Mapping conflict of interests: scoping review
BMJ 2021; 375 doi: https://doi.org/10.1136/bmj-2021-066576 (Published 03 November 2021) Cite this as: BMJ 2021;375:e066576Linked Opinion
Managing conflicts of interest in healthcare: the new frontier

- Susan Chimonas, qualitative research consultant12,
- Maha Mamoor, research data analyst12,
- Sophia A Zimbalist, research data analyst12,
- Brooke Barrow, medical student3,
- Peter B Bach, director and chief medical officer124,
- Deborah Korenstein, chief attending25
- 1Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY, USA
- 2Center for Health Policy and Outcomes, Memorial Sloan Kettering Cancer Center, 485 Lexington Avenue, New York, NY 10017, USA
- 3Warren Alpert Medical School, Brown University, Providence, RI, USA
- 4Delfi Diagnostics, Baltimore, MD, USA
- 5Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA
- Correspondence to: S Chimonas chimonas{at}mskcc.org
- Accepted 16 October 2021
Abstract
Objective To identify all known ties between the medical product industry and the healthcare ecosystem.
Design Scoping review.
Methods From initial literature searches and expert input, a map was created to show the network of medical product industry ties across parties and activities in the healthcare ecosystem. Through a scoping review, the ties were then verified, cataloged, and characterized, with data abstracted on types of industry ties (financial, non-financial), applicable policies for conflict of interests, and publicly available data sources.
Main outcome measures Presence and types of medical product industry ties to activities and parties, presence of policies for conflict of interests, and publicly available data.
Results A map derived through synthesis of 538 articles from 37 countries shows an extensive network of medical product industry ties to activities and parties in the healthcare ecosystem. Key activities include research, healthcare education, guideline development, formulary selection, and clinical care. Parties include non-profit entities, the healthcare profession, the market supply chain, and government. The medical product industry has direct ties to all parties and some activities through multiple pathways; direct ties extend through interrelationships among parties and activities. The most frequently identified parties were within the healthcare profession, with individual professionals described in 422 (78%) of the included studies. More than half (303, 56%) of the publications documented medical product industry ties to research, with clinical care (156, 29%), health professional education (145, 27%), guideline development (33, 6%), and formulary selection (8, 1%) appearing less often. Policies for conflict of interests exist for some financial and a few non-financial ties; publicly available data sources seldom describe or quantify these ties.
Conclusions An extensive network of medical product industry ties to activities and parties exists in the healthcare ecosystem. Policies for conflict of interests and publicly available data are lacking, suggesting that enhanced oversight and transparency are needed to protect patient care from commercial influence and to ensure public trust.
Introduction
In an influential 2009 report, the Institute of Medicine described a multifaceted healthcare ecosystem rife with industry influence.1 Central to the ecosystem are healthcare providers, researchers, clinical care facilities, journals, professional societies, and other healthcare institutions and supporting organizations engaged in medicine’s core professional activities: providing beneficial care to patients, conducting valid research, and providing evidence based clinical education and guidance. In so doing, these individuals and institutions frequently collaborate with pharmaceutical, medical device, and biotechnology product manufacturers.12345 Although these for profit entities play a crucial role in the ecosystem, particularly in developing new tests and treatments, their primary objective is to ensure financial returns to shareholders. Thus, industry collaborations inevitably introduce potential commercial bias into the healthcare ecosystem. With absent rigorous conflict of interest oversight across the entire system, the Institute of Medicine warned that medicine’s extensive ties to the medical product industry “threaten the integrity of scientific investigations, the objectivity of medical education, the quality of patient care, and the public’s trust in medicine.”1
Controlling conflict of interest across the ecosystem, however, requires a system level understanding of how influence can enter and circulate through it. Research on the influence of the medical product industry is voluminous and expanding, aided in no small part by new data sources such as Open Payments,6789 a US federal database that makes public nearly all payments to physicians and teaching hospitals by pharmaceutical, medical device, and other healthcare product manufacturers. Other lines of inquiry have begun to explore the ties between medical product companies and regulators, patient advocacy groups, and other influential parties in the healthcare ecosystem.34101112 And the analytic lens has broadened to include not only financial ties but also non-financial ones, such as medical product manufacturers offering healthcare professionals research data, authorship, and other opportunities for professional advancement.131415
Yet, with few exceptions,121617 most analyses focus on one or two narrow types of ties between the medical product industry and a single party, such as healthcare professionals, hospitals, or journals, or a single activity, such as research, education, or clinical care. The reality is that companies take a multipronged approach to developing and marketing products, enlisting the assistance of multiple influential parties throughout the healthcare ecosystem. The US opioid epidemic, for example, provides numerous instances of pharmaceutical manufacturers strategically developing financial ties with multiple entities in the healthcare ecosystem and leveraging those to create secondary influences, resulting in profound patient harm.1617 The complex interactions evident in the case of opioids, however, are seldom documented or explored in the literature on conflict of interests. We are unaware of any study that has endeavored to identify and characterize the full extent of medical product industry ties across the healthcare ecosystem, which involves individuals who and organizations that deliver healthcare, as well as politicians, regulators, supply chain entities, and others who shape the practice of medicine indirectly. The entire spectrum of direct ties, and subsequent indirect pathways for potential influence, could result in cumulative effects on patient care and public trust and are thus important to systematically document and assess.
We therefore developed an evidence based map to encompass the complex network of ties between the pharmaceutical, medical device, and biotechnology industries and healthcare ecosystem. To identify all known pathways that could enable companies to ultimately influence patient care, we systematically explored the full range of direct industry ties, both financial and non-financial, across the ecosystem, as well as indirect ties to and from other parties and activities within the healthcare ecosystem. We also cataloged the presence of conflict of interests oversight along these routes, as well as the extent to which industry ties are transparent to regulators, the public, and other key audiences. Our results provide a system level view of the medical product industry’s potential for influence across the healthcare ecosystem, ultimately culminating at patient care.
Methods
Our methods were twofold. First, we used targeted literature searches and expert input to draft a map depicting the ties between the pharmaceutical, medical device, and biotechnology industries and the key healthcare related activities and parties that shape utilization (ie, prescribing and use of medical devices and biotechnology products). Then we conducted a systematic scoping review to verify and refine the map and to catalog and characterize all documented industry ties across the healthcare ecosystem.
Mapping
We began by reviewing publications known to the research team (in particular, the Institute of Medicine’s extensive 2009 report1) and cataloged all identified parties (individuals and organizations involved in healthcare, such as hospitals, prescribers, public health agencies), activities (domains of clinical inquiry, judgment, and decision making, such as research, clinical care, guideline development), and linkages among them. Using terms such as “pharmaceutical industry”, “device industry”, and “conflict of interest”, and the “similar articles” function, we then conducted a targeted search of the medical and scientific literatures (through PubMed) to document industry ties to these parties and activities, as well as any additional parties, activities, and linkages in the healthcare ecosystem. To further explore additional, poorly documented ties, we used Google to search the gray literature, business publications, and lay literature, such as newspaper and magazine articles. All investigators independently performed searches in Google until saturation was achieved—that is, no new activities, parties, or linkages being identified. We used these findings to draft a preliminary map of the healthcare ecosystem, showing the network of ties between industry and each party and activity, as well as ties among parties and activities.
Next we obtained input from an international panel of experts with broad expertise in industry ties and deep knowledge of specific parties and activities (supplementary appendix A). We selected prominent experts on industry ties to healthcare parties or domains, or both. Experts were also selected who could reflect on these problems internationally, not just in the US context. Additionally, we included experts with deep knowledge of pricing and distribution systems, as these topics seldom appear in the literature on conflict of interest. Through WebEx we conducted semistructured interviews (supplementary appendix B) with experts individually to review the map, using their feedback on an ongoing basis to further search the literature, evaluate depicted ties, identify missing ties, and refine the map accordingly. We worked iteratively, making alterations to the general approach, categorizations, and visual presentation until reaching agreement within the research team. Experts were recruited until saturation was achieved (with no further changes suggested), which occurred after eight experts had been interviewed. We also solicited additional comments and final approval from the experts by email. Finally, we worked with design experts to optimize the visual clarity of the map.
Scoping review
We conducted a systematic scoping review of medical product industry ties to verify and refine the map, cataloging and characterizing documented financial and non-financial ties across the broad healthcare ecosystem. Our methods are reported according to the preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews (PRISMA-ScR) (supplementary appendix C).18
Protocol
Scoping reviews are not eligible for registration in Prospero; nonetheless, we used Prospero’s systematic review protocol for planning and reporting purposes (supplementary appendix D).
Eligibility criteria
The scoping review included qualitative and quantitative experimental and observational studies with English language full text available. Included studies documented ties between industry and a party or activity in the healthcare ecosystem. The scoping review excluded commentaries, conference presentations, abstracts, literature reviews, letters, and editorials.
Information sources and search strategy
Using search terms derived from our initial literature review, including “drug”, “device”, “industry influence”, “commercial support”, and “conflict of interest”, we conducted a scoping review (through PubMed, Scopus, and Embase) of the medical, scientific, and gray literatures to 31 December 2019, to systematically identify all published investigations documenting these and other emergent activities, relevant parties in the healthcare ecosystem, and linkages. We also included records from our previous manual searches that focused on poorly documented potential ties.
Relevant policies for conflict of interests and publicly available data sources that appeared in our searches were collated for separate analysis. To supplement our search for the policies and transparency sources, we also gathered information from MediSpend Legislative Watch, an industry facing website that compiles summaries and links for policies for conflict of interests and transparency requirements in countries across North America, Europe, the Middle East, and Asia.19
Study selection process
All search results were imported into Covidence, an online systematic review software program. The eligibility criteria were imported as a set of codes that were used for screening. To ensure reliability, multiple reviewers (SC, MM, SZ, DK) screened all items, with differences resolved through discussion.
Data items and data collection process
For all included articles, we abstracted data on activities, parties, types of ties (financial, non-financial), year and location of study, type of publication (gray, peer reviewed), and funding source. The data abstraction form (supplementary appendix E) was piloted on random samples of 10 included studies and modified as needed using feedback from the team. Full data abstraction began after four rounds of pilot testing, once sufficient intercoder agreement had been obtained (93.48-100%); calculable κ statistics ranged from 0.63-0.95, indicating substantial to near perfect agreement. Subsequently, one of two team members (MM, SZ) abstracted each included study, with additional feedback from others (SC, DK) as needed.
Methodological quality appraisal
We did not appraise methodological quality or risk of bias of the included articles, which is consistent with guidance on the conduct of scoping reviews.
Synthesis
Microsoft Excel was used to create descriptive statistics to characterize the publications identified in our scoping review along the extracted domains. Data from our scoping results was used to refine and verify our map, identifying, characterizing, and organizing all known pathways by which companies might potentially influence patient care. We created additional maps to separately show industry’s financial and non-financial entry points to the system.
Patient and public involvement
We did not include patients or members of the public in the research, as this was beyond the study’s scope. A patient representative reviewed the manuscript after submission.
Results
Mapping: Industry and the healthcare ecosystem
Figure 1 depicts the healthcare ecosystem, mapping the complex network of ties associated with the pharmaceutical, medical device, and biotechnology industries across the key activities and parties in the healthcare ecosystem. Beyond its direct ties to all parties and some activities, the medical product industry has numerous indirect ties across the healthcare ecosystem. Similarly, non-financial ties might reinforce or extend companies’ financial ones (fig 2 and fig 3).
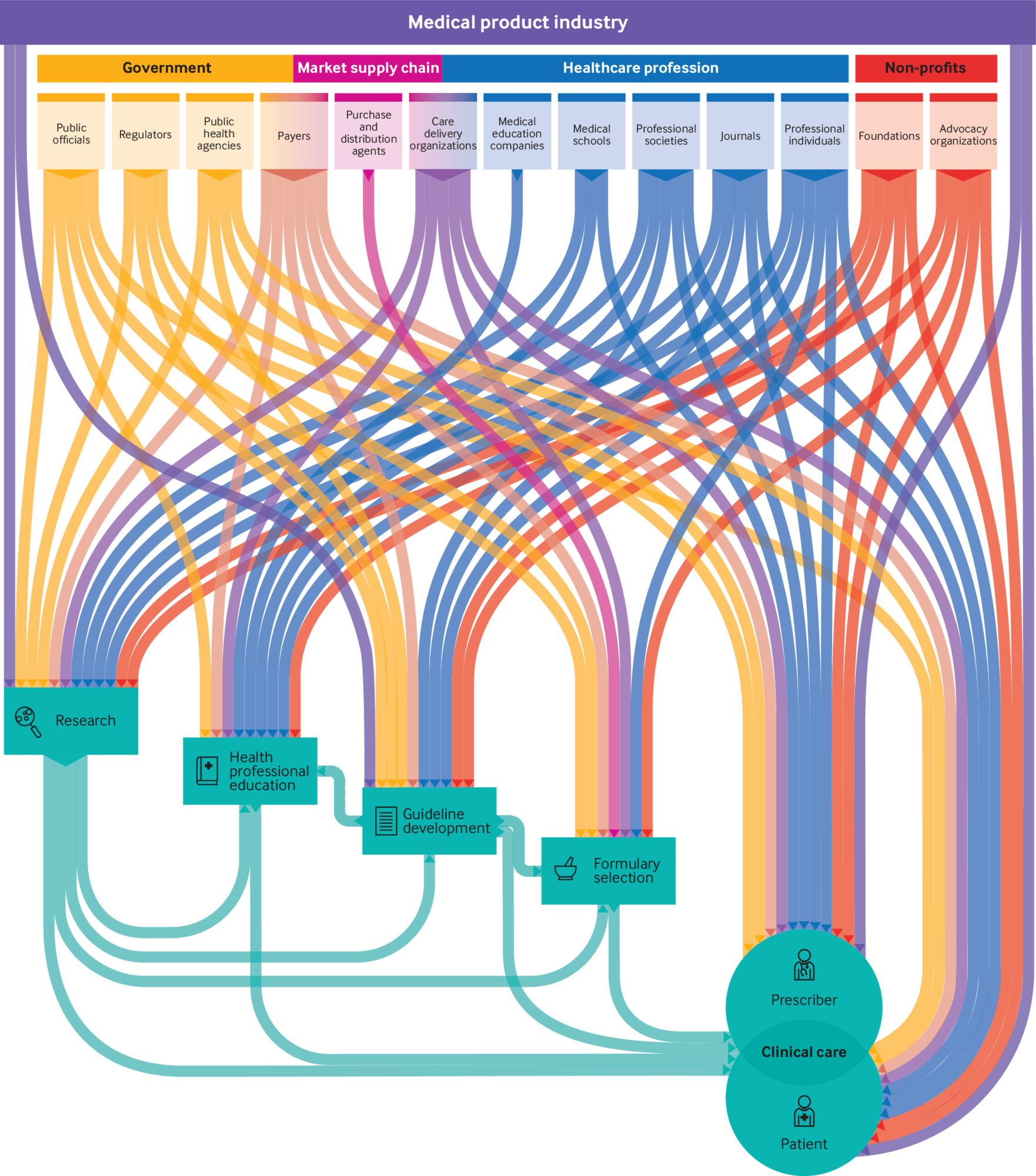
Ties between the medical product industry and healthcare ecosystem

Pathways of financial ties between the medical product industry and healthcare ecosystem

Pathways of non-financial ties between the medical product industry and healthcare ecosystem
Relevant parties in the system operate in diverse sectors of public and private life and include non-profit entities (eg, foundations, advocacy groups), the healthcare profession (eg, journals, medical schools, individual professionals), the market supply chain (eg, payers, purchasing and distribution agents), and government (eg, public officials, regulators). The medical product industry also has direct ties to patients and prescribers (box 1 and supplementary appendix F). Notably, the prescriber category is distinct from the individual professionals category, although some clinicians might belong to both categories: Prescriber denotes clinicians in a patient care role (eg, physicians, nurses, physician assistants, advanced nursing professionals) who directly determine utilization of pharmaceuticals, medical devices, and biotechnology products, whereas individual professionals more broadly includes clinicians, researchers, and other healthcare professionals and experts engaged in research, guideline development, formulary selection, health professional education, and other extraclinical activities.
Definitions of terms used in the healthcare ecosystem
Medical product industry
Pharmaceutical, medical device, and biotechnology companies that develop and manufacture medical products used in patient care1
Parties
Public officials—elected or appointed individuals in government positions20
Regulators—government bodies that regulate healthcare delivery or payments21
Public health agencies—government agencies that are involved in healthcare but do not directly deliver or regulate healthcare22
Payers—private and public health insurers23
Purchasing and distribution agents—organizations that mediate pharmaceutical pricing, payment, and distribution (eg, pharmacy benefit managers, group purchasing organizations, wholesalers)23
Care delivery organizations—facilities in which clinical care occurs, including hospitals, medical centers, clinics, private practices
Medical education companies—independent privately held businesses, usually for profit entities, that provide education to healthcare professionals24
Medical schools—institutions that award degrees for doctor of medicine or doctor of osteopathic medicine and support academic activities25
Professional societies—membership organizations consisting, and serving the interests, of healthcare professionals of the same type (eg, nurse practitioners) or from the same specialty (eg, family practitioners); activities might include education, development of guidelines and ethical codes, lobbying and advocacy, and publishing26
Journals—publications that report clinical and scientific information to physicians and other healthcare professionals27
Individual professionals—clinicians, researchers, journal editors, healthcare executives, and other experts engaged in research, guideline development, formulary selection, clinical education, or other professional activities outside of clinical care
Foundations—entities that support charitable activities by making grants to unrelated organizations or institutions or to individuals for scientific, educational, cultural, religious, or other charitable purposes28
Advocacy organizations—entities that provide patient focused or caregiver focused support, advocacy, and education, often focused on a disease or set of diseases11
Prescribers—clinicians engaged in patient care activities, including prescribing and use of medical devices and biotech products (eg, physicians, nurse practitioners, physician assistants)
Activities
Research—rigorous investigation into biology, human disease, or healthcare delivery, the results of which guide best healthcare practices29
Health professional education—Knowledge or skill acquisition related to healthcare that occurs away from patients as a free standing activity, with undergraduate, graduate, and continuing (postgraduate) components
Guideline development—systematically developed statements to assist practitioner and patient decisions about appropriate healthcare for specific clinical circumstances30
Formulary selection—the development of ranked or tiered lists of prescription drugs that are covered by a health plan or stocked by a healthcare facility; tiers typically carry different levels of cost sharing (eg, copayments or coinsurance levels)2331
Clinical care—Clinical interaction between patient and healthcare professional
Ties
Financial—economic assets or monetary payments, including but not limited to consulting fees, research funds, salary, stocks, patents, licenses, gifts, meals, travel funds, educational funds, and materials and equipment for research, education, and clinical care
Non-financial—other assets, including but not limited to information (eg, advertising, literature, reprints, and textbooks, and educational and training sessions), authorship, and data
Many medical product industry ties to these parties are financial, involving money or items of financial value, as when companies negotiate prices with supply chain agents; purchase reprints from journals; make contributions to public officials for campaigns; provide consultancy, speaking, or key opinion leader payments to healthcare professionals; or financially support government agencies, healthcare organizations, and non-profit entities through donations, grants, or fees. Other ties are non-financial, as in companies’ direct-to-consumer advertising to patients, advertising and detailing of prescribers, unpaid professional consultancy work, or the offer of data, authorship, and other professional opportunities to clinicians and researchers. All party types have financial ties to medical product companies. Only payers and distribution agents lack additional, non-financial ties (table 1, supplementary appendix E).
Examples of parties’ and activities’ direct financial and non-financial ties to the medical product industry
The healthcare ecosystem also includes five activities of clinical inquiry, judgment, and decision making at risk of commercial bias (box 1 and table 1). The medical product industry directly participates in two such activities—research and guideline development. Again, ties might be financial or non-financial, or both. For example, companies might directly fund research or guideline development and might directly provide data, content, or other non-financial assets in support of these activities.
The medical product industry also has numerous, indirect connections to three additional activities—formulary selection, medical education, and clinical care. We found no documentation to support that companies directly participate in these activities. However, they maintain extensive ties with parties who participate in these activities. For example, individuals and organizations with medical product industry ties often participate in formulary decision making, educational activities, or patient care. Similarly, linkages among activities offer companies indirect ties across the healthcare ecosystem—for example, research informs guideline development, formulary selection, and health professional education.12 The clinical care activity is unique; representing the intersection between patients and prescribers, it is shaped by all other activities and is the ultimate target of industry interest.15859
Scoping review
The literature search resulted in 2457 citations (fig 4), after elimination of duplicates. On screening of the titles or abstracts and assessing full text for eligibility, we included 538 articles for data abstraction and synthesis (table 2). The articles were published between 1980 and 2019, with half appearing after 2012. The publications spanned 37 countries, with 348 (65%) based in the United States and 190 (35%) in other geographical regions. Most of the articles (451, 84%) were peer reviewed research studies. Overall, 498 (93%) examined pharmaceutical companies, 162 (30%) studied the medical device and biotechnology industries, and 22 (4%) included all three. Notably, nearly all articles in our analysis documented financial transactions (501 (93%)), with non-financial ties appearing less often (158 (29%)).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Characteristics of 538 studies included in scoping review
The most frequently identified parties were within the healthcare profession. Individual professionals were described in 422 (78%) of the studies, prescribers in 65 (12%), medical schools in 34 (6%), and professional societies in 31 (6%). All other parties appeared in fewer than 5% of the included studies (table 2). The medical product industry’s party ties first appeared in the literature in 1980; however, our scoping review found recent citations (2018 or later) for ties to all parties except payers and medical education companies (the most recent documentation dated from 2010 and 2008, respectively).
In total, 303 (56%) of the publications documented medical product industry ties to research, with clinical care and health professional education appearing somewhat less often: 156 (29%) and 145 (27%), respectively. Ties to guideline development and formulary selection appeared in 33 (6%) and eight (1%) publications, respectively (table 2). Although these activity ties appeared in the literature as early as 1980, our scoping review also identified citations dating from 2018 or later for all activities.
Oversight and transparency
For the medical product industry’s direct ties to parties and activities, table 3 documents the presence or absence of conflict of interests oversight and public data, as uncovered by our scoping review or documented on MediSpend Legislative Watch.19 Policies for medical product industry ties are widespread among healthcare professionals and organizations, with numerous national and international bodies promulgating standards for managing such exchanges. Few, however, substantively deal with non-financial ties. Government parties are subject to varying federal, state, and local policies. Medical product industry communications to patients are federally regulated in the US and New Zealand and more tightly restricted elsewhere, but no established guidelines or policies seem to deal with companies’ financial incentives to patients (eg, copay coupons). Similarly, we found no conflict of interests oversight for medical product industry exchanges with non-profit organizations or supply chain agents.
Medical product industry interactions: Sources of transparency and conflict of interests oversight, by activity and party
Public databases are far from universal, and the ones we identified exclusively deal with financial transactions (table 3). For example, in the US, Open Payments makes transparent most but not all payments from the medical product industry to teaching hospitals and some prescribers (physicians and dentists, with data collection expanding in 2021 to include physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, and anesthesiological assistants), and Open Secrets and FollowTheMoney track companies’ contributions to state and federal candidates and officials for political campaigns. In Europe, the United Kingdom, Australia, and elsewhere, public reporting systems provide varying degrees of transparency into medical product industry payments to diverse prescribers and individual professionals (in some cases, including physician assistants, nurse practitioners, and others), care delivery organizations, health professional schools, professional societies, foundations, and advocacy organizations. We found no transparency sources for medical product industry ties to regulators, public health agencies, payers, purchasing and distribution agents, or journals.
Discussion
We conducted an extensive scoping review and interviewed experts to document an extensive network of medical product industry ties to activities and parties in the healthcare ecosystem. The pharmaceutical and medical device and biotechnology industries have established numerous ties with non-profit entities, the healthcare profession, the market supply chain, and government. Beyond clinical care, critical activities in the network include research, health professional education, guideline development, and formulary selection.
We found that conflict of interests oversight exists for some financial and a few non-financial ties between the medical product industry and other parties in the healthcare ecosystem, potentially leaving many interactions unregulated. Moreover, public data sources seldom describe or quantify these ties. This observed lack of conflict of interests oversight and transparency offers ample opportunities for medical product industry ties to potentially influence diverse clinical activities, and ultimately patient care, without the public’s knowledge. Efforts by all parties are urgently needed to deal with these gaps to protect patient care from commercial bias and to preserve public trust.
Implications
Our mapping illustrates the ways in which medical product industry influence could flow down through a complex network to reach clinical care and impact patients. Companies maintain direct ties to all parties and some activities; these direct ties then potentially extend through interrelationships among parties and activities. Industry influence might accumulate or amplify as it travels through multiple pathways to reach clinical care in ways that could be completely opaque to both clinicians and patients, yet indirect ties and the cumulative effects of those ties are seldom, if ever, examined in the literature. The medical product industry’s direct financial ties to clinicians are known to influence prescribing and other activities in which the industry participates.12798990 Our mapping illustrates how evaluating individual industry ties might underestimate the routes and magnitude of potential influence.
The findings from our scoping review illustrate the breadth of medical product industry ties to the healthcare ecosystem, with studies from 37 countries spanning six continents—documenting the great scope and diversity of industry targets across the globe. At the same time, our findings highlight the outsized focus in the literature on the healthcare profession, especially on individual professionals and prescribers. This emphasis could result from the relative availability of these data through Open Payments and other public sources. By compiling and mapping the full network of the medical product industry’s reach across the healthcare ecosystem, we depict the ways in which potential influence moves well beyond the spheres of individual professionals and prescribers.
Recent examples illustrate the power and implications of the complex ties we expose. Appendix G details how opioid manufacturers provided funding and other assets to prescribers, patients, public officials, advocacy organizations, and other healthcare parties, who, in turn, pressured regulators and public health agencies to quash or undermine opioid related guidelines and regulations.4749 Moreover, we found no evidence that the medical product industry’s activities around opioids differed from routine company practices. Analyses of past cases of consumer harm related to medical product industry promotion, as with the drug Vioxx (rofecoxib; Merk)9192 and the weight loss drug fenfluramine-phenteramine (American Home Products),93 have shown a similar, multipronged strategy of outreach to numerous parties, culminating in severe patient harm. Many additional examples of harm from industry promoted products are likely to have been unrecognized or unattributed to medical product companies’ activities. Such harms remain unexplored, but many might have led to physical harms as well as social, psychological, and other negative effects on patients.94 Moreover, medical product industry influence could undermine healthcare equity and sustainability by driving up costs for individual patients and the healthcare system overall.9596979899 In the context of eroding patient trust in the healthcare system, elucidating mechanisms of undue influence is critical.100 Our analysis and resulting map will facilitate better understanding of these pathways of potential influence and might enable regulators and the healthcare community to better protect patients and ensure public trust.
Limitations of this study
This study has several limitations. First, our findings are limited to medical product industry ties known by our experts or documented in the academic, gray, and lay literatures. Additional ties might yet exist, although our strategy of systematic, duplicative searching and feedback from an international panel of experts is unlikely to have missed common or important ties. Second, we cannot quantify the magnitude of medical product industry influence along pathways in our map. Third, our study documents not actual bias but the pathways for potential influence across the system. Fourth, our scoping review included older evidence that might not reflect current practices; however, half of included papers were published after 2012, and medical product industry ties to nearly all parties and activities have even more recent documentation, so the body of evidence likely remains relevant. Finally, our review might have missed some policies for conflict of interests and publicly available data sources because we focused on ties, although we did supplement our search by consulting MediSpend Legislative Watch.19 More research is needed to explore these issues.
Conclusions
The medical product industry maintains an extensive network of financial and non-financial ties with all major healthcare parties and activities. This network seems to be mostly unregulated and opaque. Although the medical product industry is a critical partner in advancing healthcare, companies must also work to maximize profits as part of fiduciary responsibility to shareholders or owners and thus use all available means to promote products. With absent effective conflict of interests oversight, such promotion might ultimately threaten the integrity, equity, and sustainability of healthcare systems and impact individual patients. It is therefore up to other key parties, including the healthcare profession and policy makers, to effectively manage commercial influence, protect patient safety, and ensure public trust.
What is already known on this topic
Most studies of conflict of interests related to pharmaceutical, medical device, and biotechnology companies have focused on one party (eg, prescribers, organizations) or activity (eg, research, education, clinical care) in the healthcare ecosystem
The range and interrelationships of company ties across the healthcare ecosystem are incompletely described
What this study adds
The medical product industry maintains numerous ties with all major healthcare parties and activities
This extensive network of ties is often unregulated and non-transparent
Enhanced oversight and transparency are needed to shield patient care from commercial influence and to preserve public trust in healthcare
Ethics statements
Ethical approval
The institutional review board at Memorial Sloan Kettering Cancer Center determined the study as exempt, category 4 research.
Data availability statement
Data are available upon reasonable request to the corresponding author.
Acknowledgments
We thank Andrew Briggs, Anna Kaltenboeck, Aaron Kesselheim, Joel Lexchin, Barbara Mintzes, Aaron Mitchell, Daisy Smith, and Nancy Yu for serving as experts in the study; Beth Shirrell and Renee Walker of Gold Collective for design assistance; and Jennifer Hsu and Joseph Kanik for research support.
Footnotes
Contributors: DK, SC, BB, and PB interviewed experts. DK, SC, MM, and SZ did the scoping review. MM, SZ, SC, and DK analyzed the data. BB, SZ, SC, and DK produced the figures. SC and DK drafted the manuscript. SC, DK, MM, SZ, and PB revised the manuscript. SC and DK are the guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: SC, PBB, and DK were supported in part by Arnold Ventures and from a grant to Memorial Sloan Kettering Cancer Center from the National Cancer Institute (P30 CA008748) for this work. The funders had no role in the design, conduct, reporting, or dissemination plans for this study.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from Arnold Ventures and the Memorial Sloan Kettering Cancer Center. DK’s spouse has equity interest and serves on the scientific advisory boards of Vedanta Biosciences and Opentrons and provides consulting for Fimbrion. PBB has received personal fees from Mercer, Foundation Medicine, Grail, Morgan Stanley, NYS Rheumatology Society, Cello Health, Anthem, Magellan Health, EQRx, Meyer Cancer Center of Weill Cornell Medicine, and National Pharmaceutical Council; personal fees and non-financial support from United Rheumatology, Oppenheimer, Oncology Analytics, Kaiser Permanente Institute for Health Policy, Congressional Budget Office, America’s Health Insurance Plans, and Geisinger; and grants from Kaiser Permanente and Arnold Ventures outside the submitted work. We, the authors, would like to disclose a potential intellectual bias, in that our concern about undue medical product industry influence motivated us to conduct this study. In view of this, to ensure accurate, reproducible findings, we methodically solicited input on relevant parties, domains, and connections from an international panel of experts on conflict of interests. We then scoured the published literature for all available documentation of these parties, domains, and connections, following rigorous standards for conducting scoping reviews.
The lead authors (SC and DK) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned have been explained.
Dissemination to participants and related patient and public communities: We plan to disseminate our findings widely and have developed an interactive tool on our research group’s website (www.drugpricinglab.org/tools/octopus/) to enable patients, the public, journalists, policy makers, researchers, and others to explore the flow of medical product industry assets through the healthcare ecosystem.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.