Article Text

Abstract
Objectives Congenital laryngomalacia (CLM) is the major cause of stridor in infants. Most cases are expected to resolve before 2 years of age, but long-term respiratory prospects are poorly described. We aimed to investigate if CLM was associated with altered laryngeal structure or function in later life.
Methods Twenty of 23 (87%) infants hospitalised at Haukeland University Hospital during 1990–2000 for CLM without comorbidities and matched controls were assessed at mean age 13 years. Past and current respiratory morbidity was recorded in a questionnaire, and spirometry performed according to standard quality criteria. Laryngoscopy was performed at rest and continuously throughout a maximal treadmill exercise test (continuous laryngoscopy exercise test (CLE-test)), and scored and classified in a blinded fashion according to preset criteria.
Results In the CLM group, laryngeal anatomy supporting CLM in infancy was described at rest in nine (45%) adolescents. Eleven (55%) reported breathing difficulties in relation to exercise, of whom 7 had similarities to CLM at rest and 10 had supraglottic obstruction during CLE-test. Overall, 6/20 had symptoms during exercise and similarities to CLM at rest and obstruction during CLE-test. In the control group, one adolescent reported breathing difficulty during exercise and two had laryngeal obstruction during CLE-test. The two groups differed significantly from each other regarding laryngoscopy scores, obtained at rest and during exercise (p=0.001 or less).
Conclusions CLM had left footprints that increased the risk of later exercise-induced symptoms and laryngeal obstruction. The findings underline the heterogeneity of childhood respiratory disease and the importance of considering early life factors.
- Exercise induced inspiratory symptoms
- Congenital laryngomalacia
- Vocal cord dysfunction
- Respiratory Disorders
- Follow-up study
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Exercise induced inspiratory symptoms
- Congenital laryngomalacia
- Vocal cord dysfunction
- Respiratory Disorders
- Follow-up study
What is already known on this topic?
Congenital laryngomalacia (CLM) is a major cause of stridor in infants.
CLM is considered a benign and self-limiting condition, with breathing difficulties proposed to resolve by the age of 12–24 months.
Long-term respiratory prospects are poorly described in the literature.
What this study adds?
Congenital laryngomalacia (CLM) seems to leave structural and functional footprints with increased risk of later exercise-induced respiratory symptoms and laryngeal obstruction.
Most adolescents with CLM in infancy had laryngoscopic reminiscents of CLM at rest, and breathing difficulties and laryngeal obstruction during exercise.
The findings underscore the heterogeneity of childhood respiratory disease and the importance of considering early life factors.
Introduction
Congenital laryngomalacia (CLM) is the most common cause of inspiratory stridor in infants, and is characterised by dynamic inward folding of the supraglottic part of the larynx during inspiration.1 The characteristic low-pitched stridor, inspiratory retractions and feeding difficulties typically appear during the first few weeks of life and flexible laryngoscopy is the diagnostic gold standard.2 The pathophysiology of CLM is not well understood, but various forms of anatomical, physiological or neuromuscular laryngeal abnormalities have been suggested.1–5 Surgical treatment is indicated when the obstruction compromises ventilation to the extent that it causes failure to thrive, which occurs in a minority of cases.6–11 Thus, for most patients, CLM is considered a benign and self-limiting condition, and the literature proposes that breathing difficulties resolve by the age of 12–24 months.1–3 ,5 ,9 ,11 Although cases of stridor may persist beyond this age, few studies have addressed long-term outcomes from CLM.3 ,7 ,10 ,12
Exercise-induced inspiratory symptoms (EIIS) is increasingly recognised as an important differential diagnosis to exercise-induced asthma in otherwise healthy adolescents.13–15 EIIS is most often linked to laryngeal abnormalities,13 ,14 ,16–20 and if so, often labelled exercise-induced laryngeal obstruction (EILO).19 ,21–23 In unselected populations, EILO has been found in 7.5% and 5.7% of adolescents.19 ,22 Causal mechanisms remain unclear, but abnormalities related to the epiglottis, the laryngeal cartilage skeleton or its support, mucosal or muscular structures may all conceivably disturb airflow, increase the turbulence and airflow resistance and thereby explain the symptoms. Smith et al suggested a relation between CLM and later EILO, and introduced the term exercise-induced laryngomalacia.24
The aims of the present study were to assess adolescents hospitalised for CLM in infancy with respect to respiratory symptoms and laryngeal abnormalities by means of questionnaires, spirometry and laryngoscopy performed at rest and during exercise. Findings were compared with control subjects with no previous history of CLM.
Methods
Infants hospitalised at the Paediatric Department of Haukeland University Hospital in western Norway during 1990–2000 with a diagnosis of CLM without major comorbidities were invited to participate, based on the hospital computerised patient administrative systems. Comorbidities were defined as various syndromes or congenital malformations known to be associated with CLM.25 Healthy control subjects matched for age and sex were recruited from a local sports club. The regional ethics committee approved the study. All patients and controls and their guardians signed a written consent.
Medical history and background data
The medical history relating to the hospitalisation for CLM was obtained from hospital records. Later medical history, use of medication, physical performance and level of daily physical activity were obtained using a standardised questionnaire.
Spirometry
Flow-volume loops (FVLs) were measured with Vmax 22 spirometer (SensorMedics, Anaheim, USA) in accordance with standard quality criteria.26 Forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and forced expiratory flow at 25–75% of FVC (FEF25–75) were recorded and reported as percentages of predicted.27 Forced inspiratory flow in 1 s (FIV1) and at 50% (FIF50%) of forced inspiratory volume capacity were recorded and FEF50/FIF50 and FEV1/FIV1 were calculated and classified as abnormal if exceeding 1.5, as suggested by Rundell and Spiering.15 The configuration of the FVLs were classified as normal or abnormal by an experienced respiratory physiologist (ODR) based on flattening or truncation of the inspiratory limbs, as suggested by Boris et al.28 The rater was not blinded to the status of the participants.
Laryngoscopy at rest
Video recordings from all participants were presented in random order to a blinded experienced otolaryngologist (J-HH), who used a simple classification system to identify anatomical characteristics that were judged to represent parts of the infantile CLM diagnosis.1 The classification system was based on the presence or absence of the following: Prominent cuneiform tubercles and/or redundant mucosa at the arytaenoid region and/or a prominent ω-shaped epiglottis and/or both of the aforementioned characteristics. Positive findings at rest required findings both at the arytaenoid region and the epiglottis.
Continuous laryngoscopy performed during exercise (CLE-test)
An integrated set-up for continuous video-recorded laryngoscopy throughout a maximal cardiopulmonary exercise test, coupled with video recordings of the upper part of the body and sound recordings was applied.29 The patients ran on a treadmill (Woodway ELG 70, Weil am Rhein, Germany) using a modified ramp-protocol, increasing speed and/or elevation every 1 min, aiming at maximum exercise capacity after 6–12 min. The test was considered successful if the patient continued until exhaustion, preferably supported by a plateau in oxygen consumption and/or the heart rate response, or until stopped by respiratory distress. Video recordings were evaluated based on the continuous laryngoscopy exercise (CLE) score developed by Maat et al30 (figure 1). CLE sum-score (Maat-E) of at least 3 was considered consistent with EILO.30 As CLM involves supraglottic structures, and as we primarily wished to address the laryngeal response to high intensity exercise, we also applied a modified Maat score, emphasising only supraglottic findings at maximum intensity (Maat-D). A diagnosis of supraglottic EILO required a Maat-D score of 2 or 3 on a scale from 0 to 3. All assessments were done retrospectively in a blinded fashion from video recordings presented in random order to an experienced otolaryngologist (J-HH). Findings at rest in some, challenged blinded assessment of the CLE-test.
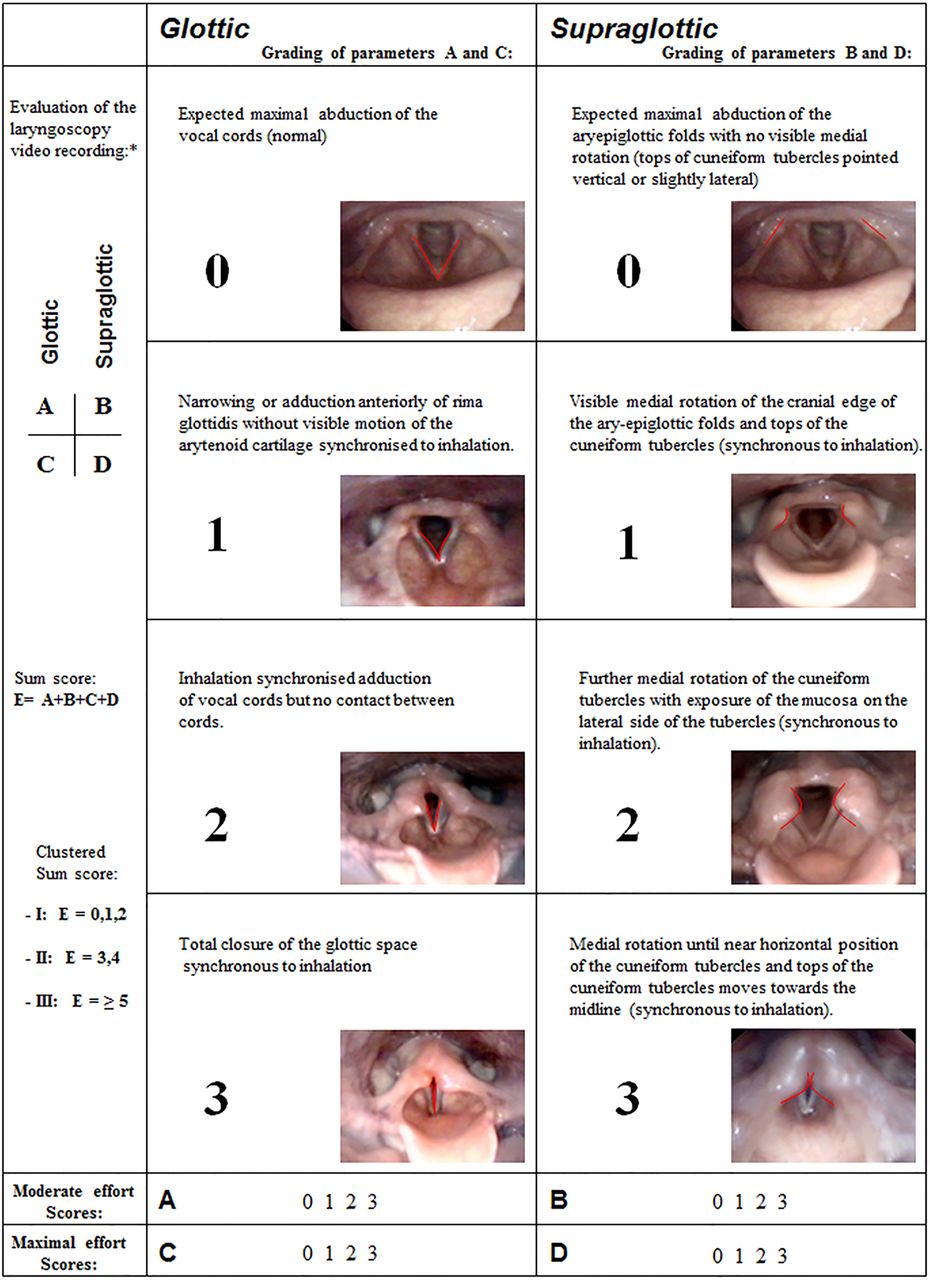
The score system (Maat score) used to describe findings during continuous laryngoscopy exercise test (CLE-test). *The scores at each level (glottic (A and C) and supraglottic (B and D)) were assessed at moderate (A and B) (when subject started to run) and at maximal effort (C and D) (just before the subject stopped running at the treadmill); all four numbers (A–D) were noted together with a sum score (E) for each test/subject (Adapted from Eur Arch Othorhinolaryngol30).
Statistical analyses
Histograms for the distribution of the background and lung function variables were plotted, and visual inspection was used to ensure that t tests were appropriate when testing for differences between groups, and that means and SDs were appropriate summary statistics. Fisher's exact test was used to test categorical data. For the CLE-scores we calculated medians and IQRs, and used the Wilcoxon's rank-sum test to assess differences between the CLM and control groups. Symptoms and findings at laryngoscopy were illustrated with Venn diagrams using dichotomised terms (figure 3). Two-tailed p<0.05 was considered statistically significant.
Results
Subjects
Thirty-one subjects were initially identified, of whom eight were excluded as they had presented with comorbidities as infants. Of the remaining 23 subjects, 2 declined and 1 was excluded due to supraglottoplasty performed in infancy, leaving 20 (87%) participants (age range 10–19 years, mean age 12.7 years, male:female=13:7). Mean age at diagnosis was 6.6 (range 0–18) weeks. Presenting symptoms in infancy were inspiratory stridor in 20 (100%), sternal retractions in 14 (70%) and varying degrees of feeding difficulties in 14 (70%). The diagnosis of CLM was verified by laryngoscopy in 9 (45%) patients. Chest X-ray was done in 17 participants of whom 16 were normal and 1 suggested pneumonia. Oesophageal pH measurement was performed in six infants of whom one suggested acidic reflux whereas one bronchoscopy revealed right middle lobe syndrome. Twenty healthy controls were recruited (age range 11–16 years, mean 13.8 years, male:female=12:8). Demographic characteristics, lung function data and findings from the maximum cardiopulmonary exercise test were similar in the CLM and the control groups, except for a lower mean maximal heart rate in those with a history of CLM (table 1).
Background data for 20 subjects hospitalised for congenital laryngomalacia (CLM) and 20 healthy control subjects with no such history
Respiratory symptoms and treatments
A history of treatment with asthma medication was more common in the CLM group (table 2). Eleven (55%) of the 20 patients with former CLM reported breathing difficulties in relation to exercise compared with 1 (5%) control.
Medical history, respiratory symptoms, diagnosis and laryngeal findings in 20 adolescents hospitalised for congenital laryngomalacia (CLM) and 20 healthy control subjects with no such history
Spirometric and laryngeal findings at rest
Abnormal configuration of FVLs was described in eight (40%) subjects in the CLM group compared with one control subject. FEF50/FIF50 and FEV1/FIV1 ratios exceeding 1.5 were seen in, respectively, four and three CLM subjects and in one control.
Laryngoscopy at rest showed characteristics resembling laryngomalacia (findings observed in both the epiglottis and in the arytaenoid region) in nine (45%) patients with former CLM and in no control subject (table 2).
Laryngeal findings during exercise
Median CLE-scores (IQR) for the CLM versus the control group for Maat-E (CLE-sum scores) were 3 (1.5–3.5) vs 1 (0–1), respectively (p=0.002), and for supraglottic findings at maximum intensity exercise (Maat-D) 2 (1–2) vs 1 (0–1), respectively (p<0.001), illustrated in figure 2. The difference between the groups was mainly caused by supraglottic scores, and the effect of Maat-E was almost fully explained by Maat-D (figure 2).

Scores of laryngeal movements obtained during a continuous laryngoscopy exercise test (CLE-test) in 20 adolescents hospitalised for congenital laryngomalacia (CLM) and 20 healthy control subjects with no such history. The left graph (Maat-D) depicts scores for supraglottic movements during maximal exercise. The right graph (Maat-E) depicts a total score from the CLE-test. The boxes show IQRs, with bold lines denoting medians. Vertical bars denote minimum and maximum scores.
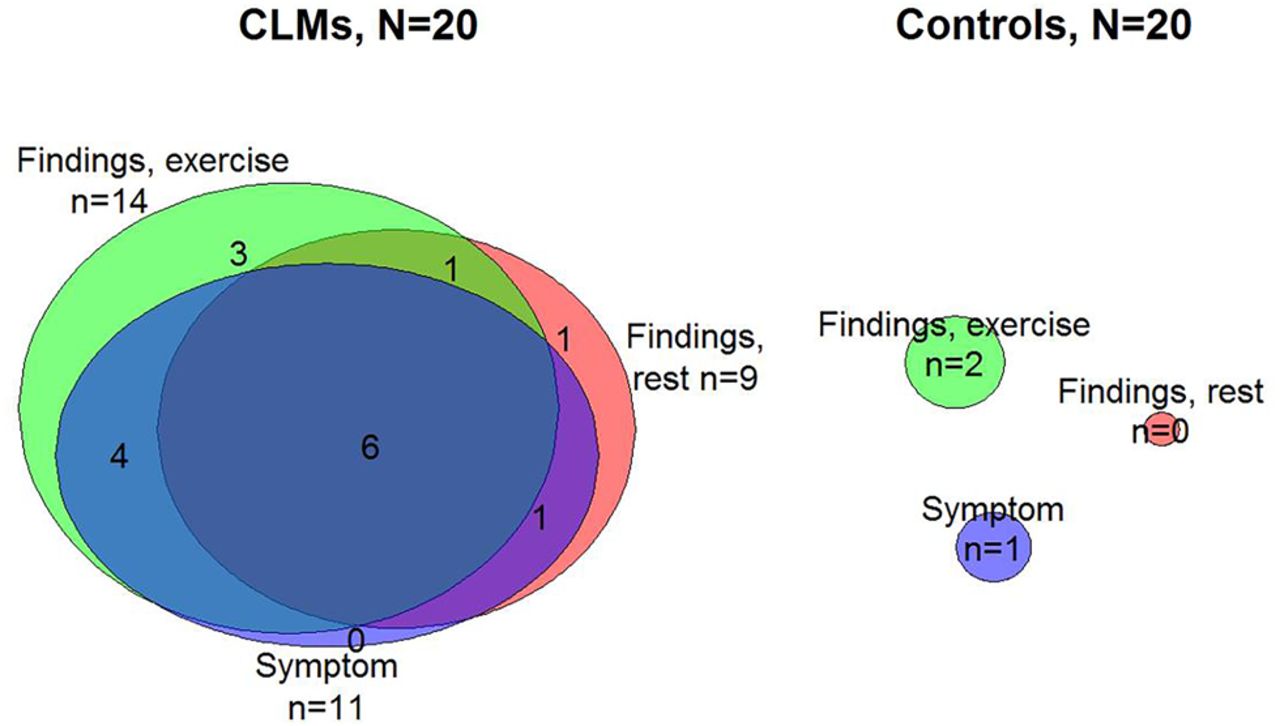
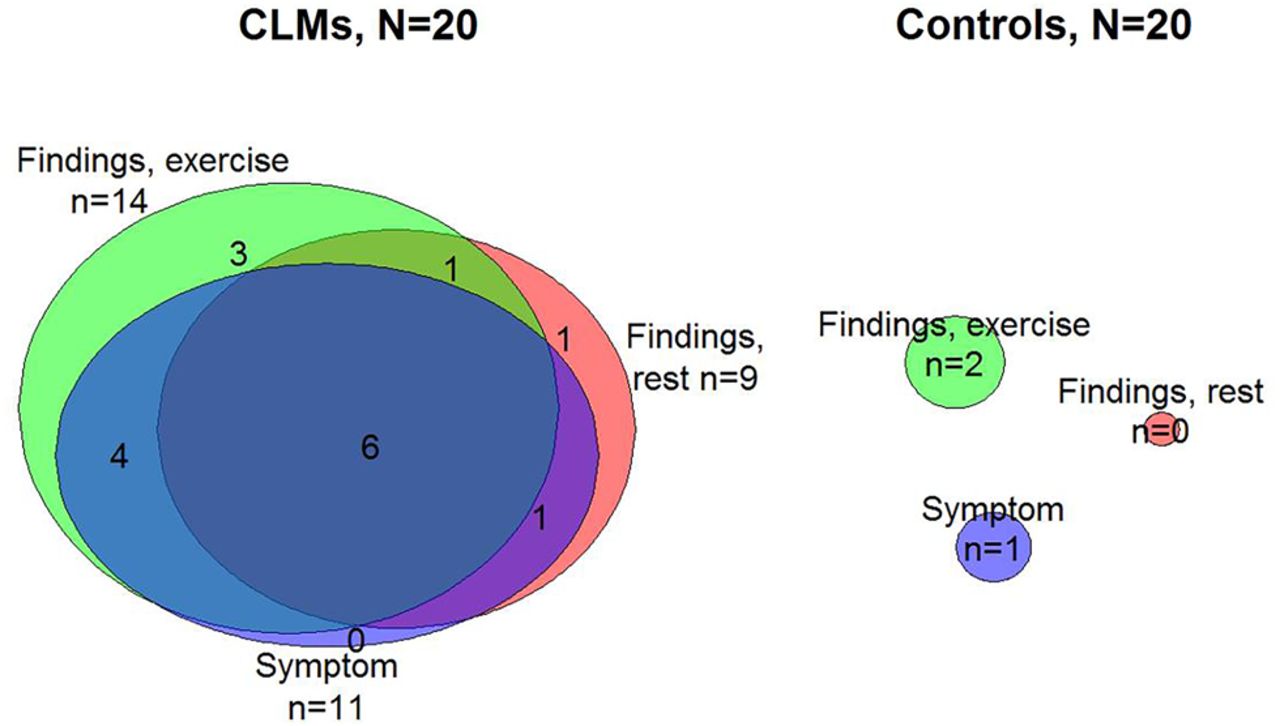
Laryngeal obstruction at maximal exercise (figure 3) consistent with supraglottic EILO (Maat-D) was observed in 14 (70%) subjects in the CLM group and in 2 (10%) subjects in the control group. Ten (50%) subjects reporting respiratory distress during physical exercise had supraglottic EILO according to the CLE-tests. Six (30%) subjects in the CLM-group reported respiratory distress in relation to exercise, exhibited laryngeal anatomy at rest likely to represent similarities to laryngomalacia and performed a CLE-test consistent with supraglottic EILO. In the control group, one subject reported respiratory distress during exercise, but had normal findings at the CLE-test. The overlapping nature of symptoms and findings is depicted in figure 3.
{kind=link}
{kind=link}
{kind=link}
Venn diagrams depicting occurrence of self-reported dyspnoea during exercise, and laryngeal findings at rest and during exercise. Findings, exercise: Maat-D score of 2 or 3 at maximum exercise during the continuous laryngoscopy exercise test (CLE-test). Findings, rest: Prominent arytaenoids and epiglottis at rest. Symptoms: Self-reported dyspnoea during exercise. The areas of the circles are proportional to the number of subjects (n) with the condition in question. Overlapping areas indicate subjects with two or three findings.
Discussion
To the best of our knowledge, this is the first study in which patients hospitalised for CLM in infancy have been systematically examined in adolescence. We found that 11/20 subjects reported breathing difficulties during exercise, 9/20 were judged to have laryngeal similarities to CLM at laryngoscopy performed at rest, while 14/20 had supraglottic laryngeal obstruction during high intensity exercise. Overlapping abnormalities were observed in 6/20, that is, they had symptoms during exercise, laryngoscopic similarities to CLM at rest and laryngeal obstruction during high intensity exercise. The number of findings clearly exceeded those of the control group.
Strength and weaknesses of the study
The strength of this study was high attendance from infancy to adolescence in a group of patients diagnosed and hospitalised in one single paediatric unit. The risk of including patients with malformations other than CLM was reduced by excluding subjects with known comorbidities. It was a weakness that CLM had not been verified by laryngoscopy in half of the participants. However, given the setting at a university paediatric unit with only experienced paediatricians assigning a final diagnosis, clinical assessment of CLM should be fairly uncomplicated in most cases. Moreover, if a diagnosis of CLM was assigned erroneously in infants with other respiratory disorders, no later findings of CLM would have been expected; that is, the ratio of positive findings should at least be as high as observed in the present study. Regrettably, declines in the control group interfered with the intended matched structure of the study. As the study was institution based and included relatively few participants, who had all been hospitalised, firm conclusions on the prevalence of abnormalities after CLM cannot be made. However, the data represent important hypothesis generating findings that underline the heterogeneity of childhood respiratory disease, and the importance of considering early life factors in the diagnostic workup. The study certainly indicates a need for larger and preferably prospective studies. Asthma was not particularly searched for and respiratory symptoms at follow-up may therefore be due to footprints from CLM or asthma or both. The choice of recruiting a control group from local sports clubs may have increased the number of healthy subjects. This may have led to less symptoms and findings in this group and therefore contributed to some of the group differences that we observed. Ideally the control group should have been drawn at random.
The literature on long-term follow-up after CLM in infancy is scarce. Laryngoscopy during exercise has only been reported in a subset of three patients with exercise-induced symptoms who participated in a study of what the authors called late-onset laryngomalacia, confirming the diagnosis in two of them.31 Smith and Cooper10 reported spirometric findings compatible with variable extrathoracic airway obstruction in 6/20 children (mean age 8 years) with former CLM. Laryngoscopy was not performed, but the results are comparable to those of the present study. Friedman et al12 reported stridor after CLM for longer than 18 months in 3/18 subjects in a group followed to an average age of 2.7 years. Macfarlane et al3 reported exercise-induced stridor in 3/20 subjects 8–16 years after endoscopically verified CLM, but laryngoscopy was not performed in relation to the follow-up.
In infancy, CLM is characterised by dynamic inward folding of the supraglottic part of the larynx during inspiration, but symptoms usually resolve before 2 years of age.1–3 ,5 ,9 ,11 It is reasonable to assume that the degree of symptoms is inversely related to the cross-sectional area of the laryngeal opening. Conceivably, a narrow larynx in an adolescent with footprints from a former laryngomalacia will more easily collapse and/or cause obstruction during exercise than at rest due to increased airflow, potentially increasing turbulence and airway resistance and thereby also increased negative pressure within the laryngeal lumen due to the Bernoulli effect.32 Findings during heavy exercise compatible with this scenario have been documented in other patient groups in several articles published by our group.14 ,23 ,29 ,30 In contrast to laryngoscopy at rest which only gives structural information and limited information on function, the CLE-test allows continuous visualisation of the larynx as symptoms evolve with increasing exercise and airflow. Laryngeal obstruction at peak exercise occurred more often (70%) than findings by laryngoscopy at rest (45%), underlining the importance of investigating these patients during ongoing exercise.
Late-onset laryngomalacia is a term that has been applied to describe patients participating in several studies in the last decades.10 ,33 Gessler34 was the first to name the term, adding to the previously described congenital, acquired and exercise-induced types of laryngomalacia. The aetiology remains unclear, but CLM usually appears with relatively modest symptoms and late-onset laryngomalacia may conceivably represent long-term consequences of milder or even undiagnosed forms of CLM, a theory that might be worth exploring.
The findings of the present study challenge the notion that spontaneous recovery from CLM should be expected in all patients. However, the participants of the present study had all been hospitalised, indicating a bias towards more severe disease than average. On the other hand, according to their medical records they were still not considered candidates for surgical treatment, and they were all discharged after a few days, when their respiratory and nutritional status had been assessed as satisfactory and the parents were assured that they could handle the situation at home. The findings therefore suggest that symptoms of CLM may fade and even disappear as the size of the laryngeal lumen increases and subsequently recur later in life when laryngeal function is challenged by high airflows caused by strenuous exercise. The clinical implication is that parents ought to be informed about the possibility of later exercise-induced obstruction. This is important in order to avoid diagnostic errors and futile treatments, as illustrated by the common use of asthma medication in the present study. The exercise data showed lower peak heart rate, and also an insignificant tendency for lower peak exercise capacity in the CLM group. Thus, despite the footprints of CLM observed in these children, they seemed to have enough ventilatory capacity to develop normal exercise capacity during their childhood.
Conclusion
CLM seems to leave structural and functional footprints in the larynx, with increasing risks of later exercise-induced symptoms and laryngeal obstruction. The findings underline the heterogeneity of childhood respiratory disease and the importance of considering early life factors when performing diagnostic workup.
References
Footnotes
Contributors MH conceptualised and designed the study, took part in data collection, performed the analyses, drafted the initial manuscript, and approved the final manuscript as submitted. ODR took part in conceptualisation and design of the study, was the main respiratory technician of the study, took part in interpretation of the analyses, drafted the manuscript for important intellectual content, and approved the final manuscript as submitted. LS took part in data collection and approved the final manuscript as submitted. ØH was the responsible statistician of the study. HJA, TH and J-HH took part in conceptualisation and design of the study, analyses and interpretations, drafting the manuscript for important intellectual content, and approved the final manuscript as submitted. J-HH was the guarantor of the study.
Funding Haukeland University Hospital, Bergen, Norway.
Competing interests None declared.
Ethics approval REC West—Secretariat—Regional Committee for Medical and Health research Ethics. 2009/1259/REK vest.
Provenance and peer review Not commissioned; externally peer reviewed.