Article Text

Abstract
Objectives: To describe presentation and outcome of patients with scleroderma renal crisis (SRC).
Methods: SRC was defined as rapidly progressive oliguric renal insufficiency and/or rapidly progressive arterial hypertension occurring during the course of systemic sclerosis (SSc). Chronic dialysis-free survival was analysed using multivariate Cox proportional hazards regression models. The risk for developing SRC associated with corticosteroid (CS) exposure during the preceding 1- or 3-month periods was analysed according to a case–crossover design.
Results: A total of 50 SSc patients aged 53.3 (14.5) (mean (SD)) years were included in the study. SRC occurred between 1979 and 2003, after a mean (SD) disease duration of 27.7 (49.1) months. A total of 43 (86%) patients had diffuse SSc, 5 (10%) had limited cutaneous SSc and 2 (4%) had SSc sine scleroderma. At the time of SRC, 10 (20%) patients were taking angiotensin converting enzyme inhibitors, and mean creatininaemia was 468 (293) μmol/l. A total of 28 (56%) patients required haemodialysis. In all, 11 patients underwent a renal biopsy, all of them had specific vascular lesions of SRC. Multivariate analyses retained age >53 years and normal blood pressure as independent predictors of decreased dialysis-free survival. Exposure to CS prior to SRC was identified in 30 (60%) patients. The odds ratios for developing SRC associated with CS exposure during the preceding 1- or 3-month periods were 24.1 (95% CI 3.0–193.8) and 17.4 (95% CI 2.1–144.0), respectively.
Conclusion: SRC remains associated with severe morbidity and mortality. CS might increase the risk of developing SRC. Further studies are needed to confirm these results.
Statistics from Altmetric.com
Vascular manifestations of systemic sclerosis (SSc) represent a hallmark of the disease and comprise Raynaud phenomenon, digital ischemia, pulmonary arterial hypertension (PAH)1 and scleroderma renal crisis (SRC).2 3 SRC is mainly encountered in patients with diffuse SSc (dSSc) during the first 4 years of disease evolution.4 5
Prior to the late 1970s, SRC was observed in 12–18% SSc patients and renal complications were a major cause of death.6 The routine use of angiotensin-converting enzyme inhibitors (ACEI) dramatically improved outcomes, with a fall in the 12-month mortality rate from 76% to less than 15% in the United States.4 Thus, causes of death in patients with SSc were recently reported to be mainly involving the lungs and less frequently SRC.7
Although ACEI improved the outcome of SSc patients experiencing SRC, the prognosis of this major event remains reserved.3 8 9 In order to analyse the prognosis of SRC and address the potential triggering role of corticosteroids (CS) in this condition, we decided to conduct a multicentre retrospective study in France.
PATIENTS AND METHODS
Patient selection
To be eligible for the study, SSc patients had to fulfil the American College of Rheumatology criteria10 and/or the Leroy criteria11 for SSc. Patients with SSc sine scleroderma had no detectable skin involvement;12 limited cutaneous SSc (lcSSc) was defined by skin thickening in areas distal to the elbows and knees and dSSc was defined by the presence of skin thickening proximal, as well as distal, to the elbows and knees.13 Only patients who experienced SRC as defined by rapidly progressive oliguric renal insufficiency with no other explanation and/or rapidly progressive hypertension occurring during the course of SSc were included in the study.4 Normotensive SRC was defined by an increase in serum >50% over baseline or serum creatinine ⩾20% of upper limit of normal and one of the following five features; proteinuria ⩾2+ by dipstick, haematuria ⩾2+ dipstick or ⩾10 red blood cells/high-power field (hpf), thrombocytopenia<100 000/mm3, haemolysis defined as anaemia not due to others causes and either schistocytes or other red blood cell fragments seen on blood smear, or increased reticulocyte count, or renal biopsy findings consistent with SRC.14
Study design
French physicians involved in the care of SSc patients were contacted by mail through the “Groupe Français de Recherche sur la Sclérodermie” (GFRS) and French Vasculitis Study Group mailing lists. They were asked, based on their recall, to declare retrospectively patients followed in their centre who had experienced SRC. A total of 285 physicians from 63 centres were contacted in October 2003, and reported 54 cases of SRC. Medical charts from the 54 patients reported were reviewed by the same observer (LT). Four of them were excluded for incomplete data collected at the time of SRC.
Parameters recorded were age; sex; ethnicity; year of onset of Raynaud syndrome; age at diagnosis; year of onset of the first non-Raynaud manifestation; disease duration; disease form (SSc sine scleroderma, lcSSc or dSSc); dyspnoea (assessed by the New York Heart Association 4-point scale); pitting scars; oedema; digital ulcers; calcinosis; joint and/or muscle involvement; oesophagus involvement defined by dysphagia, heartburn, and regurgitation; bowel involvement defined by malabsorption; pseudo-obstruction and/or bacterial overgrowth; heart involvement corresponding to conduction block or arrhythmia and/or cardiac insufficiency defined on a clinical and/or echocardiography basis with evidence of left ventricular systolic or diastolic dysfunction; interstitial lung disease (ILD) defined upon high-resolution computed tomography of the chest including one or more of the following features: isolated ground glass opacities; honeycombing, and concurrent presence of ground glass attenuation and traction bronchiectasis and/or bronchiolectasis and evaluated with pulmonary function tests (PFT) including forced vital capacity (FVC), total lung capacity (TLC) and TLCO; restrictive syndrome defined by a TLC or a FVC <80% of predicted values; PAH detected by echocardiography, with a tricuspid gradient of 30 mmHg (ie, an estimated systolic PAP ⩾30+10 = 40 mmHg assuming a right atrial pressure of 10 mmHg in all patients); and myopathy as assessed by proximal muscle weakness and elevated creatine kinases (CK). Detailed medical history prior to SRC and at onset and management of SRC were also collected: blood pressure, laboratory values of maximal serum creatinine, creatinine clearance as calculated using the Cokroft formula, white blood cell count, platelet count, haemoglobin level, presence of schistocytosis (>1%), evidence for haemolysis as assessed by haptoglobin and lactico-deshydrogenase plasma levels, haematuria, proteinuria, granular cast, CK, anti-nuclear, anti-topoisomerase 1 and anti-centromere antibodies. Thrombotic microangiopathy was defined by the association of thrombocytopenia <100 000/mm3, haemolysis defined as anaemia not due to others causes and either schistocytes or other red blood cell fragments seen on blood smear, or increased reticulocyte count. Patients were divided into four categories regarding outcome: absence of dialysis, temporary dialysis, permanent dialysis and death. Causes of death were classified as related or unrelated to SSc.
Statistical analysis
Patient’s survival was assessed by life-table analysis using the Kaplan–Meier method.15 Survival time was calculated from the date SRC had been diagnosed and ended at the date of censoring or at the time of reaching the investigated endpoint. We evaluated the occurrence of death or chronic dialysis (“chronic dialysis-free survival”) as a function of the 10 demographic, clinical and laboratory variables assessed at diagnosis of SRC, and Cox proportional hazards models16 were fitted to examine the individual and combined effects of these variables. The effect of continuous variables was analysed both as continuous covariates and as indicator covariates after stratification according to quartiles or the median values of their distribution. These variables were then used as a function of their linear or non-linear association with survival and, when used as categorical covariates, according to the threshold that defined the group at highest risk. The multivariate model included all the parameters that had a p value of ⩽0.20 in univariate analysis and used a backward selection procedure. To exclude events (deaths or chronic dialysis) potentially unrelated to SRC because they occurred a long time after SRC diagnosis from the survival analyses, we undertook two sensitivity analyses that censored the follow-up at a maximum of 12 and 6 months, respectively.
The effect of exposure to CS on the occurrence of SRC was examined by a case–crossover analysis that is a variant of a traditional case–control study. This analytic design, where participants act as his or her own control, is particularly suitable to study the effect of transient exposures on acute events.17 The principle of case–crossover analysis is based on comparisons of the probability of exposure to an investigated risk factor during the period immediately preceding the event (index period; eg, diagnosis of SRC), with that during one or several prior control periods. A major advantage of this method is that it eliminates the requirement for an additional control group, and thereby the risk of inter-person confounding inherent to traditional case–control studies.
For the current study, we compared each subject’s exposure to CS during the 3-month index period just before onset of SRC to that of consecutive 3-month control periods immediately preceding the index period; to explore the robustness of the results we conducted a separate analysis using 1-month effect periods. Each index period was matched to four control periods; however, for individuals for whom the diagnosis of SSc had been established for less than 12 months (for the analysis of 3-month effect periods) or 4 months (for 1-month effect periods) before onset of SRC, the index period was matched only to the control periods covering the time after the diagnosis of SSc. Matched odds ratios were computed using conditional logistic regression.
For all statistical analyses, p values of less than 0.05 were considered to be significant. All confidence intervals were calculated at the 95% level. Statistical analysis was computed using the SAS Statistical Package, version 9.1 (SAS Institute Inc., Cary, North Carolina, USA).
RESULTS
Clinical and biological characteristics at baseline
A total of 50 patients (mean (SD) age at the time of SRC: 53.3 (14.5) years; F/M ratio: 2.5) were included. Nine of them were recruited among the 180 SSc patients followed in our centre at the end of 2003, leading to an estimation of 5% prevalence of SCR in our cohort. Among the 50 patients, 43 (86%) had dSSc (table 1).
Seven (14%) patients developed SRC more than 4 years after the first non-Raynaud symptom. A total of 10 (20%) patients were on with low dose ACEI at the time of SRC. Exposure to CS was identified in 36 (72%) cases. CS were administered prior to the onset of SRC in 30 (60%) patients: orally in 28 (mean (SD) maximal prednisone dose: 48 (25) mg/d) and/or intravenously in 7 (mean (SD) maximal methylprednisolone dose: 606 (335) mg/d). Mean (SD) CS exposure before SRC was 8.7 (13.4) months (median 2.65 months), and exposure to CS was <3 months in 16 cases.
A total of 27 (54%) patients had ILD and restrictive syndrome. Neither of the 2 (4%) patients who had PAH underwent right heart catheterisation. Anti-nuclear antibodies were detected in 45 (90%) patients. The pattern of fluorescence was described in 42 of them, being nucleolar in 17 (34%). A total of 14 (32%) patients had anti-topoisomerase 1 antibodies and none had anti-centromere antibodies (table 1).
SRC-related clinical symptoms and laboratory findings are depicted in table 2. At the time of SRC, 44 (88%) had hypertension (blood pressure >140 mmHg systolic and/or 90 mmHg diastolic), with mean (SD) systolic and diastolic levels of 189 (39.9) and 111.4 (23.6), respectively. A total of 21 (42%) patients were oligoanuric. The mean (SD) serum creatinine level was 468 (293) μmol/l, and mean creatinine clearance was calculated at 18.3 (15.3) ml/min for 43 patients (data missing for 7 patients) on the day of initiation of SRC treatment. In all, 44 (88%) and 16 (32%) patients had a serum creatinine >150 μmol/and >500 μmol/l, respectively; 36 (84%) had a creatinine clearance <30 ml/min. A total of 42 out of 45 (93%) patients had anaemia, with a haemoglobin level <10 g/dl in 69% of them. A total of 23 (46%) patients had thrombotic microangiopathy, 13/31 (42%) had a haematuria as detected by dipstick or microscope, and 20/38 (53%) had proteinuria >0.5 g/24 h (not performed in anuric patients).
Renal histology
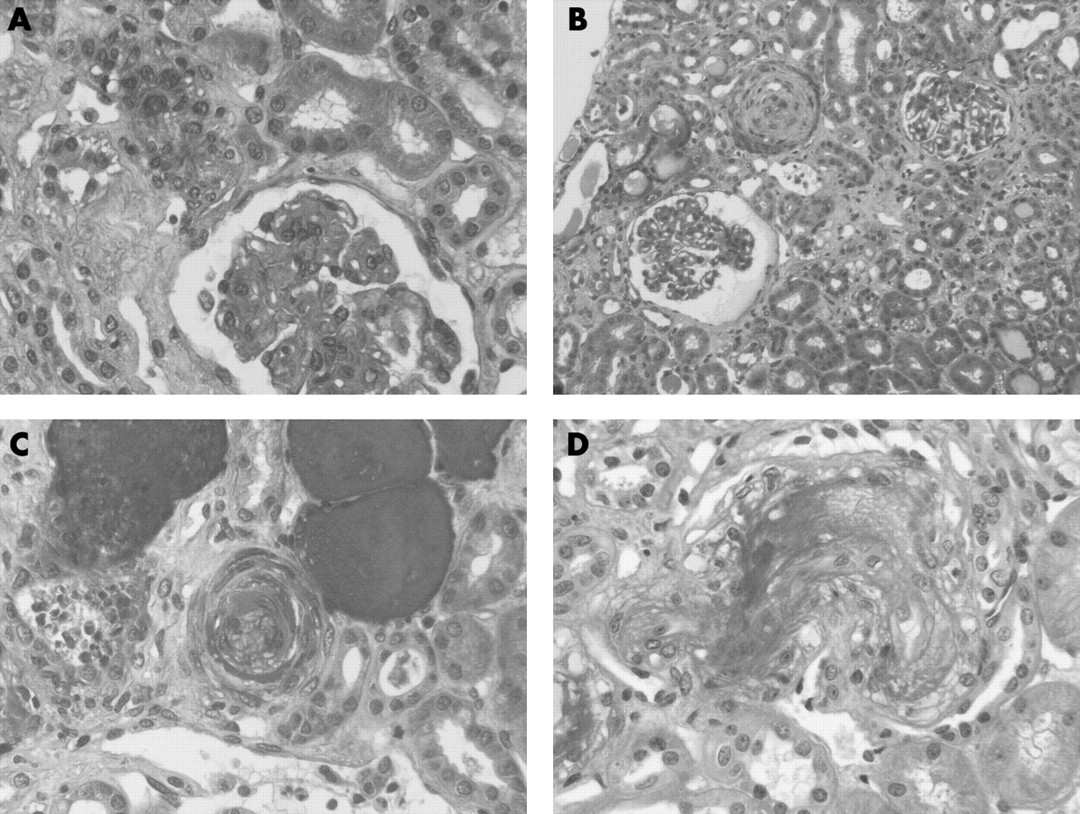
In total, 11 patients underwent a renal biopsy at the time of SRC, percutaneously in 5 and by venous catheterism in 6. All of the biopsies showed specific vascular lesions of SRC. Glomerular lesions were observed in all biopsies with glomerular microangiopathy in 6 and ischemic glomeruli in 9 (fig 1). Small arteries were involved in all cases with intraluminal thrombosis (n = 3), fibrinoid necrosis in the arterial walls (n = 4), mucoid intimal thickening and proliferation of intimal cells (“onionskin” lesions) (n = 9). Large vessels involvement with intimal proliferation or fibrous endarteritis was observed in 5 patients.
Renal outcome
After a mean (SD) follow-up of 47.0 (59.7) months, 28 (56%) patients required temporary or chronic haemodialysis, including 15 in whom haemodialysis started within the first 2 weeks after SRC (table 3).
Dialysis was stopped in 8 patients with a mean (SD) duration of 9.0 (9.8) months (median: 5.0). A total of 11 patients underwent prolonged haemodialysis and 9 died during the dialysis period. No patient underwent renal transplantation. A total of 20 (40%) patients required chronic dialysis, 17 (34%) died and 28 (56%) required chronic dialysis or died. Causes of death are listed in table 4.
In all, 47 (94%) patients received ACEI, including the 10 who were on with ACEI prior to the occurrence of SRC (median (SD) 9.5 (3.6) months), in whom the dose was increased. Eight of these 10 patients received CS at the time of SRC, 4 had normortensive SRC, 5 had thrombotic microangiopathy, 6 required chronic dialysis, and 3 died. In the remaining 37 patients who received ACEI, 2 presented normotensive SRC and 14 died. Overall, ACEI were prescribed alone in 4 patients, in association with calcium channel blockers in 23 patients, beta blockers in 5, and alpha and beta blockers in 2. In 5 additional patients, urapidil was added to ACEI and calcium channel blockers. Plasma exchanges were performed in 5 patients. One patient received Iloprost and is still on chronic dialysis.
Survival and case–crossover analyses
The respective 1- and 5-year survival rates were 78% (95% CI 66–90) and 69% (95% CI 55–83), and the 1- and 5-year chronic dialysis-free survival rates were 50% (95% CI 35–65) and 41% (95% CI 26–57) (fig 2). According to univariate survival analysis, occurrence of death or chronic dialysis was significantly higher for patients with age at SRC diagnosis >53 years, normal blood pressure (⩽140/90 mmHg), and requirement of dialysis at SRC diagnosis; none of the other variables could be significantly associated with chronic dialysis-free survival (table 5 and fig 3).


{kind=link}
{kind=link}
{kind=link}
Multivariate analyses retained age >53 years (hazard ratio (HR) = 2.5, p = 0.04) and normal blood pressure (HR = 6.7, p = 0.001) as independent predictors of decreased chronic dialysis-free survival (table 5). Essentially the same results were obtained for the uni- and multivariate models by the sensitivity analyses that censored the follow-up at maximums of 12 or 6 months.
Based on the 24 individuals for whom the time window of administration of CS could be determined, exposure rates in “index” and “control” windows were 83% (20/24) and 26% (14/54) for 3-months periods, and 79% (19/24) and 47% (38/81) for 1-month periods. Accordingly, the odds ratios of developing SRC associated with CS intake was 24.1 (95% CI 3.0–193.8) for the 3-month risk periods and 17.4 (95% CI 2.1–144.0) for the 1-month risk periods.
DISCUSSION
We here report on a series of 50 patients who developed SRC and provide evidence that SRC remains associated with severe morbidity and mortality.
In our study, in agreement with the literature,18 43 (86%) patients had diffuse SSc. In a cohort of patients with diffuse SSc, renal crisis occurred in 129/675 (19.5%) patients.19 Unfortunately, our study is based on investigator recall, and we cannot be sure that we covered all SRC cases. Moreover, except in our centre, we do not know the total number of SSc patients followed in other centres, and therefore we cannot estimate the prevalence of SRC.
In all, 28 (56%) of our patients required haemodialysis, in agreement with the 50% reported in the literature.20 Dialysis was temporary in eight (16%) of them, confirming that patients experiencing SRC may eventually come off dialysis.20
In our study, after a mean follow-up of four years, 17 (34%) patients died. These results are in agreement with the literature.8 18 Steen and colleagues obtained excellent results at one year and attributed it to the immediate and extensive use of ACEI.18 Therefore, it seems to be very important to prescribe ACEI very early in the course of SRC, and increase the dose daily to achieve a blood pressure reduction of 10–20 mmHg systolic pressure per 24 h.18 Thus, ACEI must be prescribed even if there is a continued deterioration in renal function. In case of failure of maximal dose ACEI to normalise blood pressure, additional anti-hypertensive agents may be useful including combinations of calcium channel blockers, nitrates (especially if there is pulmonary oedema) or other vasodilator agents.20 In our study, ACEI were prescribed to 94% of patients, in association with another drug in most of the cases, calcium channel blockers being the first choice in half of them.
Steen and Medsger recently reported a dramatic reduction of mortality due to SRC.7 This result might be the consequence of the better efficacy in treating patients with SRC. Alternatively, we can hypothesise that the wide prescription of ACEI in patients with early dSSc might contribute to reduce the prevalence of SRC. Thus, in the high vs low dose D-penicillamine trial, only 2 among the 18 patients who developed SRC received AECI prior to the occurrence of SRC.8 In our study, 10 patients were on with ACEI at the time of SRC, indicating that prophylactic use of this treatment does not protect against the development of SRC. Of these patients, 6 required chronic haemodialysis, including 4 who had normotensive SRC, and 3 of them died. The proportion of patients who were exposed to ACEI prior to SRC was too small to perform statistical comparisons. As our patients received ICE inhibitor after a mean of 8.53 days, it is probable that at least in some patients the treatment was not initiated early, which could contribute to explain the severity of SRC and the high frequency of complications of hypertension. However, the duration between the first sign of SRC and the initiation did not influence the outcome of SRC.
Normotensive SRC represent 10% of SRC, are often associated with CS exposure, thrombotic microangiopathy and poor prognosis.21 ACEI were administered to 4 out of the 6 patients with normotensive SRC and could have masked it so that the patients present later in the course without hypertension. We identified blood pressure <140/90 and age >53 years as independent risk factors of bad prognosis in patients experiencing SRC, confirming data from the literature.4 21 We failed, however, to confirm other bad prognosis factors such as male gender and marked renal insufficiency, probably because of the insufficient sample size of our study.
In all, 30 (60%) patients had been exposed to CS prior to the onset of SRC. The odds ratio for developing SRC associated with intake of CS during the preceding 1- or 3-month period were 17.4 and 24.1, respectively, confirming the potential role of CS in inducing SRC. Thus, in a case–control study reported by Steen and colleagues, in the 6 months prior to SRC onset or to the first visit, high-dose CS (⩾15 mg/d prednisone or equivalent) were administered significantly more frequently in SRC patients (36%) than in controls (12%) (odds ratio 4.37).22 Taken together, and despite the fact it cannot be concluded that CS plays a causal rather than confounding role, these data support the crucial preventive role of avoiding CS in patients at risk for SRC.
Our results confirm that SRC remains associated with severe morbidity and mortality despite the use of ACEI and that CS might increase the risk of developing SRC. Early mortality in patients remains elevated, pointing out the need for establishing new therapeutic agents in addition to the immediate and extensive use of ACEI.
Acknowledgments
The authors would like to thank the following physicians for their help: Hôpital Saint Antoine, Paris: K Tiev; Hôpital Pitié Salpétriêre, Paris: C Frances, S Barete, S Trad, B Wechsler, JC Piette; Hôpital Necker, Paris: F Fakhouri, P Lesavre, JP Grunfeld; Hôpital Saint Louis, Paris: D Farge-Bancel, M Darmon, E Azoulay; Hôpital Bichat, Paris: F Mignon; Hôpital Bretonneau, Tours: E Diot, JL Guilmot; Hôpital de Bois Guillaume, Rouen: H Levesque; Hôpital Claude Huriez, Lille: D Launay, M Humbert, E Hachulla, PY Hatron; Hôpital Sud, Rennes: P Jego; Hôpital Côte de Nacre, Caen: N Artigues, Y Ollivier, P Letellier; Hôpital de la Cavale Blanche, Brest: A Cenac; Hôpital A Michallon, Grenoble: P Carpentier; Centre Hospitalier Lyon-Sud, Lyon: C Grange, H Rousset, D Vital Durand; Hôpital Gabriel Montpied, Clermont-Ferrand: I Delevaux, O Aumaìtre; Hôpital Nord, Saint-Etienne: E Alamartine, P Cathebras; Centre Hospitalier Saint-André, Bordeaux: J Constans, C Combe, P Mercié, M Longy-Boursier; Hôpital d’Instruction des Armées Saint-Anne, Toulon: C Jego, P Carli. The authors also wish to thank the following pathologists for their help: Hôpital Pitié-Salpêtrière, Paris: I Brocheriou; Hôpital Bichat, Paris: F Walker; Hôpital Claude Huriez, Lille: MC Copin; Hôpital A Michallon, Grenoble: N Pinel; Hôpital Nord, Saint-Etienne: B Laurent; Centre Hospitalier Lyon-Sud, Lyon: F Dijoud; Hôpital Jean Verdier, Bondy: L Martin. This work was presented at the 6th annual congress of European League Against Rheumatism (EULAR), 8–11 June 2005, Vienna, Austria, and at the 70th ACR/ARHP Annual Scientific Meeting, 10–15 November 2006, Washington, DC, USA.
REFERENCES
Footnotes
-
Funding: LT was supported by Actelion pharmaceutics (Paris, France)
-
Competing interests: None declared