Article Text

Abstract
Background The Multiple Sleep Latency Test (MSLT) remains an important diagnostic tool in the diagnosis of hypersomnias. However, a positive MSLT may be found in other sleep disorders, such as behaviourally induced inadequate sleep syndrome (BIISS). It has been demonstrated that in sleep onset rapid eye movement (SOREM) periods in BIISS, REM sleep tends to arise from stage 2 sleep (non-REM (NREM) 2), rather than stage 1 sleep (NREM1), as in narcolepsy.
Methods We performed sleep stage sequence analysis on 127 patients with nocturnal polysomnography and MSLT, including 25 with narcolepsy with cataplexy (N+C), 41 with narcolepsy without cataplexy (N−C), 21 with idiopathic hypersomnia with long sleep time (IHL), 20 with BIISS and 20 with periodic limb movement disorder (PLMD). 537 naps were recorded, containing 176 SOREM periods.
Results All SOREM periods in the IHL, BIISS and PLMD groups arose from NREM2 sleep, 75% of those in N+C arose from NREM1 and in N−C only 52% arose from NREM1. Within the N−C group, those with SOREM periods all arising from stage 1 had a shorter MSL (p=0.02).
Conclusions These results suggest that SOREM periods arising from NREM1 have high sensitivity for the diagnosis of narcolepsy and that SOREM periods from NREM1 are a marker of severity, either of sleepiness or REM instability. Sleep stage sequence analysis of SOREM periods may also aid more accurate phenotyping of the hypersomnias and in particular clarify heterogeneity among patients with narcolepsy without cataplexy.
- Sleep Disorders
Statistics from Altmetric.com
Introduction
Excessive daytime sleepiness (EDS) is defined as sleepiness occurring in situations in which an individual should be alert and awake. The prevalence of this symptom in the general population is estimated at between 0.5% and 5%.1 ,2 According to the International Classification of Sleep Disorders, second edition (ICSD2),3 EDS is an essential characteristic of narcolepsy, hypersomnia and behaviourally induced insufficient sleep syndrome (BIISS), and is also associated with a wide range of diseases, including psychiatric, neurological, pulmonary and cardiac conditions.
The gold standard in the measurement of EDS is the Multiple Sleep Latency Test (MSLT) where patients are given the opportunity to take four or five naps at 2 h intervals, under controlled conditions, and with polysomnographic monitoring. The mean sleep latency (MSL) of all naps is calculated and the presence of abnormal rapid eye movement sleep onset periods (SOREM periods), defined as rapid eye movement (REM) onset within 15 min of sleep onset, are also scored.4 The most recent ICSD has defined an MSL of <8 min as sleepiness for diagnostic purposes,3 while adult healthy control subjects have an MSL of 10–20 min.5 The MSLT is thought to measure physiological sleep tendency. It was initially developed as a tool to measure daytime sleepiness following sleep deprivation6 and subsequently became a diagnostic tool in narcolepsy and idiopathic hypersomnia (IH).7
The MSLT still remains an important diagnostic tool in the diagnosis of narcolepsy and IH. The ICSD23 states that an MSLT with an MSL of ≤8 min and two or more SOREM periods is a mandatory diagnostic criterion for narcolepsy without cataplexy (N−C), and should be performed, where possible, to confirm the diagnosis of narcolepsy with cataplexy (N+C). For IH, with or without long sleep time, a syndrome associated with non-imperative sleepiness, long unrefreshing naps, prolonged night-time sleep, difficulty reaching full wakefulness after sleep and sleep drunkenness, the diagnostic criteria include an MSL of <8 min and fewer than two SOREM periods.
Many narcoleptic patients do not have the full spectrum of diagnostic symptoms, while up to a third of them will never develop cataplexy. It is frequently argued that the presence of cataplexy is pathognomonic for N+C. However, cataplexy-like events are not infrequent in other hypersomnias or even in normal controls,8 and have been described as arising in psychogenic disorders.9 Therefore, the diagnosis of N+C on clinical grounds may not be without problems. The absence of cataplexy in N−C complicates diagnosis on clinical grounds further, as behaviourally induced inadequate sleep syndrome (BIISS)—chronic sleep deprivation resulting in EDS that resolves with prolongation of sleep time—can give rise to similar clinical findings.10 The diagnosis of BIISS can frequently be missed and requires careful investigation of sleep patterns with a sleep diary and/or actigraphy.
Despite the emphasis on the MSLT in these diagnostic criteria, the reliability of the MSLT has been questioned. In a retrospective analysis of MSLTs,11 6% of patients with sleep disordered breathing and 4% of patients with other sleep disorders met the ICSD2 MSLT definition for narcolepsy; 18% οf patients with narcolepsy who had two MLSTs did not meet ICSD112 criteria on either study, and 45% did not meet ICSD1 criteria on one or other MSLT. These results suggest that the MSLT may be falsely positive or negative, and the authors concluded that the MSLT cannot be used to exclude or confirm narcolepsy in isolation, and is of greatest value when interpreted in a clinical context.
In another study, polysomnography (PSG) and MSLTs were performed on normal subjects.13 An MSL of 8 min or less, with two or more SOREM periods, was demonstrated in 5.9% of men and in 1.5% of women, all without cataplexy, implying that either narcolepsy is grossly underdiagnosed or that the MSLT has a high false positive rate when using the ICSD2 criteria.
More recently, analysis of the MSLT in patients with N+C and BIISS demonstrated that SOREM periods occurred frequently in the naps of patients with N+C, but also in some naps of patients with BIISS.10 Analysis of sleep stage sequences in naps with SOREM periods showed a significant difference between the two groups, with REM sleep following non-REM (NREM) 1 in 71% of SOREM periods in patients with N+C, in contrast with only 15% in those patients with BIISS, where REM was entered mostly from NREM2.
The apparent utility of sleep stage sequencing in discriminating N+C from BIISS raises the possibility that this aspect of the MSLT may be helpful in the diagnosis of narcolepsy, a condition without a definitive pathophysiological marker, and to dissect out heterogeneity in the group of patients diagnosed with N−C, in whom a subset at least appear to have a shared pathophysiology with N+C, while others appear to share clinical features with IH.14 We hypothesised that narcoleptics are more likely than BIISS and other patients with hypersomnias to have SOREM periods arising from NREM1 or wake, which may aid discrimination. Furthermore, we also hypothesised that the different proportion of the sequence NREM1–REM in patients with N+C and N−C may permit more accurate phenotyping of these groups, and in particular shed light on possible heterogeneity in the N−C patient group.
Patients and methods
Patients who underwent nocturnal PSG followed by an MSLT the next morning between August 2008 and March 2012 at Guy's and St Thomas’ Sleep Disorders Centre were retrospectively ascertained. All patients had been evaluated by an experienced sleep physician prior to their sleep study and were required to complete a sleep diary prior to the study. The MSLT were performed according to standard guidelines,4 using central (C3 and C4) and occipital (O1 and O2) electrodes for the montage, with auricular reference electrodes, two electro-occulographic channels, two submental electromyographic channels and electrocardiography. Sleep stages were scored using 30 s epochs according to standard criteria of the American Academy of Sleep Medicine,15 while the scorer was blinded to the diagnosis of the patient. Four or five naps, with a 2 h interval between them, were performed for each patient. Diagnoses of N+C, N−C, IHL and BIISS were made in accordance with ICSD2 criteria, based on a clinical evaluation which included history and physical examination, supplemented by the results of the MSLT.3 In all cases, the MSLT was performed the day following a night of at least 6 h of polysomnographically defined sleep without evidence of other sleep pathology, off sleep influencing drugs for at least 15 days and preceded by a sleep log or actigraphy for the period of 2 weeks prior to the MSLT.15
A group of isolated PLMD was used as a control group in our study, with a periodic limb movement index of 40.3±18. Patients in whom another diagnosis could be made, where there remained diagnostic doubt, clinical information was incomplete or in whom the sleep study could not be conclusively interpreted due to less than 6 h of sleep during PSG or failure to stop all medication, were excluded from these diagnostic categories. Interpretation of the sleep studies were blinded to MSLT sleep stage sequence as this was only performed for the purposes of this study.
All MSLTs were analysed to determine the MSL, number of SOREM periods, nap in which SOREM period occurred and stage of sleep from which REM sleep occurred within a SOREM period.
HLA typing for DQB1*0602 status was only available for a few of the patients and consequently it was not included in the study.
Statistical analysis was performed using the SPSS statistical analysis programme (SPSS 17.0). Data are reported as mean±SD, if not otherwise indicated. Following testing for normality, the similarity of two means was compared using the Student's t test and χ2 statistics in the case of normal distribution; otherwise the Wilcoxon signed rank test was used. Comparisons between N+C, N−C, BISS, IHL and controls were made using one way ANOVA with post hoc test least significant difference or Kruskal–Wallis test, in the case of non-Gaussian distribution. Linear regression was used to model the relationship between two variables by fitting a linear equation to the observed data. We considered p<0.05 to be statistically significant.
Results
A total of 257 consecutive patients underwent PSG and MSLT over a 3.5 year period. Twenty-six patients were excluded due to lack of clinical information and 104 patients were excluded due to multiple diagnoses or diagnostic uncertainty. The remaining 127 patients were categorised into diagnostic categories of N+C, N−C, IHL, BIISS and PLMD: 25 (19.6%) patients were diagnosed with N+C, 41 (32.3%) with N−C, 21 (16.5%) with IHL, 20 (15.7%) with BIISS and 20 (15.7%) with PLMD (table 1).
Diagnostic categories and demographics
By definition, all patients in the N+C and N−C groups had MSL values of <8 min, with at least two SOREM periods, the IHL group had an MSL <8 min with less than two SOREM periods, while four BIISS patients demonstrated one or more SOREM periods and six patients with BIISS had an MSL >8 min. One patient with BIISS met both diagnostic criteria for narcolepsy on the MSLT.
The mean MSL was 2.6 (±1.6) min for N+C patients, 4 (±2.1) min for N−C patients, 5.4 (±1.8) min for IHL patients, 7.6 (±3.9) min for BIISS patients and 10.2 (±4.9) min for PLMD patients. Seven of the PLMD patients had an MSL <8 min. The MSL differentiated statistical significance between groups, except between N+C and N−C and between N−C and IHL (table 2).
Comparison of mean±SD of mean sleep latency between the groups
A total of 537 naps were recorded, of which 176 contained SOREM periods: 64 of 102 naps (62.7%) contained SOREM periods for the N+C group, 101 of 169 naps (59.7%) for the N−C group, one of 94 naps (1%) for the IHL group, six of 84 naps (7.14%) for the BIISS group and four of 84 (4.7%) for the PLMD group. The distribution of SOREM periods in the naps showed no significant difference for the N+C and N−C groups (p=0.92) using χ2 testing (table 3).
Distribution of SOREM periods in naps
Sleep stage sequencing in SOREM periods revealed that in the N+C and N−C groups, REM periods occurred from stage NREM1, NREM2 or wake. In contrast, in the IH, BIISS and PLMD groups, SOREM periods occurred only from stage NREM2. In the N+C group, SOREM periods arose more frequently from NREM1 (75%) than NREM2 (21%) (p<0.0001). This tendency of SOREM periods arising from NREM1 was not observed to the same degree in the N−C group (52% of SOREM periods arising from NREM1 and 46% arising from NREM2) (p=0.0024) (table 4).
Tendency of the groups to have SOREM periods from NREM1, NREM2 or wake
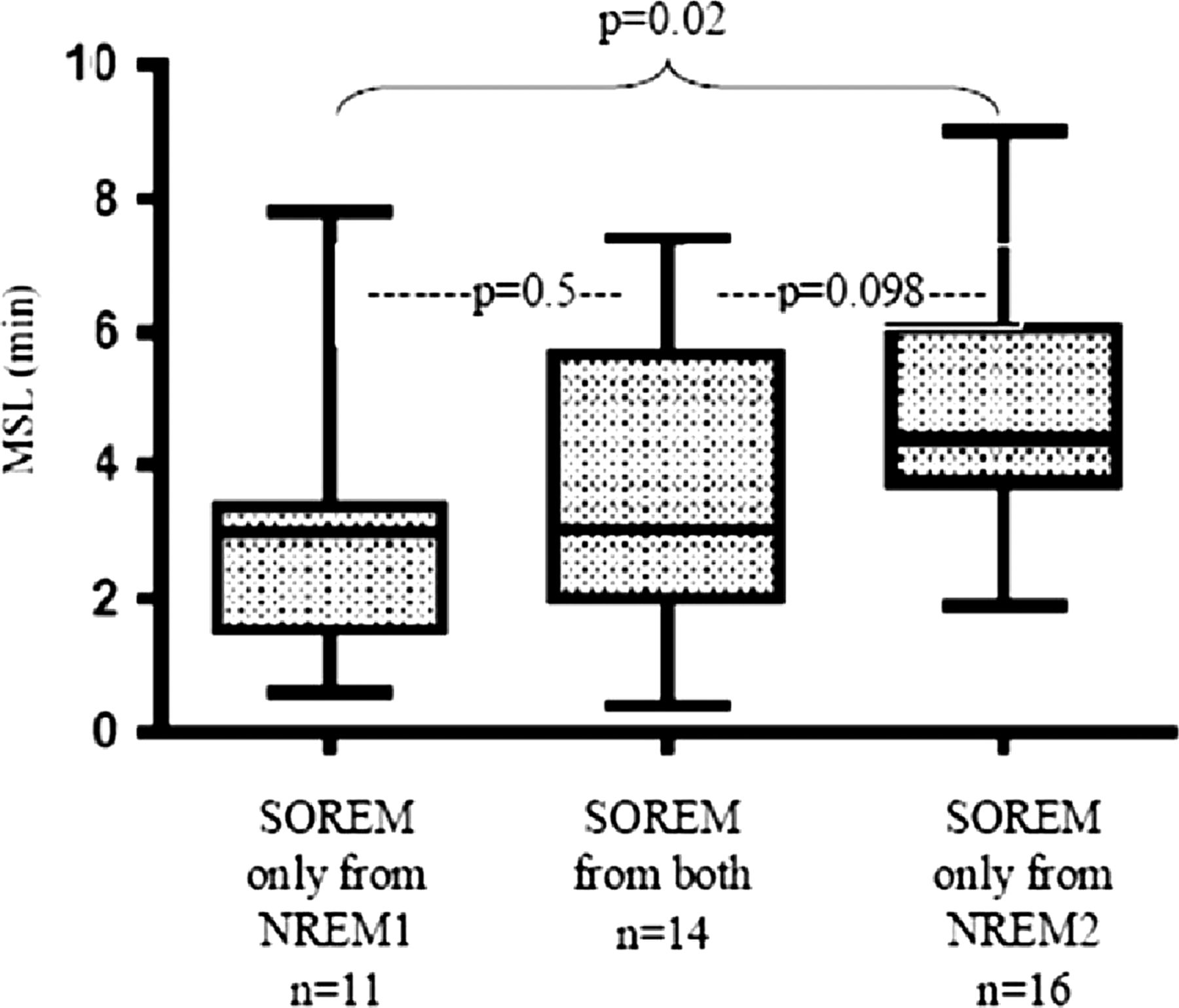
Further analysis of the N+C and N−C groups demonstrated that patients with N+C tended to have all of their SOREM periods arising only from NREM1 more frequently than only from NREM2 (p=0.019); this was not apparent in the N−C group (p>0.05) (table 5). Of the 41 patients in the N−C group, 11 patients had SOREM periods arising only from NREM1, 16 only from NREM2 and 14 demonstrated SOREM periods arising from both stages. N−C patients with SOREM periods only from NREM1 had a shorter MSL (3±2) min than those with SOREM periods only from NREM2 (4.9±1.9) min (p=0.02) (table 6, figure 1). No statistically significant difference in MSL was found between N+C and N−C patients with SOREMP periods only from NREM1 (p=0.14). A correlation was found between MSL and proportion of SOREM periods arising from NREM1 across all patients with narcolepsy (R2=0.286, p<0.0001).
N+C and N−C groups in those with their SOREM periods arising only from NREM1 or NREM2
Mean sleep latency of the N−C patients with SOREM periods only from NREM1, NREM2 or both
{kind=link}
Box-and-whisker plot of the narcolepsy without cataplexy group with sleep onset rapid eye movement (SOREM) periods from non-rapid eye movement sleep (NREM) 1, NREM2 or both. p Values were extracted with ANOVA with post hoc test least significant difference. MSL, mean sleep latency.
Discussion
We have demonstrated that there are significant differences in sleep stage sequencing in SOREM periods between patients with N+C, N−C, IHL, BIISS and PLMD in a retrospective study. In the non-narcoleptic groups, all SOREM periods arose from NREM2. Furthermore, in narcoleptics, most SOREM periods arose from NREM1, and this sequence was more likely to occur in N+C. Only patients with narcolepsy exhibited SOREM periods in the fourth nap, a potential additional discriminator between narcolepsy and other hypersomnias.
In addition, there were significant differences in SOREM period sleep stage sequences between narcoleptic patients with and without cataplexy. SOREM periods with REM arising from NREM1 occurred in 75% of naps containing REM in patients with N+C (similar to that described by Marti et al10) and 51.5% of patients with N−C. Comparison of the N+C and N−C groups demonstrated no significant difference in mean MSL. However, across both groups, the proportion of SOREM periods arising from NREM1 correlated with MSL, suggesting that the difference between the proportions of REM episodes arising from NREM1 may reflect differences in severity of sleepiness. These findings therefore suggest not only differences in the MSL between N+C and N−C, but also significant differences on the basis of SOREM period sleep stage sequences.
It remains uncertain if these differences in SOREM period sleep stage sequence are purely a function of severity of sleepiness, as a consequence of REM instability, other differences in sleep architecture or as a result of greater heterogeneity in the N−C group. Certainly, a previous study has demonstrated that patients with N+C had more awakenings and spent more time in N1 and less time in N2 than patients with other hypersomnias of central origin,16 which may in part explain an increased propensity to REM arising from NREM1 in this patient group. It has also been proposed that two countervailing mechanisms underlie narcoleptic sleep pathology—fragmented nocturnal sleep and increased phasic REM components suggest disturbance of sleep maintenance mechanisms, and specific features of the spectral EEG analysis imply decreased activity in central arousal mechanisms.17 Our findings would certainly be consistent with dysfunction of sleep maintenance mechanisms, with failure of progression into deeper sleep stages and increased REM pressure underlying the tendency for narcoleptics to enter REM from lighter sleep.
The classification of the primary hypersomnias remains problematic, particularly as there remains no gold standard in the diagnosis of these conditions, and our understanding of the pathophysiology remains vague, without clear evidence for or against a shared pathophysiology for N+C, N−C and IH.18 For narcolepsy with cataplexy, a low or absent CSF hypocretin-1 level remains the most specific marker for this condition, however CSF hypocretin levels remain normal in 10% of N+C patients.19 ,20 In N−C, a subgroup shares common markers with N+C—namely a low CSF hypocretin and HLA type—and in these patients a common pathophysiology is assumed.18 However, for those patients who do not exhibit these markers, it is unclear whether they lie elsewhere on the spectrum of narcolepsy or whether an entirely independent pathological process underlies this phenotype. As is well established, in narcolepsy excessive daytime sleepiness is usually the first symptom to appear. Cataplexy can appear simultaneously or with a delay of up to 30 years. 21 ,22 It could be hypothesised that those N−C patients with SOREM periods only arising from NREM1 share a similar pathophysiology with N+C or may represent those that may proceed to develop cataplexy. For IHL, the definition of the condition remains even more unsatisfactory, with an arbitrary cut-off of the MSL of 8 min on the MSLT.
Refinement of the phenotype remains paramount in understanding the pathophysiology and genetics in these conditions, and in the absence of an absolutely specific biomarker, identifying phenotypic features that aid classification will be useful in furthering our understanding of these conditions. SOREM period sleep stage sequencing may therefore provide a further marker, in addition to HLA type and CSF hypocretin, to unravel the assumed heterogeneity of the hypersomnias.
There are major limitations to this study, including retrospective ascertainment of patients, lack of complete information and interpretation regarding HLA typing and CSF hypocretin-1 level, which preclude firm conclusions. Furthermore, the BIISS and PLMD groups were slightly older than the other diagnostic groups, raising the possibility of age related influences on the MSLT, a feature seen in individuals with N+C.23 There is some evidence that aging is connected with a progressive decrease in the number of SOREM periods and a progressive increase in the mean sleep latency, possibly influencing our results. Future prospective studies with age matched groups would eliminate this issue and allow for more firm conclusions. However, it does raise the possibility that sleep stage sequencing of SOREM periods in the MSLT might add further phenotypic data to the effort to dissect out distinct groups of patients within the primary hypersomnia spectrum, particularly among those patients with narcolepsy without cataplexy. It remains unclear as to whether a proportion of N−C patients, especially those that are HLA negative or have normal CSF hypocretin-1 levels, are a separate disease entity or indeed are simply sleep deprived (eg, BIISS). We propose that further larger scale analyses of MSLT sleep stage sequencing should be undertaken, ideally prospectively, and with the benefit of HLA type and CSF hypocretin-1 levels for comparison.
In conclusion, sleep stage sequence analysis of SOREM periods in the MSLT may aid the discrimination between narcolepsy and other conditions with substantial clinical overlap, such as IHL and BIISS. The demonstration of SOREM periods arising from NREM1 or wake raises the possibility of narcolepsy as a diagnosis. In particular, SOREM periods arising from NREM1 or wake and SOREM periods in nap 4 appear to be very strong indicators of narcolepsy. The absence of SOREM periods arising from NREM1 in patients thought to have N−C does not make the diagnosis unlikely, but should raise the possibility that BIISS should be excluded through a sleep diary and/or actigraphy. Sleep stage sequence analysis of SOREM periods has also revealed an inverse correlation between MSL and SOREM periods arising from NREM1, and suggests possible heterogeneity in the N−C group on the basis of an intermediate phenotype, as has previously been described in terms of HLA type and CSF hypocretin-1 levels.
Acknowledgments
The authors would like to thank Dr Joerg Steier, Kate Bridle, Sam Briscoe and Iain Duncan for their help in the undertaking of this work.
References
Footnotes
-
Contributors Analysis, writing design and interpretation: PD. Analysis and writing: AS. Analysis and interpretation: SEH. Interpretation and discussion: CAK, RTM and IOE. Concept and design: AJW. Concept, design, interpretation and writing: GDL.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.