second investigator for accuracy and consistency.
Outcomes and Data Analysis
The primary aim of this systematic review was to determine the risk factors for mortality among neonates and infants hospitalized with an infectious process in developing countries. All risk estimates pertain to in-patient mortality, except those specifically noted as risk factors for outpatient (i.e., post-discharge) mortality.
As all studies were interpreted from a cohort design perspective, their quality was assessed using the Newcastle-Ottawa Scale (16). Each study was reviewed by one investigator (LE) for criteria related to selection, comparability, and outcome assessment.
Due to expected heterogeneity in study population, risk factors and analysis, it was determined a priori that formal meta-analysis would not be conducted. The primary form of analysis was therefore descriptive and conducted using Microsoft Excel (Redmond, WA). Studies were grouped according to both participant age group (neonatal vs. infant) and underlying population (i.e., disease etiology).
Results
Summary of Included Articles
Through the systematic literature search, 1,139 abstracts were identified. Of these, 970 were excluded during the abstract screening stage. The full-text of the remaining 169 articles were reviewed, after which an additional 124 articles were excluded. Thus, a total of 45 articles were included (Figure 1) (17–62).
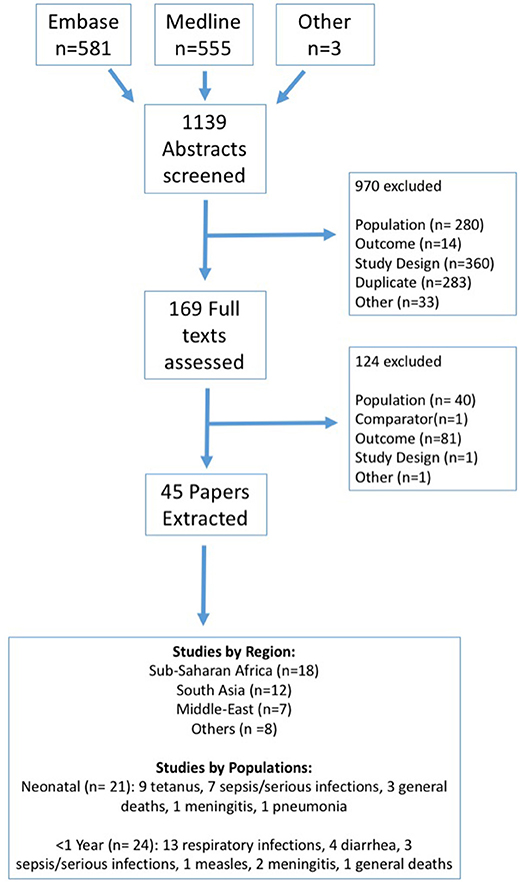
Figure 1. Systematic review flowchart.
Among these 45 studies, the majority of studies were prospective or retrospective cohort studies (Tables 3, 4). Upon assessment using the Newcastle-Ottawa scale, the average score for included studies was 6.3 out of 9 stars, based on selection criteria, comparability of cohorts, and assessment of outcomes encompassing attrition. Included studies were found to have low comparability, with only 40% controlling for confounders in the study design or statistical analysis. Approximately 70% of studies chose representative samples and reported reliable inclusion criteria.
Among the 45 included studies, multiple geographic regions were represented: 18 from Sub-Saharan Africa, 12 from South Asia, 7 from the Middle-East and 8 from other regions (Table 2). Twenty-one (46.6%) focused exclusively on the neonatal populations, whereas the other 24 studies (53.3%) focused on children under 1 year of age (Table 2). Nearly all of the studies (n = 42, 93.3%) focused exclusively on in-hospital deaths, while two (4.4%) studies focused exclusively on post-discharge death and one study (2.2%) on both in-hospital and post-discharge death. Seventeen (37.8%) of the included studies were published before 2000. The median number of study participants was 201 children (IQR 102-697).
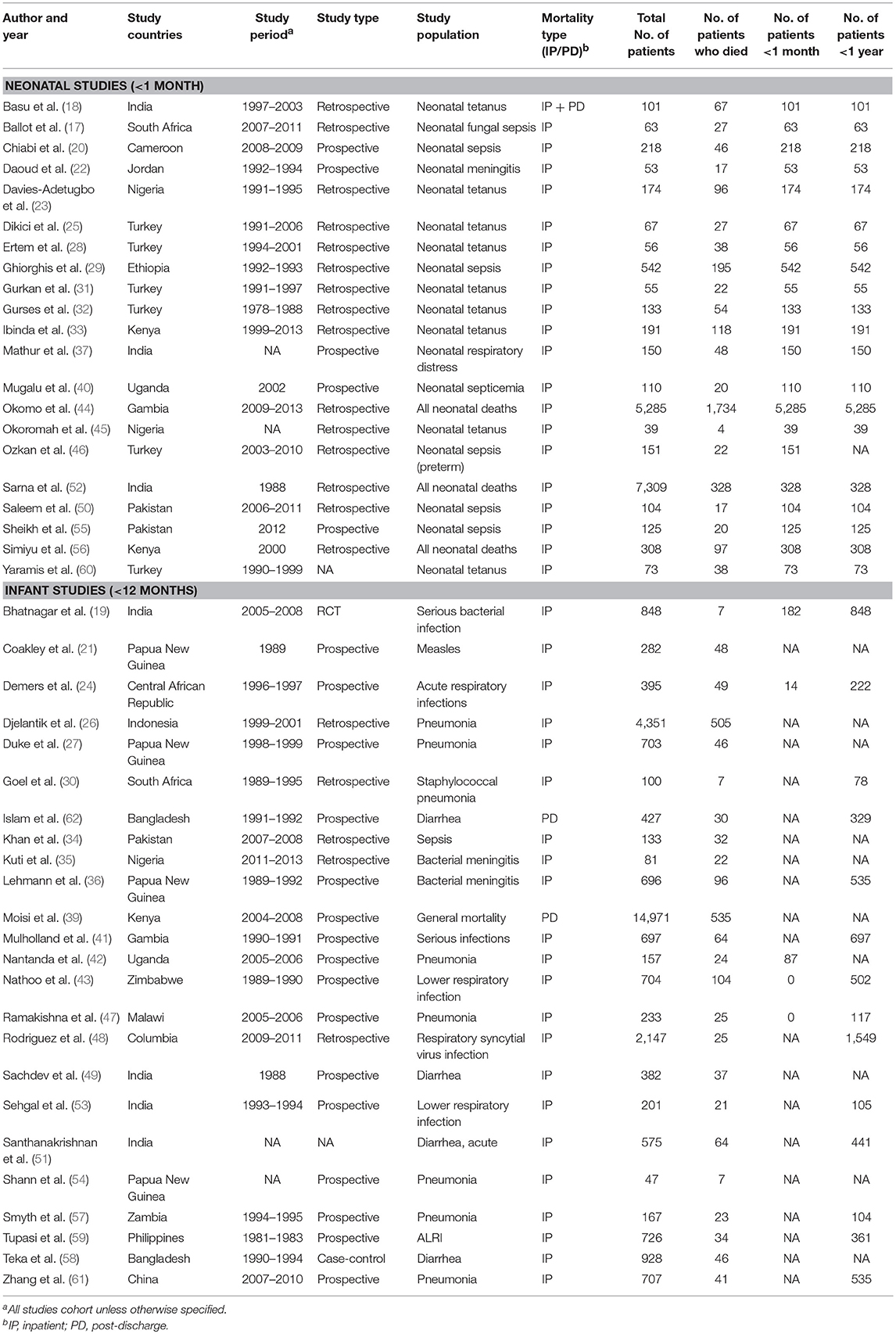
Table 2. Study characteristics.
Among 21 neonatal studies, nine focused on tetanus, seven on sepsis, one on meningitis, one on respiratory infections, and three on general admissions (Table 2). Among the 24 infant studies, 13 focused on children with respiratory infections. The remaining focused on diarrhea (n = 4), sepsis or serious infections (n = 3), meningitis (n = 2), measles (n = 1) and general admissions (n = 1; Table 2). Key results, along with definitions for all parameters, are highlighted in Tables 3, 4. For each illness, the most common risk factors, prioritized by frequency, are presented in these tables to ensure conciseness. Risk factors discussed only in a single study were not included in these tables, but are reported in the Supplementary Table 1.
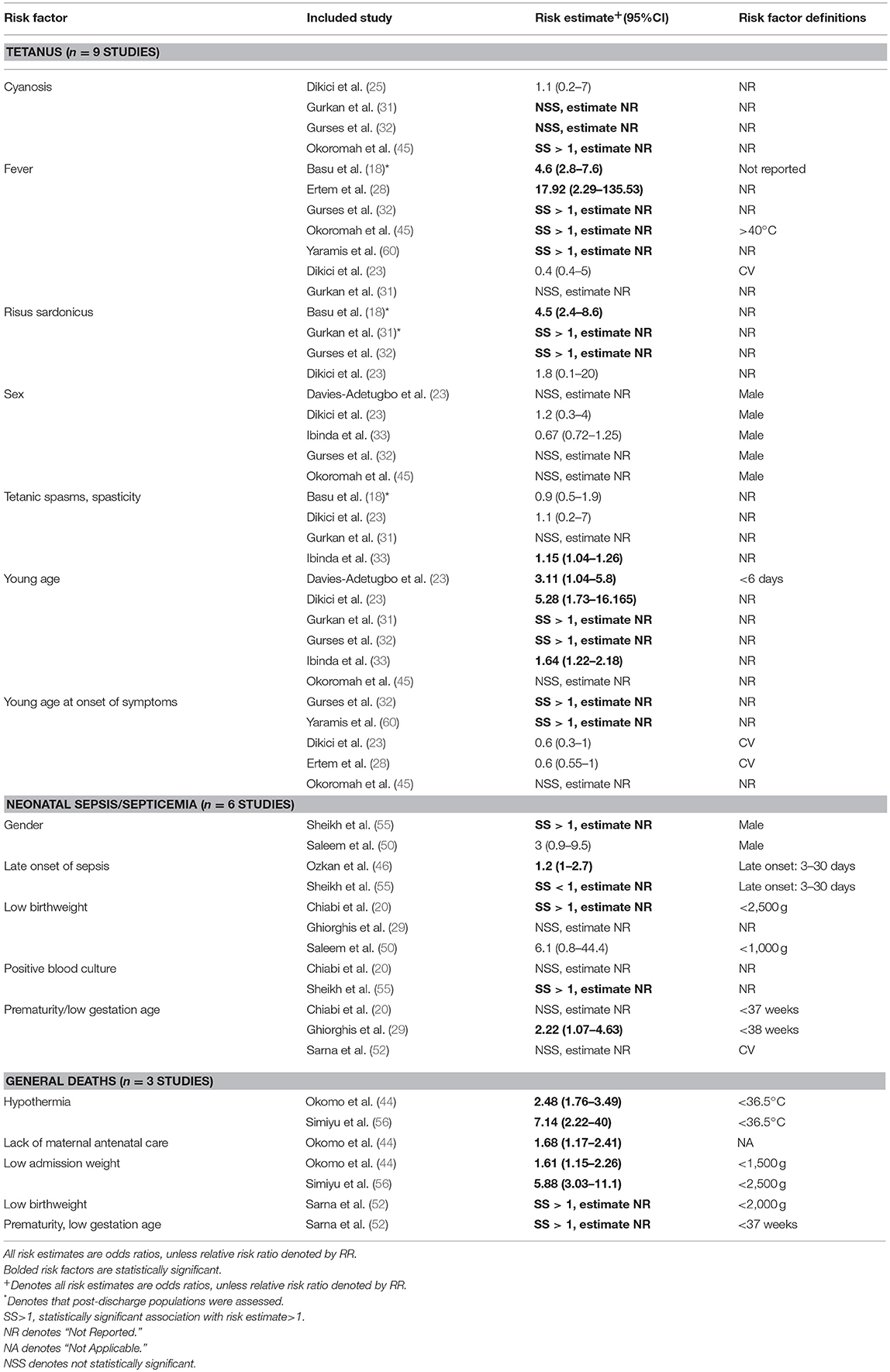
Table 3. Summary of risk factors for neonatal mortality by underlying disease.
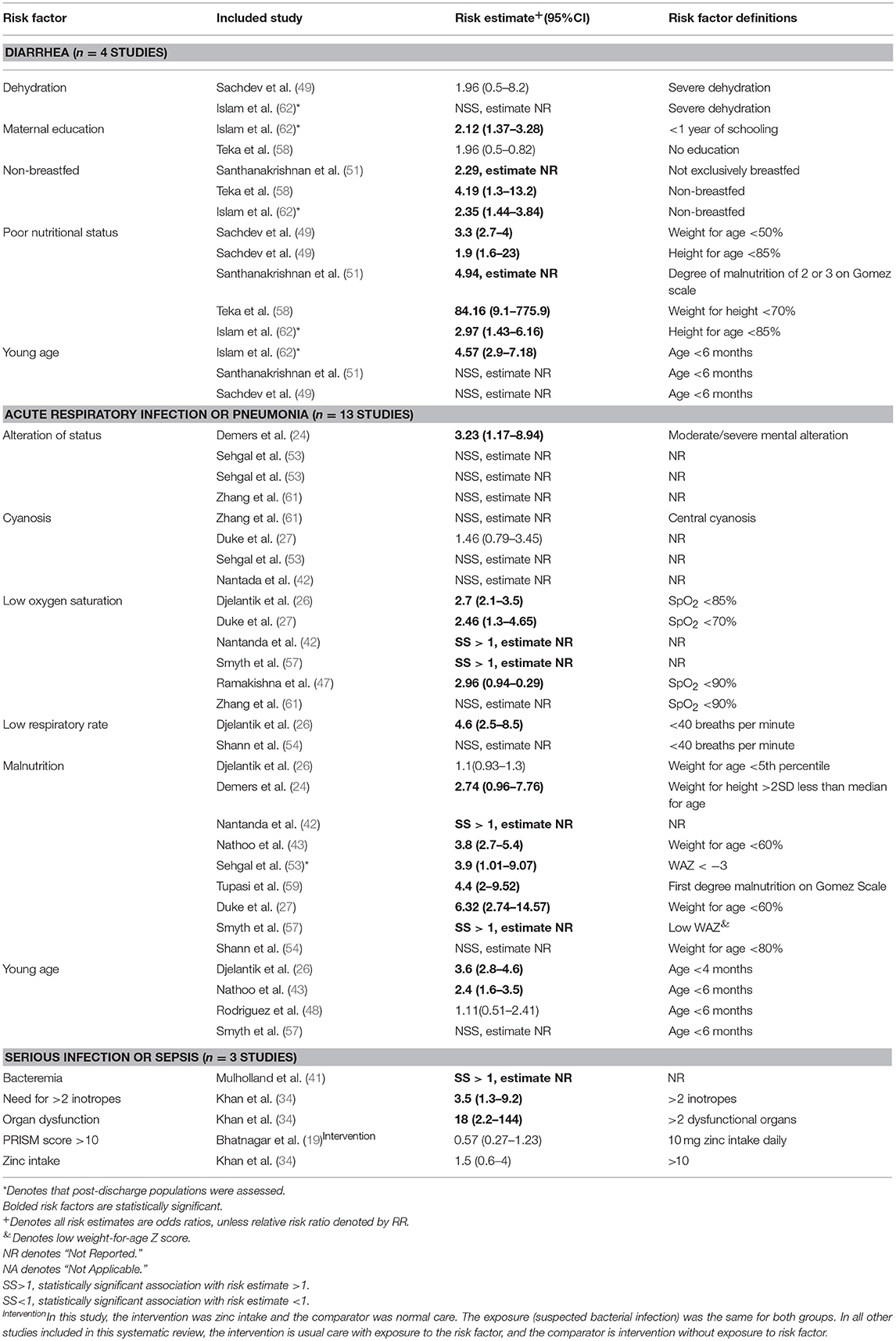
Table 4. Summary of risk factors for infant mortality by underlying disease.
Neonatal Mortality
Tetanus
A total of nine studies evaluated predictors of mortality for neonatal tetanus. Mortality rates ranged from 10.3 to 67.9% in these studies. The most consistent predictors of mortality were young age of presentation and onset, presence of fever and risus sardonicus. For young age at presentation, the adjusted odds ratios ranged from 1.64 (95% CI: 1.22–2.18) to 5.29 (95% CI: 1.73–16.17). The presence of fever was associated with increased odds of mortality, ranging from 4.6 (95% CI: 2.8–7.6) to 17.92 (95% CI: 2.29–135.53). Three of the five studies reported fever as a statistically significant variable, but did not provide odds ratios. The odds of mortality among patients with risus sardonicus study were 4.5 (95% CI: 2.4–8.6) in one study. Two studies also found risus sardonicus and young age of onset to be significantly associated with mortality, although specific values were not provided.
Variables frequently assessed as potential risk factors, but which consistently showed no association with mortality in this population included sex, tetanic spasms/spasticity, umbilical inflammation, sepsis, trismus, maternal tetanus immunization status, lack of sucking, omphalitis, irritability, high heart rate and high respiratory rate.
Sepsis/Serious Infections
Seven studies evaluated mortality among populations of neonates with sepsis or severe infection. Mortality rates were very high, ranging from 14.6 to 36.0% of admitted patients. Prematurity and low birth weight were significantly associated with mortality in two studies for each of these factors. The odds ratio for prematurity was 2.22 (95% CI: 1.07–4.63) for one study and not given for another study. Similarly, the odds ratio for low birth weight was 6.1 (95% CI: 0.8–44.4) in one study and not given for another study. Platelet count, weight at presentation, sex and white blood cell counts did not show statistically significant correlations with mortality in these studies.
General Hospital Admissions
Three studies assessed mortality among general neonatal hospital admissions. These studies have included neonatal populations with diarrhea, malaria, pneumonia, jaundice, convulsions, soft-tissue infections, asphyxia, tetanus, omphaitis, congenital malformations, intrapartum abnormalities and hypothermia. Low admission weight and hypothermia were found to be statistically significant predictors of mortality in both studies in which they were assessed. The odds of mortality for children with low admission weight was 1.61 (95% CI: 1.15–2.26) and 5.88 (95% CI: 3.03–11.1), and for children with hypothermia was 2.48 (95% CI: 1.76–3.49) and 7.14 (95% CI: 2.22–40). Maternal age, sex and time of day at presentation were not significant correlates of mortality in these studies.
Other Studies
In the single study assessing mortality among neonates with meningitis, a bulging anterior fontanelle was the only significant predictor of mortality, with an odds ratio of 7.7 (95% CI: 1.7–35.4). Hypothermia, feeding difficulties, jaundice, cyanosis, vomiting, convulsions and respiratory distress showed no significant correlation with mortality among meningitis patients. It is worth mentioning that the above study only contained a total of 17 deaths, so was likely underpowered. In the single study focused on respiratory infections among neonates, an alveolar-arterial carbon dioxide gradient (AaCO2 gradient) >250 mmHg was the only statistically significant predictor of mortality, with an odds ratio of 71.1 (95% CI: 1.1–4,395). Weight, gestational age, lethargy, age at presentation, pH < 7.2, absent neonatal reflexes, shock, fraction of inspired oxygen (FiO2), blood base excess, blood culture, C-reactive protein level, arterial alveolar oxygen ratio, and ventilatory support showed little or no correlation with mortality among patients with respiratory infections. Many of these variables were significant correlates of mortality in univariate analysis but lost significance in multivariate analysis. However, it is possible that the study is underpowered since only a total of 22 deaths were reported in the study.
Infant (< 1 Year) Mortality
Respiratory Infections
In the 13 studies evaluating respiratory tract infections, mortality rates ranged from 1.2 to 15.3% among admitted infants. Malnutrition, low oxygen saturation, younger age and positive Human Immunodeficiency Virus (HIV) status were top predictors of mortality in these patients. The odds of mortality among malnourished patients varied from 3.8 (95% CI: 2.7–5.4) to 6.32 (95% CI: 2.72–14.57). Among four studies, the odds of mortality among patients with lower oxygen saturation were 2.7 (95% CI: 2.1–3.5), 2.46 (95% CI: 1.3–4.65), and significant, but not provided, in the two remaining studies. The odds ratios of mortality among younger infants with respiratory infections, defined as < 4 months in one study and < 6 months in another, varied from 2.4 (95% CI: 1.6–3.5) to 3.6 (95% CI: 2.8–4.6). One study showed an association between high respiratory rate and mortality, while another showed high respiratory rates to be significantly associated with mortality. Cyanosis (four studies), wheezing (four studies), duration of breastfeeding (two studies) and congenital cardiac abnormalities (two studies) were not found to be correlates of mortality in these studies.
Diarrhea
In the four studies focused on infants admitted with diarrhea, the mortality rate was between 5 and 11.1%. Malnutrition and the absence of breastfeeding were the top predictors of mortality among both in-hospital and post-discharge populations, showing statistically significant correlations with mortality. The odds of mortality varied widely from 1.9 (95% CI: 1.6–2.3) to 84.16 (95% CI: 9.1–775.9) among malnourished patients, and from 2.35 (95% CI: 1.44–3.84) to 4.2 (95% CI: 1.3–13.2) among non-breastfed patients. Dehydration status, blood in stools, xerophthalmia, and concurrent pneumonia did not appear as statistically significant correlates of mortality.
Sepsis/Serious Infections
In the three studies focused on sepsis or serious infection, organ dysfunction, the need for more than 2 inotropes and bacterial isolates in blood showed significant correlations with mortality. The odds of mortality was 18 (95% CI 2.2–144) for organ dysfunction, 3.5 (95% CI 1.3–9.2) for those needing for more than 2 inotropes and significant, although not specifically provided, for those with bacteremia. Zinc intake and a Pediatric Risk of Mortality (PRISM) score >10 were not statistically significantly correlated in these studies.
Other studies
Two studies assessed predictors of mortality among patients with meningitis. Low hemoglobin (OR 2.9, 95% CI: 1.5–5.3), refusal or inability to feed (OR 3.3, 95% CI: 2.1–5.6), vomiting (OR 1.7, 95% CI: 1.2–2.7), and drowsiness (OR 2.9, 95% CI: 1.7–5) were significant predictors of mortality. In addition, high WBC count and low CSF glucose were significantly associated with increased odds of mortality, although odds ratios were not specifically stated. Multiple seizures, coma at presentation, neck stiffness, hyponatremia, hyperglycemia, hypoglycorrhachia, and turbid CSF showed no significant correlation with mortality. This is likely underpowered as only 22 deaths were reported in the study describing the above risk factors.
One study focused on mortality among a post-discharge population. This study found malnutrition defined as weight-for-age Z score < −3 (OR 3.42, 95% CI 2.5–4.68), hypoxia (OR 2.3, 95% CI: 1.64–3.23), bacteremia (OR 1.77, 95% CI: 1.15–2.74), jaundice (OR 1.77, 95% CI: 1.08–2.91), hepatomegaly (OR 2.34, 95% CI: 1.6–3.42), and hospitalization length < 13 days (OR 1.83, 95% CI: 1.33–2.52) showed significant correlations with post-discharge mortality. Age and parasitemia showed no correlation with mortality outcomes.
Lastly, in one study on infants with measles, low birth weight and nosocomial infections showed significant correlations with mortality, although the odds ratios were not provided. Infant age and vitamin A supplementation did not correlate with mortality.
Discussion
This systematic review focused on risk factors of mortality among hospitalized neonates and infants under 1 year of age due to infectious causes in LMICs. To the best of our knowledge, this is the first systematic literature review that focuses of clinical predictors of mortality from severe infection among hospitalized neonates and infants in developing countries. Most previous work on these populations consist of single population-based studies (11, 63). Previous systematic reviews of clinical predictors of mortality from severe infections have included infants in developed countries, which may not applicable to areas of the world where the majority of the disease burden occurs (10). Furthermore, other systematic reviews have examined predictors of severe illness and/hospitalization rather than mortality (64, 65), the latter which is a more objective, directly actionable outcome for use in intervention trials. Moreover, other previous work have focused on on all-cause mortality from sepsis as universally preventable disease, rather than more specific illness populations (7). This evidence base is complementary to publications from the WHO, CDC, and other international organizations, which approach neonatal and infant mortality from a population perspective. This systematic review consolidates mortality outcomes on the individual and community level, by focusing on clinical, laboratory and socio-demographic risk factors. It can be used to guide interventions to address the epidemic of early mortality among over 4 million infants and neonates in developing countries.
Comprehensive understanding of the clinical risk factors for mortality in these populations is important for several reasons. First, compilation of risk factors will help to drive the development risk prediction models aimed at the identification of high-risk infants, in order to triage resources to improve health outcomes and health care efficiency. This precision public-health approach has previously been utilized to derive risk-prediction models. For example, the miniPIERS, a prediction model to identify women at risk of hypertensive-related death, was developed to intervene among high-risk pregnant women in LMICs (66). Similar models have been created to identify high-risk patients with Chagas disease and to predict pediatric post-discharge mortality (67–69). Second, expanding our understanding of clinical risk factors for mortality in this age group could highlight key diagnostic approaches and research gaps in these areas. Lastly, specific populations or diseases may have limited research, and the benefits of systematic reviews in the identification of such gaps is well-described (12, 13).
The predictors of mortality were assessed for two distinct age groups: neonates (< 28 days old) and infants (28 days to 12 months old). Overall, the most frequent predictors of mortality in neonates were young age, fever or hypothermia, low birth weight and prematurity, while the most frequent predictors of mortality in infants were malnutrition, breast-feeding status and low oxygen saturation. It appears that perinatal variables play a larger role in predicting mortality during the neonatal period, whereas nutritional factors play a larger role among infants. Although both age groups encompassed a variety of disease populations, these risk factors found commonality in predicting mortality despite the heterogeneity in underlying conditions. Some of these predictors, such as temperature instability, young age, low birth weight, and prematurity, may not be surprising from a diagnostic perspective, as they are directly related to inherent causes of neonatal mortality. However, other predictors, such as a low oxygen saturation and breastfeeding, are more interesting from an interventional point of view. For instance, our results suggest that substantial efforts should be directed toward reducing malnutrition, promoting breastfeeding (parallel to HIV prevention) and developing affordable technologies for identifying oxygenation status among neonates and infants.
On the whole, included studies in this systematic review upheld strong research designs and maintained internal validity, based on the Newcastle-Ottawa scale. The primary limitation was comparability, as many studies did not adequately control for confounders, possibly due to small sample sizes. Retrospective studies utilizing medical record review were often faced with incomplete records, and the included studies may or may not have addressed this issue adequately. Other limitations of cohort studies often include recall and reporting bias, which were not assessed by this scale.
It is relevant to note that many of the studies identified for full text review assessed risk factors for serious illness, rather than mortality, and these studies were ultimately excluded (11, 70, 71). This systematic review focused primarily on predictors of mortality, since this downstream outcome is critical to the development of prediction tools or interventions to improve child health and survival. Furthermore, the definition of mortality is more consistent as compared to serious illness, which can have broad and heterogeneous definitions.
Although the definition of mortality is more objective, a major source of heterogeneity between studies was the variable definitions of risk factors. For example, malnutrition definitions varied from weight-for-age Z score < 3 standard deviations to weight-for-age Z score < 60% to first degree malnutrition on the Gomez scale (corresponding to < 90% expected weight-for-age). Likewise, definitions for low oxygen saturation varied substantially between studies. Low oxygen saturation ranged from SpO2 < 70 to < 92%. This heterogeneity was pervasive among sub-populations and limited the ability to perform meta-analyses. A further source of heterogeneity is the differences in inclusion criteria for populations with the same illness. For example, one study on if late-onset sepsis (defined as 3–30 days of life) is a risk factor for mortality looked at pre-term neonates whereas another study looked at at-term ones. This difference may be partially responsible for one studying showing a statistically significant positive correlation with mortality whereas the other showed a statistically significant negative correlation.
Although uncommon, a small proportion of included studies did not provide definition for the evaluated risk factors, such as fever and young age. The provision of clear definitions for risk factors is crucial for generalizability and study replication. Moreover, increased standardization of these definitions would allow future data to be more amenable to meta-analyses. This would greatly enhance the translation potential of these studies, especially since many of the existing individual studies are underpowered for statistical analysis.
This systematic review has several limitations. First, some studies identified in this review only conducted univariate analyses while others conducted multivariate analyses. Thus, risk factors identified as statistically significant in the univariate analyses may cease to be statistically significant if multivariate analyses were performed. Second, most studies focus on single disease populations, resulting in risk factors that may not be generalizable across multiple illness populations. Since sepsis is associated with most disease-related deaths (72), it may provide an overarching framework within which to assess mortality predictors that are applicable across different acute illness processes. Third, few studies focused on post-discharge mortality, resulting in a critical knowledge gap in child mortality research. Post-discharge mortality rates have been shown to be equal or greater than in-hospital mortality rates in pediatric populations (67). More post-discharge studies on neonates and infants would be useful in determining if there are additional risk factors relevant to this population. Fourth, many risk factors which we evaluated did not demonstrate statistical significance. Frequently, small sample sizes may have limited the ability to evaluate the association of important variables on mortality. These results underscore the need for adequately powered studies, but also clearly demonstrate the importance of those variables which did achieve statistical significance. Furthermore, some clinically important risk factors, such as maternal HIV status, maternal malnutrition and implementation of TB or HIV preventative therapy during pregnancy, may have not been captured as statistically significant risk factors as a result of many included studies being underpowered as well as the focus on hospitalized patients as an inclusion criteria. Lastly, many parameters found to be important predictors of mortality among infants, such as hemoglobin level, oxygen saturation and nutritional status, were not assessed in studies focused on serious infections among neonatal patients. The inclusion of these parameters in future studies has the potential to elucidate strong predictors of infant mortality.
Conclusions
This systematic review summarizes risk factors for mortality among neonates and infants in LMICs. Our data highlight major risk factors that could be incorporated into risk-prediction models to identify children at risk for in-hospital or post-discharge mortality. This data also points toward specific interventions that could be further incorporated into healthcare systems or policies. Targeted, evidence-based interventions have the potential to vastly reduce the burden of preventable mortality among neonates and infants around the world. Future studies in this area should incorporate precise definitions and risk estimates for mortality, including larger sample sizes, detailed statistical analysis, and overlapping risk factors between these high-risk age groups.
Author Contributions
LL prepared first draft of manuscript, conducted systematic search and data extraction, assisted in analysis of data, approved final version of manuscript. NaK and LE conducted systematic search and data extraction, assisted in analysis of data, approved final version of manuscript. NiK, PL, JA, and JK reviewed and edited manuscript and provided critical interpretation of data, assisted in analysis of data, approved final version of manuscript. MW conceived study idea, assisted in systematic search and data extraction, assisted in analysis of data, reviewed and edited manuscript and provided critical interpretation of data, approved final version of manuscript.
Funding
This work was supported by Grand Challenges Canada.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2018.00277/full#supplementary-material
References
1. You D, Hug L, Ejdemyr S. Global regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Inter-agency Group for child mortality estimation. Lancet (2015) 386:2275–86. doi: 10.1016/S0140-6736(15)00120-8
2. Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L, et al. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970–2010: a systematic analysis of progress towards millennium development goal 4. Lancet (2010) 375:1988–2008. doi: 10.1016/S0140-6736(10)60703-9
3. Ehret DY, Patterson JK, Bose CL. Improving neonatal care: a global perspective. Clin Perinatol. (2017) 44:567–82. doi: 10.1016/j.clp.2017.05.002
4. Zupan J. Perinatal mortality in developing countries. N Engl J Med. (2005) 352:2047–8. doi: 10.1056/NEJMp058032
5. Children: Reducing Mortality. World Health Organization (2016). Available online at: http://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (Accessed September 22, 2018).
6. Lawn JE, Cousens S, Zupan J. 4 million neonatal deaths: when? Where? Why? Lancet (2005) 365:891–900. doi: 10.1016/S0140-6736(05)71048-5
7. World Health Organization. Global Health Observatory (GHO) Data: Causes of Child Mortality (2016). Available online at: http://www.who.int/gho/child_health/mortality/causes/en/ (Accessed September 22, 2018).
8. Mahy M. DHS Comparative Reports: Childhood Mortality in the Developing World. Calverton, MD: ORC Macro (2003). Available Online at: https://dhsprogram.com/pubs/pdf/CR4/CR4.pdf
9. Rutstein SO. Factors associated with trends in infant and child mortality in developing countries during the 1990s. Bull World Health Organ. (2000) 78:1256–70.
10. Van den Bruel A. Diagnostic value of clinical features at presentation to identify serious infection in children in developed countries: a systematic review. Lancet (2010) 375:834–45. doi: 10.1016/S0140-6736(09)62000-6
11. Young Infants Clinical Signs Study Group. Clinical signs that predict severe illness in children under age 2 months: a multicentre study. Lancet (2008) 371:135–42. doi: 10.1016/S0140-6736(08)60106-3
12. Saha S, Chant D, and McGrath J. A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatr. (2007) 64:1123–31. doi: 10.1001/archpsyc.64.10.1123
13. Jayne Wilson JG, Moroz V, Gaze M, Wheatley K. Using systematic reviews to identify research gaps–a case study: mIBG for the treatment of neuroblastoma in children. Trials (2013) 14(Suppl. 1):126. doi: 10.1186/1745-6215-14-S1-P126
14. Kissoon N, Reinhart K, Daniels R, Machado MFR, Schachter RD, Finfer S. Sepsis in children: global implications of the world health assembly resolution on sepsis. Pediatr Crit Care Med. (2017) 18:e625–7. doi: 10.1097/PCC.0000000000001340
15. Jahan S. Human Development Report 2016: Human Development for Everyone. New York, NY: UNDP (2016).
16. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses (2018). Available online at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
17. Ballot DE, Bosman N, Nana T, Ramdin T, Cooper PA. Background changing patterns of neonatal fungal sepsis in a developing country. J Trop Pediatr. (2013) 59:460–4. doi: 10.1093/tropej/fmt053
18. Basu S, Paul DK, Ganguly S, Chandra PK. Risk factors for mortality from neonatal tetanus: 7 years experience in North Bengal, India. Ann Trop Paediatr. (2006) 26:233–239. doi: 10.1179/146532806X120336
19. Bhatnagar S, Wadhwa N, Aneja S, Lodha R, Kabra SK, Natchu UC, et al. Zinc as adjunct treatment in infants aged between 7 and 120 days with probable serious bacterial infection: a randomised, double-blind, placebo-controlled trial. Lancet (2012) 379:2072–8. doi: 10.1016/S0140-6736(12)60477-2
20. Chiabi A, Djoupomb M, Mah E, Nguefack S, Mbuagbaw L, Zafack J, et al. The clinical and bacteriogical spectrum of neonatal sepsis in a tertiary hospital in Yaounde, Cameroon. Iran J Pediatr. (2011) 21:441–8.
21. Coakley KJ, Coakley CA, Spooner V, Smith TA, Javati A, Kajoi M. A review of measles admissions and deaths in the paediatric ward of Goroka Base Hospital during 1989. PNG Med J. (1991) 34:6–12.
22. Daoud AS, Al-Sheyyab M, Abu-Ekteish F, Obeidat A, Ali AA,El-Shanti H. Neonatal meningitis in northern Jordan. J Trop Pediatr. (1996) 42:267–70.
23. Davies-Adetugbo AA, Torimiro SE, Ako-Nai KA. Prognostic factors in neonatal tetanus. Trop Med Int Health (1998) 3:9–13. doi: 10.1046/j.1365-3156.1998.00162.x
24. Demers AM, Morency P, Mberyo-Yaah F, Jaffar S, Blais C, Somsé P et al. Risk factors for mortality among children hospitalized because of acute respiratory infections in Bangui, Central African Republic. Pediatr Infect Dis J. (2000) 19:424–32.
25. Dikici B, Uzun H, Yilmaz-Keskin E, Tas T, Gunes A, Kocamaz H, et al. Neonatal tetanus in Turkey; what has changed in the last decade? BMC Infect Dis. (2008) 8:112. doi: 10.1186/1471-2334-8-112
26. Djelantik IG, Gessner BD, Sutanto A, Steinhoff M, Linehan M, Moulton LH, et al. Case fatality proportions and predictive factors for mortality among children hospitalized with severe pneumonia in a rural developing country setting. J Trop Pediatr. (2003) 49:327–32. doi: 10.1093/tropej/49.6.327
27. Duke T, Mgone J, Frank D. Hypoxaemia in children with severe pneumonia in Papua New Guinea. Int J Tuberculosis Lung Dis. (2001) 5:511–9.
28. Ertem M, Cakmak A, Saka G, Ceylan A. Neonatal tetanus in the South-Eastern region of Turkey: changes in prognostic aspects by better health care. J Trop Pediatr. (2004) 50:297–300. doi: 10.1093/tropej/50.5.297
29. Ghiorghis B. Neonatal sepsis in Addis Ababa Ethiopia: a review of 151 bacteremic neonates. Ethiop Med J. (1997) 35:169–76.
30. Goel A, Bamford L, Hanslo D, Hussey G. Primary staphylococcal pneumonia in young children: a review of 100 cases. J Trop Pediatr. (1999) 45:233–6.
31. Gürkan F, Boşnak M, Dikici B, Boşnak V, Taş MA, Haspolat K, et al. Neonatal tetanus: a continuing challenge in the southeast of Turkey: risk factors, clinical features and prognostic factors. Eur J Epidemiol. (1999) 15:171–4.
32. Gürses N, Aydin M. Factors affecting prognosis of neonatal tetanus. Scand J Infect Dis. (1993) 25:353–5.
33. Ibinda F, Bauni E, Kariuki SM, Fegan G, Lewa J, Mwikamba M, et al. Incidence and risk factors for neonatal tetanus in admissions to Kilifi County Hospital, Kenya. PLoS ONE (2015) 10:e0122606. doi: 10.1371/journal.pone.0122606
34. Khan MR, Maheshwari PK, Masood K, Qamar FN, Haque AU. Epidemiology and outcome of sepsis in a tertiary care PICU of Pakistan. Indian J Pediatr. (2012) 79:1454–8. doi: 10.1007/s12098-012-0706-z
35. Kuti BP, Bello EO, Jegede TO, Olubosede O. Epidemiological, clinical and prognostic profile of childhood acute bacterial meningitis in a resource poor setting. J Neurosci Rural Pract. (2015) 6:549–57. doi: 10.4103/0976-3147.165424
36. Lehmann D, Yeka W, Rongap T, Javati A, Saleu G, Clegg A, et al. Aetiology and clinical signs of bacterial meningitis in children admitted to Goroka Base Hospital, Papua New Guinea, 1989–1992. Ann Trop Paediatr. (1999) 19:21–32.
37. Mathur NB, Garg K, Kumar S. Respiratory distress in neonates with special reference to pneumonia. Indian Pediatr. (2002) 39:529–37.
38. Islam MA, Rahman MM, Mahalanabis D, Rahman AK. Death in a diarrhoeal cohort of infants and young children soon after discharge from hospital-risk factors and causes by verbal autopsy. J Trop Pediatr. (1996) 42:342–7.
39. Moïsi JC, Gatakaa H, Berkley JA, Maitland K, Mturi N, Newton CR. Excess child mortality after discharge from hospital in Kilifi, Kenya: a retrospective cohort analysis. Bull World Health Organ. (2011) 89:725–32, 732A. doi: 10.2471/BLT.11.089235
40. Mugalu J, Nakakeeto M, Kiguli S, Mulindwa DH. Aetiology, risk factors and immediate outcome of bacteriologically confirmed neonatal septicaemia in Mulago hospital, Uganda. Afr Health Sci. (2006) 6:120–6.
41. Mulholland EK, Ogunlesi OO, Adegbola RA, Weber M, Sam BE, Palmer A, et al. Etiology of serious infections in young Gambian infants. Pediatr Infect Dis J. (1999) 18(10 Suppl.):S35–41.
42. Nantanda R, Hildenwall H, Peterson S, Kaddu-Mulindwa D, Kalyesubula I, Tumwine JK. Bacterial aetiology and outcome in children with severe pneumonia in Uganda. Ann Trop Paediatr. (2008) 28:253–60. doi: 10.1179/146532808X375404
43. Nathoo KJ, Nkrumah FK, Ndlovu D, Nhembe M, Pirie DJ, Kowo H. Acute lower respiratory tract infection in hospitalized children in Zimbabwe. Ann Trop Paediatr. (1993) 13:253–61.
44. Okomo UA, Dibbasey T, Kassama K, Lawn JE, Zaman SM, Kampmann B, et al. Neonatal admissions, quality of care and outcome: 4 years of inpatient audit data from the Gambia's teaching hospital. Paediatr Int Child Health (2015) 35:252–64. doi: 10.1179/2046905515Y.0000000036
45. Okoromah CN, Lesi FE, Egri-Okwaji MT, Iroha E. Clinical and management factors related to outcome in neonatal tetanus. Niger Postgrad Med J. (2003) 10:92–5.
46. Ozkan H, Cetinkaya M, Koksal N, Celebi S, Hacimustafaoglu M. Culture-proven neonatal sepsis in preterm infants in a neonatal intensive care unit over a 7 year period: Coagulase-negative Staphylococcus as the predominant pathogen. Pediatr Int. (2014) 56:60–6. doi: 10.1111/ped.12218
47. Ramakrishna B, Graham SM, Phiri A, Mankhambo L, Duke T. Lactate as a predictor of mortality in Malawian children with WHO-defined pneumonia. Arch Dis Child. (2012) 97:336–42. doi: 10.1136/archdischild-2011-300920
48. Rodríguez DA, Rodríguez-Martínez CE, Cárdenas AC, Quilaguy IE, Mayorga LY, Falla LM, et al. Predictors of severity and mortality in children hospitalized with respiratory syncytial virus infection in a tropical region. Pediatr Pulmonol. (2014) 49:269–76. doi: 10.1002/ppul.22781
49. Sachdev HP, Kumar S, Singh KK, Satyanarayana L, Puri RK. Risk factors for fatal diarrhea in hospitalized children in India. J Pediatr Gastroenterol Nutr. (1991) 12:76–81.
50. Saleem AF, Qamar FN, Shahzad H, Qadir M, Zaidi AK. Trends in antibiotic susceptibility and incidence of late-onset Klebsiella pneumoniae neonatal sepsis over a six-year period in a neonatal intensive care unit in Karachi, Pakistan. Int J Infect Dis. (2013) 17:961–5. doi: 10.1016/j.ijid.2013.04.007
51. Santhanakrishnan BR, Ramalingam R. Risk factors for mortality in children with diarrhoeal disease in Madras, India. J Diarrhoeal Dis Res. (1987) 5:36–9.
52. Sarna MS, Saili A, Dutta AK, Kumari S. Neonatal mortality patterns in an urban hospital. Indian Pediatr. (1991) 28:719–24.
53. Sehgal, V, Sethi GR, Sachdev HP, Satyanarayana L. Predictors of mortality in subjects hospitalized with acute lower respiratory tract infections. Indian Pediatr. (1997) 34:213–9.
54. Shann F, MacGregor D, Richens J, Coakley J. Cardiac failure in children with pneumonia in Papua New Guinea. Pediatr Infect Dis J. (1998) 17:1141–3.
55. Sheikh AN, Sajjad A, Hanif S. Neonatal sepsis: an evaluation of bacteriological spectrum, antibiotic susceptibilities and prognostic predictors at Civil Hospital, Karachi. Pak Paediatr J. (2014) 38:143–55.
56. Simiyu DE. Morbidity and mortality of neonates admitted in general paediatric wards at Kenyatta National Hospital. East Afr Med J. (2003) 80:611–6.
57. Smyth A, Carty H, Hart CA. Clinical predictors of hypoxaemia in children with pneumonia. Ann Trop Paediatr. (1998) 18:31–40. doi: 10.1080/02724936.1998.11747923
58. Teka T, Faruque AS, Fuchs GJ. Risk factors for deaths in under-age-five children attending a diarrhoea treatment centre. Acta Paediatr. (1996) 85:1070–5. doi: 10.1111/j.1651-2227.1996.tb14219.x
59. Tupasi TE, Velmonte MA, Sanvictores ME, Abraham L, De Leon LE, Tan SA, et al. Determinants of morbidity and mortality due to acute respiratory infections: Implications for intervention. J Infect Dis. (1988) 157:615–23.
60. Yaramis A, Tas MA. Neonatal tetanus in the southeast of Turkey: risk factors, and clinical and prognostic aspects. review of 73 cases, 1990–1999. Turk J Pediatr. (2000) 42:272–4.
61. Zhang Q, Guo Z, Bai Z, MacDonald NE. A 4 year prospective study to determine risk factors for severe community acquired pneumonia in children in southern China. Pediatr Pulmonol. (2013) 48:390–7. doi: 10.1002/ppul.22608
62. Islam MA, Rahman MM, Mahalanabis D, Rahman AK. Death in a diarrhoeal cohort of infants and young children soon after discharge from hospital: risk factors and causes by verbal autopsy. J Trop Pediatr. (1996) 42:342–7.
63. Weber MW, Carlin JB, Gatchalian S, Lehmann D, Muhe L, Mulholland EK, et al. Predictors of neonatal sepsis in developing countries. Pediatr Infect Dis J. (2003) 22:711–7. doi: 10.1097/01.inf.0000078163.80807.88
64. Coghill JE, Simkiss DE. Which clinical signs predict severe illness in children less than 2 months of age in resource poor countries? J Trop Pediatr. (2011) 57:3–8. doi: 10.1093/tropej/fmr001
65. Opiyo N, English M. What clinical signs best identify severe illness in young infants aged 0–59 days in developing countries? a systematic review. Arch Dis Child. (2011) 96:1052–9. doi: 10.1136/adc.2010.186049
66. Payne BA, Hutcheon JA, Ansermino JM, Hall DR, Bhutta ZA, Bhutta SZ, et al. A risk prediction model for the assessment and triage ofwomen with hypertensive disorders of pregnancy in low-resourced settings: the miniPIERS (Pre-eclampsia Integrated Estimate of RiSk) multi-country prospective cohort study. PLoS Med. (2014) 11:e1001589. doi: 10.1371/journal.pmed.1001589
67. Rassi A Jr, Rassi A, Little WC, Xavier SS, Rassi SG, Rassi AG, et al. Development and validation of a risk score for predicting death in Chagas' heart disease. N Engl J Med. (2006) 355:799–808. doi: 10.1056/NEJMoa053241
68. Wiens MO, Kumbakumba E, Larson CP, Ansermino JM, Singer J, Kissoon N, et al. Postdischarge mortality in children with acute infectious diseases: derivation of postdischarge mortality prediction models. BMJ Open (2015) 5:e009449. doi: 10.1136/bmjopen-2015-009449
69. Wiens MO, Kissoon N, Kabakyenga J. Smart hospital discharges to address a neglected epidemic in sepsis in low- and middle-income countries. JAMA Pediatr. (2018) 172:213–4. doi: 10.1001/jamapediatrics.2017.4519
70. Shitaye D, Asrat D, Woldeamanuel Y, Worku B. Risk factors and etiology of neonatal sepsis in Tikur Anbessa University Hospital, Ethiopia. Ethiop Med J. (2010) 48:11–21.
71. Pengsaa K, Lumbiganon P, Taksaphan S, Pairojkul S, Sookpranee T, Kosuwon P, et al. Risk factors for neonatal Klebsiella septicemia in Srinagarind Hospital. Southeast Asian J Trop Med Public Health (1996) 27:102–6.
Keywords: risk prediction, neonatal mortality, infant mortality, systematic review, developing countries, infectious disease, sepsis, hospital mortality
Citation: Liang L, Kotadia N, English L, Kissoon N, Ansermino JM, Kabakyenga J, Lavoie PM and Wiens MO (2018) Predictors of Mortality in Neonates and Infants Hospitalized With Sepsis or Serious Infections in Developing Countries: A Systematic Review. Front. Pediatr. 6:277. doi: 10.3389/fped.2018.00277
Received: 31 March 2018; Accepted: 12 September 2018;
Published: 04 October 2018.
Edited by:
Valeriane Leroy, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Lucy Thairu, Stanford University, United StatesGiuseppe Liotta, Università degli Studi di Roma Tor Vergata, Italy
Copyright © 2018 Liang, Kotadia, English, Kissoon, Ansermino, Kabakyenga, Lavoie and Wiens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthew O. Wiens, matthew.wiens@cw.bc.ca