





Abstract
Balloon pulmonary angioplasty (BPA) is an emerging treatment for patients with inoperable chronic thromboembolic pulmonary hypertension (CTEPH).
We report on a prospective series of 56 consecutive patients who underwent 266 BPA interventions (median, five per patient) at two German institutions. All patients underwent a comprehensive diagnostic work-up including right heart catheterisation at baseline and 24 weeks after their last intervention.
BPA resulted in improvements in WHO functional class, 6 min walk distance (mean change, +33 m), right ventricular function and haemodynamics, including a decline in mean pulmonary artery pressure by 18% and in pulmonary vascular resistance by 26%. Procedure-related adverse events occurred in 9.4% of the interventions. The most common complications were related to pulmonary vascular injury and consecutive pulmonary bleeding. Most of these events were asymptomatic and self-limiting, but one patient died from pulmonary bleeding, resulting in a mortality rate of 1.8%.
BPA resulted in haemodynamic and clinical improvements but was also associated with a considerable number of complications, including one fatal pulmonary bleeding. As the effects of BPA on survival are unknown, randomised controlled outcome trials comparing BPA with approved medical therapies in patients with inoperable CTEPH are required to allow for appropriate risk–benefit assessments.
Abstract
BPA improves haemodynamics and exercise capacity in patients with inoperable CTEPH but complications are not uncommon http://ow.ly/mMYY30b1rch
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a life-threatening disease caused by persistent obstruction of pulmonary arteries as a result of residual pulmonary emboli and consecutive small-vessel pulmonary vascular remodelling [1, 2]. Surgical pulmonary endarterectomy (PEA) is the standard treatment of CTEPH and potentially curative [3, 4]. However, about one-third of the patients are not operable, mostly because of peripheral location of pulmonary vascular obstructions or because of comorbidities [5]. In addition, up to 50% of patients undergoing pulmonary endarterectomy have residual pulmonary hypertension (PH), which is usually mild, but occasionally moderate-to-severe, requiring additional treatment [6, 7]. Drug therapy with riociguat, a soluble guanylate cyclase stimulator, improves haemodynamics and exercise capacity in patients with inoperable or residual CTEPH, but it is not curative [8–10].
An evolving interventional treatment option for patients with inoperable CTEPH is balloon pulmonary angioplasty (BPA). After a first case report in 1988 [11], a series of 18 patients was presented by Feinstein et al. in 2001 [12], followed by two additional cases from Germany in 2003 [13]. BPA initially did not get widespread attention as it was associated with serious and potentially fatal complications, most notably reperfusion oedema and pulmonary bleeding. Over the past couple of years, however, BPA has re-emerged after several centres, mainly from Japan, have optimised the interventional approach using modern imaging technology, a careful staged approach and undersizing of the balloons to minimise injury to the pulmonary vessels [14–16]. The initial peri-procedural mortality was 3–10% [16–18] but this figure has dropped to 0–1.5% in more recent reports [14, 15, 19–22]. At the same time, impressive haemodynamic and clinical improvements closely resembling those seen in pulmonary endarterectomy with normalisation or near-normalisation of pulmonary haemodynamics in up to 50% have been reported [14, 19]. In addition, hybrid procedures consisting of pulmonary endarterectomy surgery and intraoperative BPA have been described in highly selected cases with operable findings in one lung and inoperable findings in the contralateral lung [23].
Despite being a promising therapy for patients with CTEPH, BPA is not yet considered an established procedure [24–26]. So far, there are no long-term, multicentre data on the safety and efficacy of BPA and it is unclear if BPA improves survival in patients with inoperable CTEPH. In addition, BPA was initially developed in countries where pulmonary endarterectomy was not widely used. Hence, several patients who underwent BPA may have been considered operable in other countries. Only recently, BPA has been adopted by European and American centres with established surgical programmes. In these centres, BPA is offered exclusively to patients who are considered inoperable or who suffer from symptomatic residual PH after surgery. It is unclear if the results of BPA in centres that strictly restrict BPA to inoperable patients are comparable with the results of BPA in centres that offer this interventional approach to a broader population of patients with CTEPH.
In Germany, BPA was introduced in 2013 by two centres with established surgical programmes for CTEPH (Kerckhoff Clinic Bad Nauheim and Hannover Medical School). These two centres cooperate closely as members of the German Centre for Lung Research. Both centres hold regular multidisciplinary conferences to determine individual treatment strategies for patients with CTEPH and offer BPA only to patients who are deemed technically inoperable or at high surgical risk, respectively. The two centres utilise different imaging technologies and technical approaches but similar standardised follow-up programmes for patients undergoing BPA to allow comparative analysis. Here, we present the results of the first 56 consecutive patients who underwent BPA in these two centres.
Methods
Patient selection
The two participating centres hold weekly conferences of a multidisciplinary team consisting of experienced PEA surgeons, interventional radiologists, cardiologists and/or pneumologists, and anaesthesiologists, if required. Inoperable patients were selected for BPA based on a comprehensive assessment of haemodynamics, comorbidities and imaging findings.
Per protocol, PH-targeted medication was introduced at least 12 weeks prior to BPA and remained unchanged during the study.
All patients were informed verbally and in writing about the innovative nature of the procedure including potential risks and benefits. This prospective study was approved by the ethics committees of both institutions and all patients provided written informed consent.
Clinical assessment
All patients underwent structured pre-specified assessment at baseline, i.e. prior to the first BPA, before each consecutive intervention and 24 weeks after the last BPA. Assessment at baseline and at week 24 after intervention included the WHO functional class (FC), the 6 min walk test (6MWT), the Borg dyspnoea index obtained directly after the 6MWT, pulmonary function testing including the lung diffusion capacity for carbon monoxide (DLCO), serum levels of creatinine (with calculation of the estimated creatinine clearance) and the N-terminal fragment of pro-brain natriuretic peptide (NT-proBNP), echocardiography (including right ventricular end diastolic diameter, right ventricular free wall diameter, tricuspid annular plane systolic excursion, right atrial dilation, defined as right atrial diameter >43 mm in the four-chamber view) and right heart catheterisation to determine right atrial pressure, pulmonary arterial pressures, pulmonary arterial wedge pressure (PAWP), cardiac output (CO), cardiac index (CI), pulmonary vascular resistance (PVR) and mixed-venous oxygen saturation (SvO2). Assessment between the BPAs consisted of WHO FC, 6MWT and laboratory studies as described above.
Balloon pulmonary angioplasty
Both centres used a staged approach targeting a limited number of segmental or subsegmental pulmonary arteries during each intervention with intervals of 4–6 weeks between each session. All procedures were performed under local anaesthesia.
Bad Nauheim
In Bad Nauheim, all patients received direct-acting oral anticoagulants (DOACs) for the intervention period. One day prior to BPA, DOACs were replaced with low molecular weight heparin (LMWH). LMWH was not administered on the day of BPA. During the procedure, unfractionated heparin was used intravenously at 100 IU·kg−1 to maintain an activated clotting time >250 s.
BPA was performed in a series of staged procedures over a 6-month period using a femoral or jugular access. A 6F sheath (Johnson & Johnson Vista Brite Tip, Milpitas, CA, USA) was placed in the pulmonary artery using fluoroscopy (Siemens Axiom artis zee, Siemens, Erlangen, Germany), and a 6F guiding catheter (Medtronic multi-purpose, Judkins right 4, Medtronic, Dublin, Ireland) was inserted in the pulmonary artery to intubate the segmental arteries. The guide wire (Runthrough NS-PTCA Guide Wire, Terumo Europe, Leuven, Belgium) was placed into the target subsegmental arteries, whose diameters had been determined by fluoroscopy. Subsequently, the target subsegmental branches were dilated by multiple balloon inflations using semi-compliant balloons (Emerge 2.0/20 mm and 4.0/20 mm, Boston Scientific, Marlborough, MA, USA). To avoid pulmonary arterial rupture, slightly undersized balloons were used in all cases. A final pulmonary angiography documented the post-procedural morphologic result.
Hannover
In Hannover, BPA procedures were conducted as described previously [27]. All patients received anticoagulation with rivaroxaban, which was paused for the intervention day (without LMWH bridging). During the procedure, patients received 5000–10 000 IU of unfractionated heparin intra-arterially. A 6F sheath (Destination – Peripheral guiding sheath, Terumo Europe, Leuven, Belgium) was placed in the main pulmonary artery of interest and a selective C-Arm CT (CACT) was acquired using a 5F pigtail catheter (Optitorque, Terumo Europe) as described elsewhere [27, 28]. The target lesions were localised by selective digital subtraction angiography (DSA) and CACT. Based on these images, centre-lines indicating the course of the pulmonary arteries were drawn, BPA positions were identified and marked by coloured lines in the CACT dataset [27]. Both images could be superimposed on the live fluoroscopic image during intervention for individual navigation. Subsequently, a 6F guiding catheter (MACH 1, Boston Scientific, Marlborough, MA, USA) was advanced into the targeted pulmonary artery segment and a hydrophilic 0.014-inch guide-wire (V-14, Boston Scientific) was used to cross the target lesions. Based on the measured vessel diameter in CACT, appropriate rapid exchange balloon catheters (1.2–4 mm, Emerge, Boston Scientific) were selected. The balloons were advanced through the pulmonary lesion and inflated for 15–60 s by hand using an inflation device. BPA results were documented by selective pulmonary angiograms.
Statistical analysis
The IBM SPSS Statistics 24.0 (IBM Corp, Armonk, NY, USA) and STATA 13.0 (State Corp LP, College Station, TX, USA) statistical software were used to analyse the data. Categorical variables are shown as numbers (n) and percentages (%). Continuous variables are shown as mean±sd, unless indicated otherwise. For comparisons, Fisher's exact test, Chi-squared test, Mann–Whitney U test, McNemar's test or two-sided paired t-test were used as appropriate. All reported p-values are two-sided unless indicated otherwise; p-values <0.05 were considered statistically significant.
Results
Baseline characteristics, effects of BPA and procedures
Between August 2013 and January 2016, 56 consecutive patients were enrolled into this study: 31 in Hannover and 25 in Bad Nauheim. Only patients undergoing hybrid procedures, i.e. PEA surgery and BPA at the same time [23], were excluded. The demographics and baseline characteristics of these patients are depicted in tables 1 and 2. Follow-up ended in July 2016. The median duration between CTEPH diagnosis and first BPA was 14 months; in 34% of the patients this interval exceeded 2 years. Most patients received PH-targeted therapies, which were introduced at least 3 months prior to baseline assessment and kept unchanged during the study.
Characteristics of patients at time of inclusion
Changes from baseline to week 24
A total of 266 interventions were performed: 155 in Hannover and 111 in Bad Nauheim. In both centres, the median number of interventions per patient was five (range, 3–8). The median number of vessels targeted per intervention was two (range, 1–4). The median duration from first BPA to the 24-week follow-up assessment was 13.8 months.
Treatment response
The effects of BPA on haemodynamics, right ventricular (RV) function, serum NT-proBNP and exercise capacity are presented in table 2. WHO FC improved in 33 (59%) patients and remained unchanged in 22 (41%) patients; it did not deteriorate in any patients. The 6-min walk distance improved by an average of 33 m (about 9% from baseline) accompanied by a reduction in the Borg dyspnoea index. Haemodynamic assessment showed improvements in right atrial pressure, mean pulmonary artery pressure (PAPm) and PVR, while CO, CI and SvO2 remained unchanged. NT-proBNP improved and so did several echocardiographic measurements of RV function including right atrial diameter, RV diameter and tricuspid annular plane systolic excursion. Arterial oxygen tension (increased while DLCO remained unchanged, as did serum creatinine and creatinine clearance.
Supplementary table S1 shows the effects of BPA on haemodynamics, RV function, serum NT-proBNP and exercise capacity in the two centres.
Complications
A total of 25 procedure-related complications (Hannover, n=9; Bad Nauheim, n=16) occurred during the 266 interventions (9.4% of all interventions, 32% of all patients; figure 1 and table 3). Most of these adverse events were related to pulmonary vascular injury by wire perforation resulting in parenchymal bleeding with or without haemoptysis, the majority of which were mild and did not require intervention. There was, however, one episode of fatal pulmonary bleeding. In that patient, wire perforation of a subsegmental right lower lobe artery occurred during the intervention. The patient was initially asymptomatic and had no haemoptysis. Chest fluoroscopy showed mild parenchymal bleeding which appeared to have stopped spontaneously without further therapeutic measures. The patient was discharged from the hospital after 1 week in apparently good health but was admitted 14 days after the intervention to another hospital with shock, respiratory distress and a large right-sided haemothorax. The patient could not be stabilised and died from haemorrhagic shock.
{kind=link}
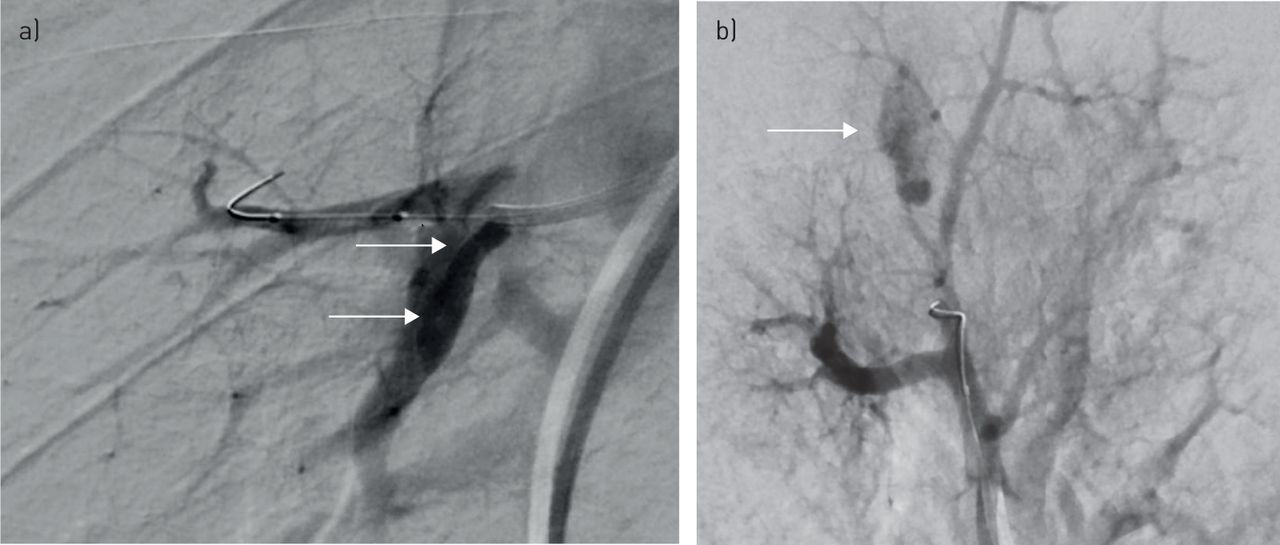
a) Digital subtraction angiography of the middle lobe arteries in a 63-year-old man with inoperable chronic thromboembolic pulmonary hypertension (CTEPH) showing a pulmonary artery dissection (arrows) after manipulation with the guiding catheter. b) Digital subtraction angiography of the right upper lobe arteries in a 72-year-old woman with inoperable CTEPH showing pulmonary haemorrhage (arrow) after guide wire perforation.
Complications related to balloon pulmonary angioplasty
Discussion
The present study supports the notion that BPA is potentially an effective interventional treatment for patients with inoperable CTEPH. We saw improvements in pulmonary haemodynamics, RV function, serum NT-proBNP, WHO functional class and 6 min walk distance in most of our patients, but this did not come without risks. In the present series of 266 interventions in 56 patients, adverse events occurred in 9.4% of the interventions; 32% of the patients had at least one procedure-related event. Reperfusion oedema, which was the predominant adverse event in previous series [12, 15–17], was rare, occurring only in two patients. By far the most common complication in our series was pulmonary bleeding because of pulmonary vascular injury. In the majority of cases, bleeding was mild, asymptomatic and required no intervention. One patient, however, died from pulmonary bleeding, resulting in a mortality rate of 1.8%.
The average haemodynamic improvement observed with BPA in our study was moderate with an 18% drop in PAPm (from 40 mmHg to 33 mmHg) and a 26% decrease in PVR (from 591 to 440 dyn·s·cm−5). These haemodynamic improvements were less pronounced than in previous publications from Japanese centres, which reported reductions in PAPm and PVR between 31–49% and 45–69%, respectively [14, 15, 18–20, 22]. There are several possible explanations for these differences. 1) One might argue that Japanese centres are more experienced in BPA than German centres; however, both German centres developed BPA in close collaboration with Japanese centres and used basically the same interventional approach; in addition the overall number of 266 interventions in our series makes lack of experience an unlikely explanation; finally, the number of patients and interventions reported from Japanese centres was in the same range as in our series [14, 16]. 2) We studied a prospective cohort of consecutive patients treated in two centres whereas previous reports were based on single-centre series, so that the possibility of selective reporting cannot be excluded. 3) PEA surgery is well established in Germany but it is used less frequently in Japan; some of the patients who underwent BPA in Japan would have been deemed operable in Germany, but we selected for BPA only patients with inoperable disease or residual PH after surgery; hence, patient populations were not comparable. 4) The majority of patients in our series had a relatively long interval between CTEPH diagnosis and first BPA (median 14 months; 34% of the patients >2 years). It is possible that some of these patients had developed peripheral pulmonary vasculopathy, which would mitigate the haemodynamic effects of upstream interventions such as BPA.
The haemodynamic effects of BPA observed in our study were inferior to the effects of PEA surgery, which decreases PAPm by approximately 40% and PVR by approximately 60% [3, 6], but are similar to the effects of riociguat, which decreases PAPm by approximately 11% and PVR by approximately 31% in patients with inoperable CTEPH [8].
The profile of the haemodynamic changes observed with BPA, however, was different from the haemodynamic changes observed with medical therapy as we saw improvements in PAPm and PVR with very small changes in cardiac output. Medical therapy, in contrast, tends to improve mostly cardiac output, but the effects on PAPm are usually modest [8, 29]. One possible reason for this observation may have been that most patients in our study had normal or near normal cardiac output at baseline, perhaps because almost all of them were already pre-treated with PH medications. The baseline haemodynamics of our patients were similar to the on-treatment haemodynamics reported with riociguat in the CHEST-1 study [8]. In addition, it is possible that the increase in cardiac output observed with most medical therapies is partly mediated by systemic vasodilation, an effect that would be absent with BPA. This hypothesis is supported by the haemodynamic effects of inhaled nitric oxide, a selective pulmonary vasodilator, which also lowers PAPm with little effect on cardiac output [30].
As stated above, adverse events occurred in 9.4% of the interventions and in 32% of the patients. The observed mortality rate of 1.8% (1 of 56 patients) is similar to more recent publications from Japanese centres that reported mortality rates between 0 and 1.5% [14, 15, 19, 22]. However, the rate of pulmonary vascular injury with or without pulmonary bleeding was higher in our series, possibly because we recorded all episodes of parenchymal bleeding, even if they did not require interventions. The rate of adverse events tended to be higher in Bad Nauheim than in Hannover, which might have been partly related to the fact that Bad Nauheim used conventional contrast-enhanced DSA to guide the interventional procedures whereas DSA and CACT imaging were used in Hannover. CACT provides more detailed imaging of peripheral pulmonary arteries, allowing for a more reliable assessment of accessibility, vessel morphology and diameter, adequate balloon size and procedural guidance [27, 28]. In addition, LMWH bridging in patients receiving DOACs may have been associated with an increased bleeding risk in Bad Nauheim, as has been reported from other patient populations [31, 32].
Our study has several limitations. Firstly, although this was one of the largest prospective series of BPA, the number of patients was still small. Secondly, there was no control group. Thirdly, efficacy measures such as 6MWT, WHO FC and haemodynamics were not obtained by blinded study personal. Finally, long-term outcome data were not available. Despite these limitations, our data may provide a realistic perspective on the risks and benefits associated with the introduction of a BPA programme in referral centres with an established surgical programme for CTEPH.
In conclusion, our results confirm previous reports demonstrating that BPA improves haemodynamics, RV function and exercise capacity in patients with inoperable CTEPH or residual PH after PEA surgery. However, like any other interventional procedure, BPA is associated with potentially life-threatening complications. Further studies need to determine whether CACT-guided BPA is safer than DSA-guided BPA. Most importantly, as it remains unknown if BPA improves survival, our data call for a large, prospective, multicentre study comparing long-term outcomes in patients receiving medical therapy and BPA with medical therapy alone.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Table S1. Measurements at baseline and 24 weeks after the final BPA and changes from baseline in the two participating centres Supplementary_Table_S1
Disclosures
Supplementary Material
H.A. Ghofrani ERJ-02409-2016_Ghofrani
S. Guth ERJ-02409-2016_Guth
M.M. Hoeper ERJ-02409-2016_Hoeper
T. Kramm ERJ-02409-2016_Kramm
C. Liebetrau ERJ-02409-2016_Liebetrau
E. Mayer ERJ-02409-2016_Mayer
B.C. Meyer ERJ-02409-2016_Meyer_BC
K. Meyer ERJ-02409-2016_Meyer_K
K.M. Olsson ERJ-02409-2016_Olsson
C.B. Wiedenroth ERJ-02409-2016_Wiedenroth
Acknowledgements
We are indebted to Norifumi Nakanishi, Takeshi Ogo, Toru Satoh and their groups for invaluable advice and support during the implementation of our BPA programme.
Footnotes
First published online June 8, 2017; republished June 30, 2017 with amendments to the authors' affiliation details.
This article has supplementary material available from erj.ersjournals.com
Support statement: The study was funded by the German Centre of Lung Research (DZL). M.M. Hoeper was supported by the Deutsche Forschungsgemeinschaft (HO 1599/2-1).
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received December 7, 2016.
- Accepted March 11, 2017.
- Copyright ©ERS 2017
References










