Article Text

Abstract
Objective To develop and validate revised classification criteria for eosinophilic granulomatosis with polyangiitis (EGPA).
Methods Patients with vasculitis or comparator diseases were recruited into an international cohort. The study proceeded in five phases: (1) identification of candidate criteria items using consensus methodology, (2) prospective collection of candidate items present at the time of diagnosis, (3) data-driven reduction of the number of candidate items, (4) expert panel review of cases to define the reference diagnosis and (5) derivation of a points-based risk score for disease classification in a development set using least absolute shrinkage and selection operator logistic regression, with subsequent validation of performance characteristics in an independent set of cases and comparators.
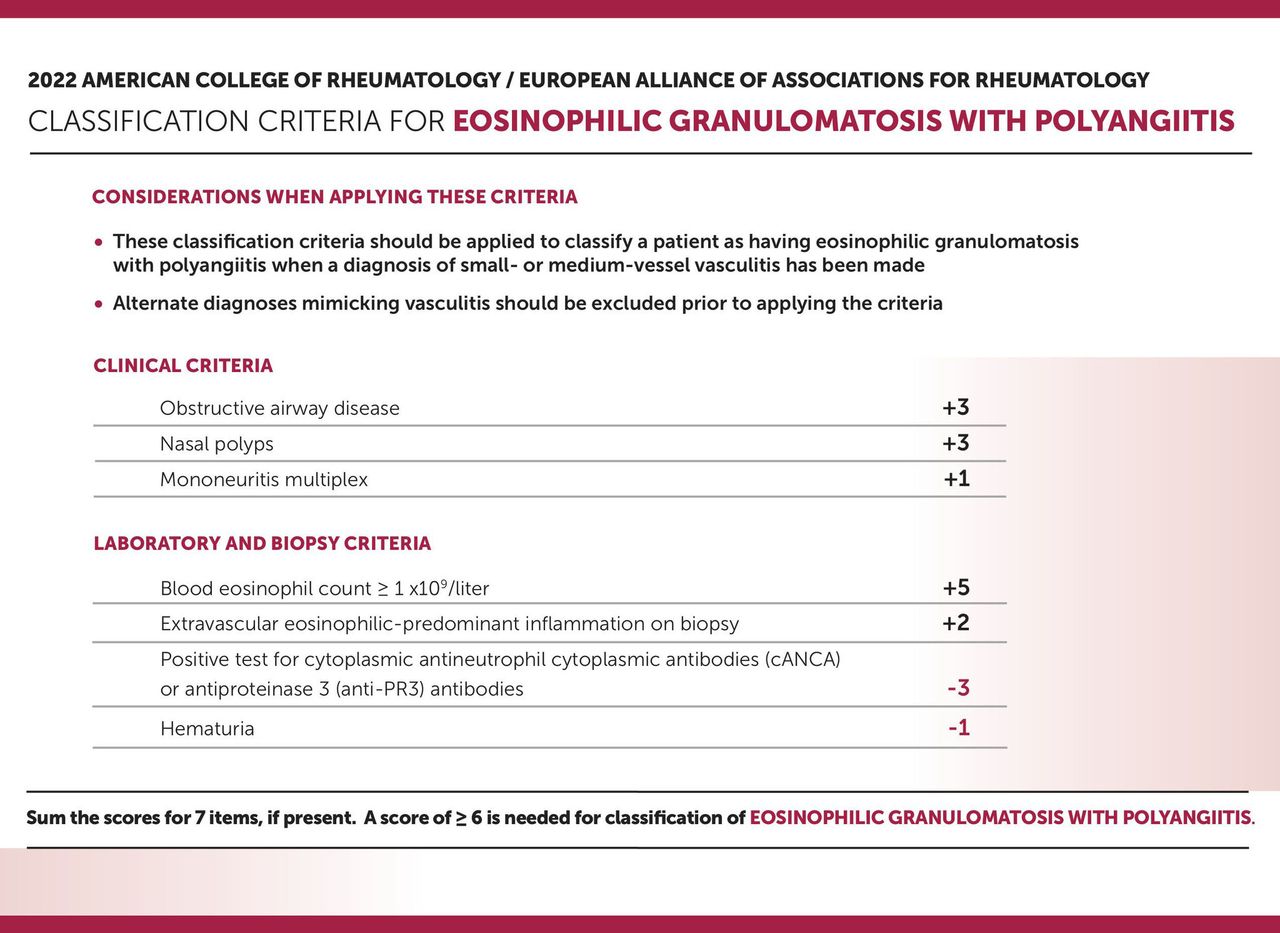
Results The development set for EGPA consisted of 107 cases of EGPA and 450 comparators. The validation set consisted of an additional 119 cases of EGPA and 437 comparators. From 91 candidate items, regression analysis identified 11 items for EPGA, 7 of which were retained. The final criteria and their weights were as follows: maximum eosinophil count ≥1×109/L (+5), obstructive airway disease (+3), nasal polyps (+3), cytoplasmic antineutrophil cytoplasmic antibody (ANCA) or anti-proteinase 3–ANCA positivity (−3), extravascular eosinophilic predominant inflammation (+2), mononeuritis multiplex/motor neuropathy not due to radiculopathy (+1) and haematuria (−1). After excluding mimics of vasculitis, a patient with a diagnosis of small- or medium-vessel vasculitis could be classified as having EGPA if the cumulative score was ≥6 points. When these criteria were tested in the validation data set, the sensitivity was 85% (95% CI 77% to 91%) and the specificity was 99% (95% CI 98% to 100%).
Conclusion The 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis demonstrate strong performance characteristics and are validated for use in research.
- autoimmune diseases
- rehabilitation
- arthritis
Statistics from Altmetric.com
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA), formerly known as Churg-Strauss syndrome, is a form of vasculitis that is histologically defined by eosinophil-rich, necrotising granulomatous inflammation primarily involving the respiratory tract, along with necrotising vasculitis of small- to medium-sized arteries.1 EGPA is considered a form of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV), along with granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA). ANCAs are detected in ~40% to 60% of patients with EGPA and are typically directed against myeloperoxidase (MPO).2 3
In 1990, the American College of Rheumatology (ACR) published classification criteria for EGPA.4 By current standards, these criteria have never been validated because they were developed using data from only 20 patients with EGPA without independent test and validation sets. Furthermore, the criteria were derived by comparing clinical data from patients with EGPA to data from 787 patients with other forms of vasculitis. Many of these comparators were patients with giant cell arteritis, a form of large-vessel vasculitis that is typically not difficult to readily distinguish from EGPA based on obvious clinical differences. Despite these methodological weaknesses, the 1990 ACR criteria for EGPA have existed unchanged for several decades and have been useful to advance clinical research in these diseases. This article outlines the development and validation of the new ACR/European Alliance of Associations for Rheumatology (EULAR)-endorsed classification criteria for EGPA.
Methods
A detailed and complete description of the methods involved in the development and validation of the classification criteria for EGPA is provided in online supplemental appendix 1. Briefly, an international steering committee comprising clinician investigators with expertise in vasculitis, statisticians and data managers was established to oversee the overall Diagnostic and Classification Criteria in Vasculitis (DCVAS) project.5 The steering committee established a five-stage plan using data-driven and consensus methodology to develop the criteria for each of six forms of vasculitis.
Supplemental material
Stage 1: generation of candidate classification items for systemic vasculitides
Candidate classification items were generated by expert opinion and were reviewed by a group of vasculitis experts across a range of specialties using a nominal group technique.
Stage 2: DCVAS prospective observational study
A prospective, international, multisite observational study was conducted (see collaborators for study investigators and sites). Consecutive patients representing the full spectrum of disease were recruited from academic and community practices. Patients were included if they were 18 years or older and had a diagnosis of vasculitis or a condition that mimics vasculitis. Patients with AAV could only be enrolled within 2 years of diagnosis. Only data present at diagnosis were recorded.
Supplemental material
Stage 3: refinement of candidate items specifically for AAV
The steering committee conducted a data-driven process to reduce the number of candidate items of relevance to cases and comparators for AAV. Items were selected for exclusion if they had a prevalence of <5% within the data set and/or they were not clinically relevant for classification criteria (eg, related to infection, malignancy or demographic characteristics). Low-frequency items of clinical importance could be combined, when appropriate.
Stage 4: expert review to derive a gold standard-defined final set of cases of AAV
Experts in vasculitis from a wide range of geographical locations and specialties reviewed all submitted cases of vasculitis and a random subset of mimics of vasculitis. Each reviewer was asked to review ~50 submitted cases to confirm the diagnosis and to specify the certainty of their diagnosis as follows: very certain, moderately certain, uncertain or very uncertain. Only cases agreed on with at least moderate certainty were retained for further analysis.
Stage 5: derivation and validation of the final classification criteria for EGPA
The DCVAS AAV data set was randomly split into development (50%) and validation (50%) sets. Comparisons were performed between cases of EGPA and a comparator group randomly selected from the DCVAS cohort in the following proportions: another type of AAV (including GPA and MPA), 60%; and another form of small-vessel vasculitis (eg, cryoglobulinemic vasculitis) or medium-vessel vasculitis (eg, polyarteritis nodosa), 40%. Least absolute shrinkage and selection operator (lasso) logistic regression was used to identify items from the data set and to create a parsimonious model including only the most important items. The final items in the model were formulated into a clinical risk-scoring tool with each factor assigned a weight based on its respective regression coefficient. A threshold that best balanced sensitivity and specificity was identified for classification.
In sensitivity analyses, the final classification criteria were applied to an unselected population of cases and comparators from the DCVAS data set based on the submitting physician diagnosis. Comparison was also made between the measurement properties of the new classification criteria for EGPA and the 1990 ACR classification criteria for EGPA using pooled data from the development and validation sets.
Results
Generation of candidate classification items for the systemic vasculitides
The steering committee identified >1000 candidate items for the DCVAS case report form (see online supplemental appendix 2, available on the Arthritis & Rheumatology website at http://onlinelibrary.wiley.com/doi/10.1002/art.41982/abstract).
DCVAS prospective observational study
Between January 2011 and December 2017, the DCVAS study recruited 6991 participants from 136 sites in 32 countries. Information on the DCVAS sites, investigators and participants is listed in online supplemental appendices 3–5, available on the Arthritis & Rheumatology website (http://onlinelibrarywileycom/doi/101002/art41982/abstract).
Refinement of candidate items specifically for AAV
Following a data-driven and expert consensus process, 91 items from the DCVAS case report form were retained for regression analysis, including 45 clinical (14 composite), 18 laboratory (two composite), 12 imaging (all composite) and 16 biopsy (one composite) items. Some clinical items were removed in favour of similar but more specific pathophysiological descriptors. For example, ‘hearing loss or reduction’ was removed, and the composite item ‘conductive hearing loss/sensorineural hearing loss’ was retained. See online supplemental appendix 6, available on the Arthritis & Rheumatology website (http://onlinelibrary.wiley.com/doi/10.1002/art.41982/abstract), for the final candidate items used in the derivation of the classification criteria for GPA, MPA and EGPA.
Expert review to derive a gold standard-defined final set of cases of AAV
Fifty-five independent experts reviewed vignettes derived from the case report forms for 2871 cases submitted with a diagnosis of either small-vessel vasculitis (90% of case report forms) or another type of vasculitis or a mimic of vasculitis (10% of case report forms). The characteristics of the expert reviewers are shown in online supplemental appendix 7. A flowchart showing the results of the expert review process is shown in online supplemental appendix 8. A total of 2072 cases (72%) passed the process and were designated as cases of vasculitis; these cases were used for the stage 5 analyses.
After expert panel review, 226 of 315 cases of EGPA were retained for subsequent analysis. Compared with patients who were retained, patients who were excluded from further analysis had significantly higher serum creatinine levels (mean±SD 102.8±88.7 vs 85.0±53.6 μmol/L, p=0.03) and lower rates of MPO-ANCA positivity (22% vs 43%, p<0.01), and were less likely to have maximum eosinophil counts ≥1×109/L (62% vs 92%, p<0.01). There were 887 comparators randomly selected for analysis. Table 1 shows the demographic and disease features of the 1113 cases included in this analysis (226 patients with EGPA and 887 comparators), of which 557 (50%, 107 patients with EGPA and 450 comparators) were in the development set and 556 (50%, 119 patients with EGPA and 437 comparators) were in the validation set.
Demographic and disease features of cases of EGPA and comparators*
Derivation and validation of the final classification criteria for EGPA
Lasso regression of the previously selected 91 items yielded 11 independent items for EGPA (online supplemental appendix 9A). Each item was then adjudicated by the DCVAS Steering Committee for inclusion based on clinical relevance and specificity to EGPA, resulting in seven final items. Weighting of an individual criterion was based on logistic regression fitted to the seven selected items (see online supplemental appendix 10A).
Model performance
Use of a cut-off of ≥6 for total risk score (see online supplemental appendix 11A for different cut points) yielded a sensitivity of 84.9% (95% CI 77.2% to 90.8%) and a specificity of 99.1% (95% CI 98.3% to 99.8%) in the validation set. The area under the curve (AUC) for the model was 0.98 (95% CI 0.97 to 1.00) in the development set and 0.99 (95% CI 0.97 to 1.00) in the validation set for the final EGPA classification criteria (online supplemental appendix 12A). The final classification criteria for EGPA are presented in figure 1 (for the slide presentation version, see online supplemental figure 1.
Supplemental material

{kind=link}
2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis.
Sensitivity analyses
The classification criteria for EGPA were applied to 2871 patients in the DCVAS database using the original physician-submitted diagnosis (n=315 EGPA and 2556 randomly selected comparators). Use of the same cut point of ≥6 points for the classification of EGPA yielded a similar specificity of 99% but a lower sensitivity of 75%. This upheld the a priori hypothesis that specificity would remain unchanged, but sensitivity would be reduced in a population of patients that included fewer clear-cut diagnoses of EGPA (ie, cases that did not pass expert panel review).
When the 1990 ACR classification criteria for EGPA were applied to the DCVAS data set, the criteria performed poorly due to low sensitivity (44%) but retained excellent specificity (99%), with an AUC of 0.72 (95% CI 0.68 to 0.75).
Discussion
Presented here are the final 2022 ACR/EULAR EGPA classification criteria. A five-stage approach has been used, underpinned by data from the multinational prospective DCVAS study and informed by expert review and consensus at each stage. The comparator group for developing and validating the criteria was patients with other forms of AAV and other small- and medium-vessel vasculitides, which are the clinical entities where discrimination from EGPA is difficult but important. The new criteria for EGPA have excellent sensitivity and specificity and incorporate ANCA testing. The criteria were designed to have face and content validity for use in clinical trials and other research studies.
These criteria are validated and intended for the purpose of classification of vasculitis and are not appropriate for use in establishing a diagnosis of vasculitis. The aim of the classification criteria is to differentiate cases of EGPA from similar types of vasculitis in research settings. Therefore, the criteria should only be applied when a diagnosis of small- or medium-vessel vasculitis has been made and all potential ‘vasculitis mimics’ have been excluded. The exclusion of mimics is a key aspect of many classification criteria, including those for Sjögren’s syndrome6 and rheumatoid arthritis.7 The 1990 ACR classification criteria for vasculitis perform poorly when used for diagnosis (ie, when used to differentiate between cases of vasculitis vs mimics without vasculitis),8 and it is expected that the 2022 criteria would also perform poorly if used inappropriately as diagnostic criteria in people in whom alternative diagnoses, such as infection or other non-vasculitis inflammatory diseases, are still being considered. Specifically, the criteria were not developed to differentiate patients with EGPA from those with other related hypereosinophilic syndromes or eosinophilic malignancies.9
The 2022 ACR/EULAR EGPA classification criteria reflect the collaborative effort of the international vasculitis community to delineate the salient clinical features that differentiate EGPA from other forms of vasculitis. The final criteria include seven clinical items that are easily assessed during routine clinical evaluation of patients with EGPA. The criteria highlight the importance of blood eosinophilia, asthma and eosinophilic inflammation to classify EGPA among other forms of vasculitis and specify additional features (eg, nasal polyps and mononeuritis multiplex) that function as important disease classifiers. Classification criteria are intended to define a homogeneous group of patients with a particular disease for inclusion into clinical research studies. By maximising specificity, the revised criteria for EGPA ensure that few cases will inappropriately meet the criteria threshold of ≥6 points; thus, these criteria will function to facilitate the conduct of future clinical trials and other studies in EGPA.
The negative items included in the final criteria underscore that these criteria are intended for use as classification, not diagnostic, criteria to differentiate EGPA from other forms of vasculitis in research settings. Both haematuria and antiproteinase 3–antineutrophil cytoplasmic antibody (anti-PR3-ANCA) function as negative items in the new EGPA classification criteria, yet glomerulonephritis and ANCA are features of disease that, when present, can be useful to diagnose EGPA. When compared with other forms of AAV, however, biopsy-proven glomerulonephritis was significantly less common in the DCVAS cohort in patients with EGPA (4.9%) compared with those with GPA (27.8%) or MPA (48.5%). Similarly, anti-PR3-ANCAs have been reported in few patients with EGPA but are much more prevalent in GPA.10 For these reasons, haematuria and anti-PR3-ANCAs work against a patient with small-vessel vasculitis being classified as having EGPA. Although anti-MPO-ANCAs can be detected in 40%–60% of patients with EGPA, anti-MPO-ANCA positivity was not included in the final criteria because these antibodies are significantly more prevalent in diseases like MPA and thus are not discriminant classifiers for EGPA.11
There are some study limitations to consider. Although this was the largest international study ever conducted in vasculitis, most patients were recruited from Europe, Asia and North America. The performance characteristics of the criteria should be further tested in African and South American populations, which may have different clinical presentations of vasculitis. These criteria were developed using data collected from adult patients with vasculitis. Although the clinical characteristics of EGPA and the other vasculitides which these criteria were tested against are not known to differ substantially between adults and children, these criteria should be applied to children with some caution. The scope of the criteria is intentionally narrow and applies only to patients who have been diagnosed as having vasculitis. Diagnostic criteria are not specified. The criteria are intended to identify homogeneous populations of disease and, therefore, may not be appropriate for studies focused on the full spectrum of clinical heterogeneity in these conditions. To maximise relevance and face validity of the new criteria, study sites and expert reviewers were recruited from a broad range of countries and different medical specialties. Nonetheless, the majority of patients were recruited from academic rheumatology or nephrology units, which could have introduced referral bias.
There are several strengths to the new 2022 ACR/EULAR EGPA classification criteria. The criteria were developed within a large cohort reflecting international expertise in systemic vasculitis according to ACR guidance for classification criteria development.11 The criteria represent several important methodological advancements compared with the original 1990 ACR classification criteria for EGPA. Expert review rather than submitting physician diagnosis was used as the diagnostic reference standard to minimise investigator bias. Second, while the 1990 ACR criteria were entirely derived from 20 patients with EGPA and were not validated, the new criteria were developed in 107 patients with EGPA and were validated in an independent test set that contained an additional 119 patients with EGPA. Third, unlike the 1990 ACR criteria, the new ACR/EULAR EGPA criteria are weighted to reflect the relative importance of specific items (eg, eosinophil counts). Finally, when both criteria sets were tested within the DCVAS cohort, the performance characteristics of the 1990 ACR criteria were suboptimal when compared with the 2022 revised ACR/EULAR EGPA criteria.
The 2022 ACR/EULAR classification criteria for EGPA are the product of a rigorous methodological process that used an extensive data set generated by the work of a remarkable international group of collaborators. These criteria have been endorsed by the ACR and EULAR and are now ready for use to differentiate one type of vasculitis from another to define populations in research studies.
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants. Ethical approval was obtained from national and local ethics committees.
Acknowledgments
We acknowledge the patients and clinicians who provided data to the Diagnostic and Classification Criteria in Vasculitis project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This article is published simultaneously in Arthritis & Rheumatology.
Collaborators The DCVAS study investigators are as follows: Paul Gatenby (ANU Medical Centre, Canberra, Australia); Catherine Hill (Central Adelaide Local Health Network: The Queen Elizabeth Hospital, Australia); Dwarakanathan Ranganathan (Royal Brisbane and Women’s Hospital, Australia); Andreas Kronbichler (Medical University Innsbruck, Austria); Daniel Blockmans (University Hospitals Leuven, Belgium); Lillian Barra (Lawson Health Research Institute, London, Ontario, Canada); Simon Carette, Christian Pagnoux (Mount Sinai Hospital, Toronto, Canada); Navjot Dhindsa (University of Manitoba, Winnipeg, Canada); Aurore Fifi-Mah (University of Calgary, Alberta, Canada); Nader Khalidi (St Joseph’s Healthcare, Hamilton, Ontario, Canada); Patrick Liang (Sherbrooke University Hospital Centre, Canada); Nataliya Milman (University of Ottawa, Canada); Christian Pineau (McGill University, Canada); Xinping Tian (Peking Union Medical College Hospital, Beijing, China); Guochun Wang (China-Japan Friendship Hospital, Beijing, China); Tian Wang (Anzhen Hospital, Capital Medical University, China); Ming-hui Zhao (Peking University First Hospital, China); Vladimir Tesar (General University Hospital, Prague, Czech Republic); Bo Baslund (University Hospital, Copenhagen [Rigshospitalet], Denmark); Nevin Hammam (Assiut University, Egypt); Amira Shahin (Cairo University, Egypt); Laura Pirila (Turku University Hospital, Finland); Jukka Putaala (Helsinki University Central Hospital, Finland); Bernhard Hellmich (Kreiskliniken Esslingen, Germany); Jörg Henes (Universitätsklinikum Tübingen, Germany); Peter Lamprecht (Klinikum Bad Bramstedt, Germany); Thomas Neumann (Universitätsklinikum Jena, Germany); Wolfgang Schmidt (Immanuel Krankenhaus Berlin, Germany); Cord Sunderkoetter (Universitätsklinikum Müenster, Germany); Zoltan Szekanecz (University of Debrecen Medical and Health Science Center, Hungary); Debashish Danda (Christian Medical College & Hospital, Vellore, India); Siddharth Das (Chatrapathi Shahuji Maharaj Medical Center, Lucknow [IP], India); Rajiva Gupta (Medanta, Delhi, India); Liza Rajasekhar (NIMS, Hyderabad, India); Aman Sharma (Postgraduate Institute of Medical Education and Research, Chandigarh, India); Shrikant Wagh (Jehangir Clinical Development Centre, Pune [IP], India); Michael Clarkson (Cork University Hospital, Ireland); Eamonn Molloy (St. Vincent’s University Hospital, Dublin, Ireland); Carlo Salvarani (Santa Maria Nuova Hospital, Reggio Emilia, Italy); Franco Schiavon (L’Azienda Ospedaliera of University of Padua, Italy); Enrico Tombetti (Università Vita-Salute San Raffaele Milano, Italy); Augusto Vaglio (University of Parma, Italy); Koichi Amano (Saitama Medical University, Japan); Yoshihiro Arimura (Kyorin University Hospital, Japan); Hiroaki Dobashi (Kagawa University Hospital, Japan); Shouichi Fujimoto (Miyazaki University Hospital [HUB], Japan); Masayoshi Harigai, Fumio Hirano (Tokyo Medical and Dental University Hospital, Japan); Junichi Hirahashi (University Tokyo Hospital, Japan); Sakae Honma (Toho University Hospital, Japan); Tamihiro Kawakami (St. Marianna University Hospital Dermatology, Japan); Shigeto Kobayashi (Juntendo University Koshigaya Hospital, Japan); Hajime Kono (Teikyo University, Japan); Hirofumi Makino (Okayama University Hospital, Japan); Kazuo Matsui (Kameda Medical Centre, Kamogawa, Japan); Eri Muso (Kitano Hospital, Japan); Kazuo Suzuki, Kei Ikeda (Chiba University Hospital, Japan); Tsutomu Takeuchi (Keio University Hospital, Japan); Tatsuo Tsukamoto (Kyoto University Hospital, Japan); Shunya Uchida (Teikyo University Hospital, Japan); Takashi Wada (Kanazawa University Hospital, Japan); Hidehiro Yamada (St. Marianna University Hospital Internal Medicine, Japan); Kunihiro Yamagata (Tsukuba University Hospital, Japan); Wako Yumura (IUHW Hospital [Jichi Medical University Hospital], Japan); Kan Sow Lai (Penang General Hospital, Malaysia); Luis Felipe Flores- Suarez (Instituto Nacional de Enfermedades Respiratorias, Mexico City, Mexico); Andrea Hinojosa (Instituto Nacional de Ciencias Médicas y Nutricion Salvador Zubiran, Mexico City, Mexico); Bram Rutgers (University Hospital Groningen, Netherlands); Paul-Peter Tak (Academic Medical Centre, University of Amsterdam, Netherlands); Rebecca Grainger (Wellington, Otago, New Zealand); Vicki Quincey (Waikato District Health Board, New Zealand); Lisa Stamp (University of Otago, Christchurch, New Zealand); Ravi Suppiah (Auckland District Health Board, New Zealand); Emilio Besada (Tromsø, Northern Norway, Norway); Andreas Diamantopoulos (Hospital of Southern Norway, Kristiansand, Norway); Jan Sznajd (University of Jagiellonian, Poland); Elsa Azevedo (Centro Hospitalar de S~ao Jo~ao, Porto, Portugal); Ruth Geraldes (Hospital de Santa Maria, Lisbon, Portugal); Miguel Rodrigues (Hospital Garcia de Orta, Almada, Portugal); Ernestina Santos (Hospital Santo Antonio, Porto, Portugal); Yeong-Wook Song (Seoul National University Hospital, Republic of Korea); Sergey Moiseev (First Moscow State Medical University, Russia); Alojzija Hocˇevar (University Medical Centre Ljubljana, Slovenia); Maria Cinta Cid (Hospital Clinic de Barcelona, Spain); Xavier Solanich Moreno (Hospital de Bellvitge-Idibell, Spain); Inoshi Atukorala (University of Colombo, Sri Lanka); Ewa Berglin (Umeå University Hospital, Sweden); Aladdin Mohammed (Lund-Malmo University, Sweden); Mårten Segelmark (Linköping University, Sweden); Thomas Daikeler (University Hospital Basel, Switzerland); Haner Direskeneli (Marmara University Medical School, Turkey); Gulen Hatemi (Istanbul University, Cerrahpasa Medical School, Turkey); Sevil Kamali (Istanbul University, Istanbul Medical School, Turkey); Ömer Karadag (Hacettepe University, Turkey); Seval Pehlevan (Fatih University Medical Faculty, Turkey); Matthew Adler (Frimley Health NHS Foundation Trust, Wexham Park Hospital, UK); Neil Basu (NHS Grampian, Aberdeen Royal Infirmary, UK); Iain Bruce (Manchester University Hospitals NHS Foundation Trust, UK); Kuntal Chakravarty (Barking, Havering and Redbridge University Hospitals NHS Trust, UK); Bhaskar Dasgupta (Southend University Hospital NHS Foundation Trust, UK); Oliver Flossmann (Royal Berkshire NHS Foundation Trust, UK); Nagui Gendi (Basildon and Thurrock University Hospitals NHS Foundation Trust, UK); Alaa Hassan (North Cumbria University Hospitals, UK); Rachel Hoyles (Oxford University Hospitals NHS Foundation Trust, UK); David Jayne (Cambridge University Hospitals NHS Foundation Trust, UK); Colin Jones (York Teaching Hospitals NHS Foundation Trust, UK); Rainer Klocke (The Dudley Group NHS Foundation Trust, UK); Peter Lanyon (Nottingham University Hospitals NHS Trust, UK); Cathy Laversuch (Taunton & Somerset NHS Foundation Trust, Musgrove Park Hospital, UK); Raashid Luqmani, Joanna Robson (Nuffield Orthopaedic Centre, Oxford, UK); Malgorzata Magliano (Buckinghamshire Healthcare NHS Trust, UK); Justin Mason (Imperial College Healthcare NHS Trust, UK); Win Win Maw (Mid Essex Hospital Services NHS Trust, UK); Iain McInnes (NHS Greater Glasgow & Clyde, Gartnavel Hospital & GRI, UK); John Mclaren (NHS Fife, Whyteman’s Brae Hospital, UK); Matthew Morgan (University Hospitals Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, UK); Ann Morgan (Leeds Teaching Hospitals NHS Trust, UK); Chetan Mukhtyar (Norfolk and Norwich University Hospitals NHS Foundation Trust, UK); Edmond O’Riordan (Salford Royal NHS Foundation Trust, UK); Sanjeev Patel (Epsom and St Helier University Hospitals NHS Trust, UK); Adrian Peall (Wye Valley NHS Trust, Hereford County Hospital, UK); Joanna Robson (University Hospitals Bristol NHS Foundation Trust, UK); Srinivasan Venkatachalam (The Royal Wolverhampton NHS Trust, UK); Erin Vermaak, Ajit Menon (Staffordshire & Stoke on Trent Partnership NHS Trust, Haywood Hospital, UK); Richard Watts (East Suffolk and North Essex NHS Foundation Trust, UK); Chee-Seng Yee (Doncaster and Bassetlaw Hospitals NHS Foundation Trust, UK); Daniel Albert (Dartmouth-Hitchcock Medical Center, US); Leonard Calabrese (Cleveland Clinic Foundation, US); Sharon Chung (University of California, San Francisco, US); Lindsy Forbess (Cedars-Sinai Medical Center, US); Angelo Gaffo (University of Alabama at Birmingham, US); Ora Gewurz-Singer (University of Michigan, US); Peter Grayson (Boston University School of Medicine, US); Kimberly Liang (University of Pittsburgh, US); Eric Matteson (Mayo Clinic, US); Peter A. Merkel (University of Pennsylvania, US); Jason Springer (University of Kansas Medical Center Research Institute, US); and Antoine Sreih (Rush University Medical Center, US).
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. PAM had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study conception and design: PCG, CP, RS, JR, AC, AJ, AH, RAL, RAW and PAM. Acquisition of data. PCG, CP, RS, JR, AC, RAL, RAW and PAM. Analysis and interpretation of data. PCG, CP, RS, JR, AC, AJ, SK, AH, RAL, RAW and PAM.
Funding The Diagnostic and Classification Criteria in Vasculitis study, of which the development of these classification criteria was a part, was funded by grants from the American College of Rheumatology, the European Alliance of Associations for Rheumatology, the Vasculitis Foundation and the University of Pennsylvania Vasculitis Center.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.