Article Text

Abstract
Background Chronic obstructive pulmonary disease accounts for a significant portion of the world’s morbidity and mortality, and disproportionately affects low/middle-income countries. Chronic obstructive pulmonary disease management in low-resource settings is suboptimal with diagnostics, medications and high-quality, evidence-based care largely unavailable or unaffordable for most people. In early 2016, we aimed to improve the quality of chronic obstructive pulmonary disease management at Bayalpata Hospital in rural Achham, Nepal. Given that quality improvement infrastructure is limited in our setting, we also aimed to model the use of an electronic health record system for quality improvement, and to build local quality improvement capacity.
Design Using international chronic obstructive pulmonary disease guidelines, the quality improvement team designed a locally adapted chronic obstructive pulmonary disease protocol which was subsequently converted into an electronic health record template. Over several Plan-Do-Study-Act cycles, the team rolled out a multifaceted intervention including educational sessions, reminders, as well as audits and feedback.
Results The rate of oral corticosteroid prescriptions for acute exacerbations of chronic obstructive pulmonary disease increased from 14% at baseline to >60% by month 7, with the mean monthly rate maintained above this level for the remainder of the initiative. The process measure of chronic obstructive pulmonary disease template completion rate increased from 44% at baseline to >60% by month 2 and remained between 50% and 70% for the remainder of the initiative.
Conclusion This case study demonstrates the feasibility of robust quality improvement programmes in rural settings and the essential role of capacity building in ensuring sustainability. It also highlights how individual quality improvement initiatives can catalyse systems-level improvements, which in turn create a stronger foundation for continuous quality improvement and healthcare system strengthening.
- chronic disease management
- continuous quality improvement
- evidence-based medicine
- decision support, computerised
- PDSA
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- chronic disease management
- continuous quality improvement
- evidence-based medicine
- decision support, computerised
- PDSA
Problem
At Bayalpata Hospital in rural Nepal, chronic obstructive pulmonary disease (COPD) is among the top three most prevalent non-communicable diseases managed in the outpatient department and one of the most common reasons for inpatient admission. At Bayalpata Hospital, clinical leadership identified a gap between guideline-based management of acute exacerbations of COPD (AECOPD) and care provision. In early 2016, chart audits, provider interviews and clinical observations showed there was a lack of standardised AECOPD management, resulting in wide variation in practice and quality among healthcare providers. Accurate diagnosis of AECOPD was often missed. High-dose intravenous corticosteroids and antibiotics were often used inappropriately for AECOPD, which led to lower quality care provision and higher costs.
Bayalpata Hospital is a 50-bed, government-owned, district-level hospital in Achham, Nepal, managed by a public–private partnership between the non-profit healthcare organisation Possible and the Government of Nepal’s Ministry of Health and Population. Mid-level providers, including paramedics, nurses and medical assistants, make up the hospital’s core clinical staff, supervised by staff physicians and general practitioner physicians.
In this report, we discuss a quality improvement (QI) initiative in a low-resource setting in rural Nepal designed to: (1) improve the quality of COPD management, (2) model the use of an electronic health record (EHR) system for QI and (3) build local QI capacity, with the overarching goal of catalysing broad, long-term improvements in healthcare quality. The initiative aimed to increase appropriate outpatient oral corticosteroid prescriptions to 75% over a 6-month period and demonstrate maintenance of the improvement over an additional 6 months.
Background
COPD accounts for a significant portion of the world’s morbidity and mortality. Per recent estimates, 251 million people currently suffer from COPD while 3.2 million people die of COPD annually.1 2 Of note, 90% of COPD-related deaths occur in low/middle-income countries.3 COPD is the second leading cause of death in Nepal.4 COPD management in low/middle-income countries is suboptimal with diagnostic tests and medications largely unavailable or unaffordable for most people.5 Additionally, prior research has documented gaps in mid-level providers’ diagnostic and clinical decision-making skills in similar settings in Nepal6 and India.7
Globally, quality of care is increasingly seen as a priority, as policymakers are realising the limits of focusing on healthcare access alone. QI and systems thinking have been leveraged to reduce the ‘quality chasm’ in resource-rich settings.8 9 However, in low/middle-income countries such as Nepal, resource-poor healthcare systems struggle to meet population needs and QI infrastructure is limited or non-existent.10 Thus, quality of care is under-researched in low/middle-income country healthcare systems,11 and available research suggests overall care quality to be inadequate.12–14
Several healthcare systems ‘building blocks’ need to be in place to ensure quality care and the success of subsequent QI initiatives. The WHO’s Systems Thinking Framework defines these as service delivery, healthcare workforce, healthcare information systems, access to essential medicines, financing and leadership and governance (online supplementary file A).15 Systems thinking emphasises successful integration of healthcare systems components via attention to context, inter-relationships and the framing of causality as a cycle rather than a one-time event.16 We use this framework to evaluate both the immediate outputs of our COPD QI initiative and the broader impacts on the local healthcare system.
Supplementary file A
Baseline measurement
Our team selected the rate of oral corticosteroid prescriptions (prednisolone) for AECOPD as the primary outcome measure, so as to align with international, evidence-based practices.17 18 The metric served as a proxy for protocol adherence and provider behaviour change. At baseline, only 14% of patients with a documented AECOPD were prescribed oral prednisolone, with the vast majority of patients receiving high-dose intravenous corticosteroids, contrary to evidence-based guidelines. We considered employing the rate of inhaled salbutamol prescriptions as the outcome measure of choice, but we found this to be acceptable, at 92% at baseline. Therefore, our primary aim was to increase appropriate outpatient oral corticosteroid prescriptions for AECOPD to 75% over a 6-month period and demonstrate maintenance of the improvement over an additional 6 months.
In addition, our team chose EHR template utilisation for outpatients with a prior diagnosis of COPD as a process measure, and a secondary proxy for protocol adherence. Given our design of these EHR templates as tools for clinical decision support and standardisation of care provision, we hypothesised that their use would improve adherence to evidence-based practices. At baseline, the COPD template was completed in 44% of encounters with patients who were previously diagnosed with COPD. We chose the target of 75% COPD EHR template utilisation to reflect full uptake of the template for visits pertaining specifically to AECOPD management of known patients with COPD.
Design
We designed our QI initiative to attend to the following goals: (1) improve the quality of COPD management; (2) model the use of an EHR for QI and (3) build local QI leadership capacity via staff sensitisation to QI methods and systems thinking. An overarching aim of the initiative was to demonstrate that small-scale QI initiatives can serve as powerful tools to catalyse systems-level improvements thereby ensuring more effective, higher quality healthcare delivery.
Bayalpata Hospital has several design assets, organised by the WHO Systems Thinking Framework, that facilitated a QI initiative. First, the EHR (online supplementary file B) in use since 201519 comprised templates for common diagnoses, each of which contain a series of questions formatted as point-and-click choices and simple data entry fields. This allowed for the creation of a dedicated COPD template and continuous programme monitoring (Health Information System). Multidisciplinary continuing medical education lectures are held daily, which provided a dedicated time and space to deliver QI-related training and feedback. Mid-level providers are also supervised during routine service delivery and are able to consult with staff physicians and general practitioners for all cases (Health Workforce). Another unique aspect of care delivery at Bayalpata Hospital is a mid-level provider-led outpatient chronic disease counselling programme (Service Delivery). Other assets that facilitated QI were strong hospital leadership and a formal memorandum of understanding with the government detailing the terms of the hospital’s management and expected outcomes (Leadership and Governance); a digitised procurement system integrated into the EHR thereby minimising stock-outs (Essential Medicines Access) and a variety of financing sources including government in-kind and performance-based financing, in-country grants and private donors (Financing).
Supplementary file B
All stages of the initiative were led by a local QI champion in order to cultivate local ownership, increase engagement among colleagues and ultimately, facilitate a culture of continuous QI. A staff physician was recruited to lead this initiative as the QI champion. This individual, under the guidance of a mentor, was responsible for collaborating with relevant team members to: (1) create a standardised protocol for COPD management; (2) integrate the protocol into the COPD EHR template; (3) educate clinicians on the protocol, its rationale and relevant workflow changes; (4) review weekly data and suggest relevant actions and (5) identify enabling or hindering factors. The QI champion received structured mentorship from academic clinicians, including orientation to QI concepts and examples as well as ongoing support for project design and iteration.
Our project design was intended to address known systems gaps, prompting improvements which would facilitate future QI initiatives. For example, we integrated EHR and data use into project design, in order to provide an impetus to improve EHR usability. Finally, local leadership and QI capacity building was prioritised.
Strategy
Systematic reviews have shown that passive guideline and protocol dissemination has little effect.20 21 As such, we designed a multifaceted intervention which would include a process to build local consensus, educational sessions, reminders, as well as audits and targeted feedback. The QI champion monitored process and outcome measures weekly over a 12-month period and facilitated four broad Plan-Do-Study-Act (PDSA) cycles. We summarise the PDSA cycles below and comprehensively document the aim, change hypothesis and strategy for each PDSA cycle undertaken in table 1.
Comprehensive list of Plan-Do-Study-Act cycles undertaken during the QI initiative
PDSA cycle 1: This cycle (containing three components) focused on remedying baseline systems-level gaps: (A) Service Delivery—the QI champion developed a guideline-based local protocol for COPD management (online supplementary file C), adapted to clinician knowledge and resource constraints (limited formulary, lack of arterial blood gas and lack of home oxygen) based on key guidelines including WHO standards and the Global Initiative for Chronic Obstructive Lung Disease protocol.22 23 The QI champion also designed a COPD EHR template that guided users in the diagnosis and management of AECOPD, and recognition of common complications of COPD (online supplementary file D). The QI champion completed protocol development and template creation under the supervision of clinical leadership. (B) Healthcare Workforce—clinical leadership hired an additional chronic disease counsellor for COPD counselling after assessment of COPD patient volume showed that baseline COPD counselling capacity was insufficient to allow for 10 min of counselling per patient. (C) Essential Medicines—clinical leadership added salmeterol to the formulary, which was unavailable prior to the intervention. These components were deployed after the QI champion sensitised staff to management of both stable COPD and AECOPD, the COPD QI initiative and QI concepts more broadly.
Supplementary file C
Supplementary file D
PDSA cycle 2: This cycle focused on a long-term feasibility assessment of the interventions piloted in PDSA cycle 1. (A) The EHR template was modified to be more streamlined per feedback from clinicians after a pilot-testing period. (B) The QI champion prepared and delivered continuing medical education lectures on the availability and appropriate usage of salmeterol after review of EHR records showed low utilisation of salmeterol.
PDSA cycle 3: This cycle focused on institutionalising the endeavours piloted and modified in the previous cycles. Paper copies of the COPD protocol were displayed in clinician working areas and targeted feedback was provided to individual clinicians after review of EHR records showed faltering adoption of the COPD protocol.
PDSA cycle 4: This cycle focused on reinforcing the changes in clinician behaviours institutionalised in PDSA cycle 3 in light of staff turnover. The QI champion conducted continuing medical education sessions regarding COPD, staff orientation sessions to the EHR template, and continued providing weekly feedback to individual clinicians. This was completed after review of EHR records showed a decline in adherence to the protocol which occurred during an influx of a large number of new clinicians, and the departure of many who were familiar with the protocol.
Deidentified and routinely collected data, including prescription and template completion information, were extracted weekly from the EHR system for analysis. The EHR team compiled and distributed these data to the QI champion and mentor. Both the EHR team and the QI champion reviewed the data for accuracy, prompting modifications to the query as needed. For example, we modified the query to identify COPD EHR template completion rate by user and helped identify low-performing clinicians. These data were supplemented as needed by manual chart audits and direct communication with clinicians. The QI champion communicated data to all clinicians monthly during designated continuing medical education sessions. The QI champion also obtained qualitative feedback and reflections via informal conversations with clinicians and leadership as well as continuing medical education discussions. In our discussions, clinicians alluded to healthcare system gaps exposed by, and changes triggered by, the intervention. We have included select quotations to represent these broad themes.
Results
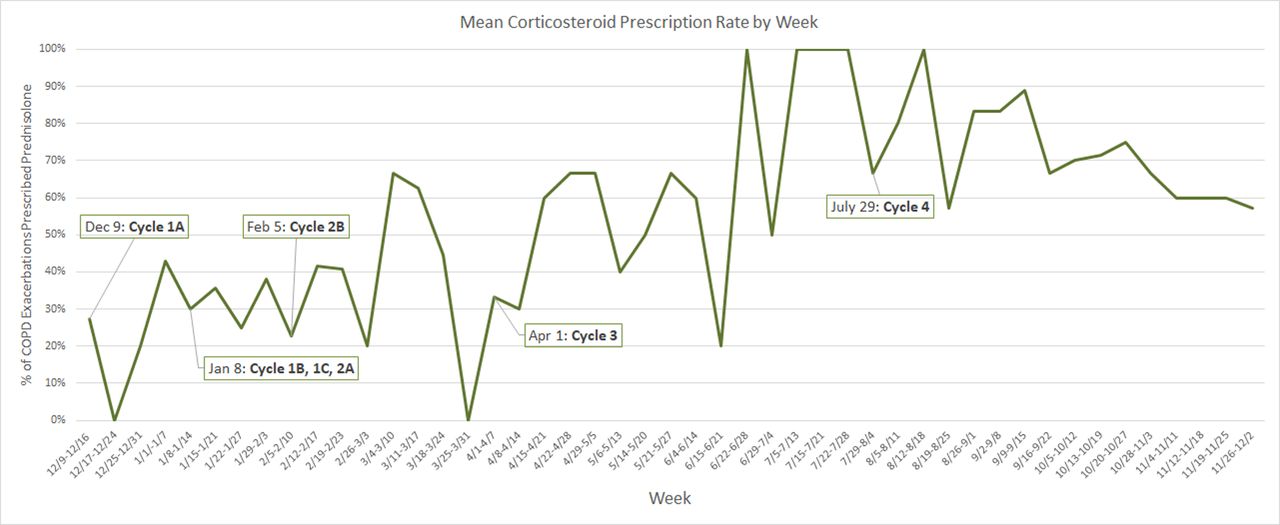
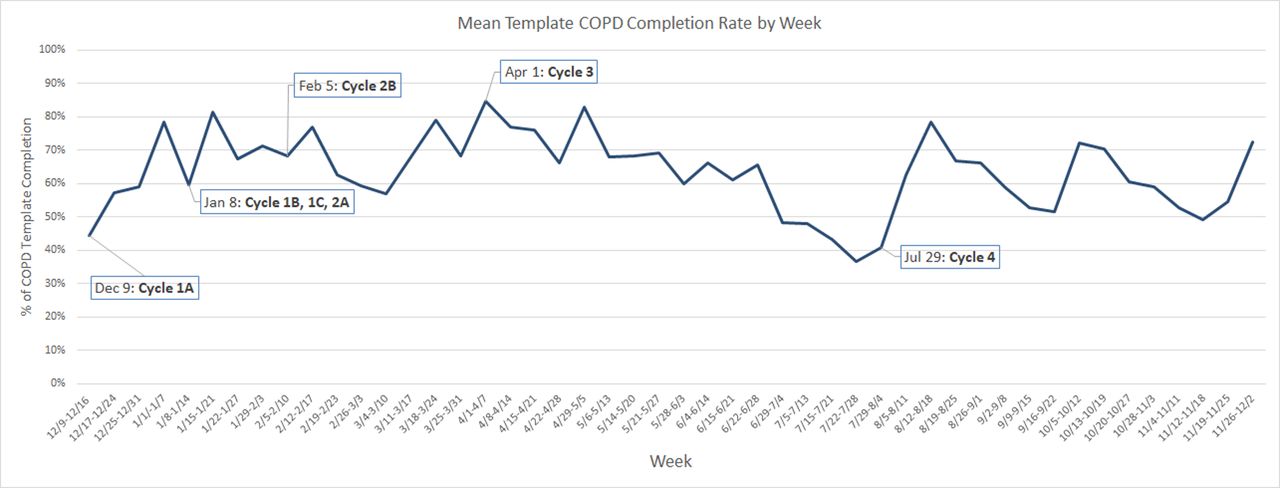
The primary outcome of oral corticosteroid prescription for AECOPD increased from 14% at month 1, to >60% by month 7, at which point the monthly average was maintained for the duration of the initiative (figure 1). Significant changes in the prescription rate correlated with timing of continuing medical education sessions and staff turnover, among other interventions, all of which are noted in table 1. The process measure of COPD EHR template completion rate was found to be 44% in month 1 and increased to >60% by month 2 (figure 2). Template use dropped from month 5 to 8, during a period of large staff turnover, and in the second half of the study period, template use remained between 50% and 70%, below the goal of 75%.
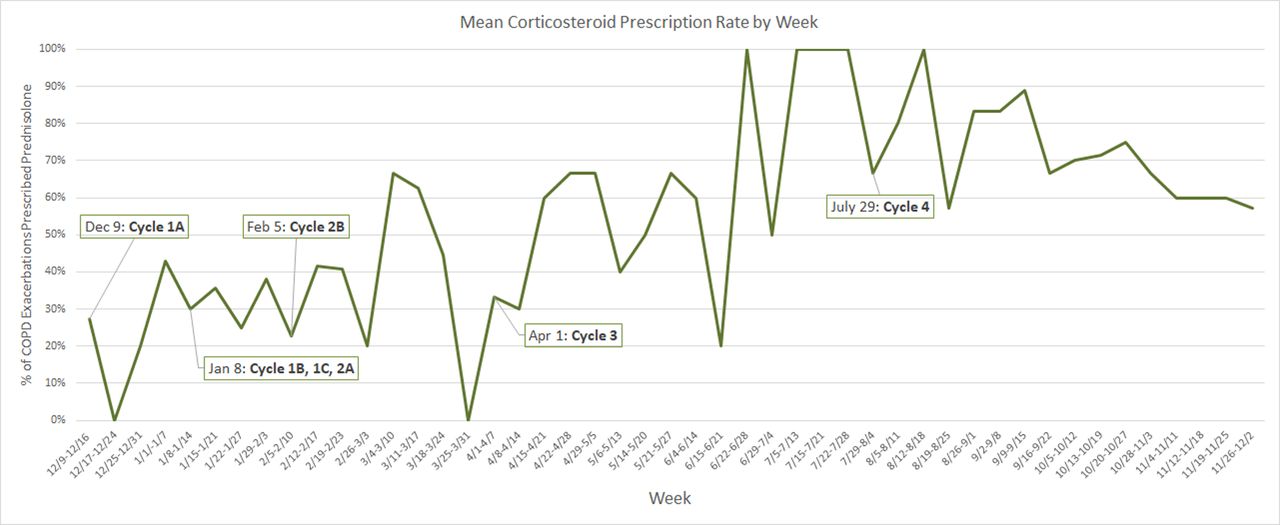
Mean corticosteroid prescription rate based on per cent of chronic obstructive pulmonary disease (COPD) exacerbations prescribed prednisolone by week.

![[bmjoq-2018-000408supp001.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/8/1/e000408/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
![[bmjoq-2018-000408supp002.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/8/1/e000408/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[bmjoq-2018-000408supp004.jpg]](https://bmjopenquality.bmj.com/content/bmjqir/8/1/e000408/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Mean template chronic obstructive pulmonary disease (COPD) completion rate by week.
We noted several themes regarding the behaviour changes (as reported anecdotally, not systematically measured) catalysed by the initiative during our continuing medical education feedback conversations on the initiative’s results. All quotes are from senior clinical staff. One staff physician noted his perception of mid-level provider behaviour after the initiative: ‘[Mid-level providers] are now giving the same treatments as physicians.’ The medical director similarly noted, ‘… you can really see a change in practice of mid-level providers… they are auscultating, and often finding wheezes and stridor… and referring to staff physicians when necessary’. Other comments focused on changing prescribing patterns, with providers feeling that there was an increased awareness that intravenous antibiotics were not needed for mild or moderate COPD exacerbations. Finally, providers felt that they had observed incidents of changed patient behaviour as well. Specifically, they noted that prior to the initiative, patients requested oral formulations of salbutamol, because they were unfamiliar with inhalers but by the end of the initiative, multiple providers noted that patients had begun to request inhaled rather than oral formulations. One staff physician provided an anecdote:
…I was in the old [Outpatient Department] with a patient when we began QI. We began prescribing inhalers. [This] patient threw the metered-dose inhaler on the table and demanded an oral prescription. Most patients wanted oral prescriptions… by the end patients want inhaled prescriptions… now they won’t take oral prescriptions. This was unexpected but was a very positive thing. They, themselves, are saying that inhaled prescriptions are better…
We also observed unanticipated systems-level changes. In response to reported deficits in chronic disease counselling services, an additional chronic disease counsellor was hired (month 2, table 1), and a targeted COPD counselling template was created (Service Delivery, Health Information System). Salmeterol (long-acting beta agonist) was added to the local formulary after it became apparent that this cost-effective and guideline-based medication was unavailable for patients (Essential Medication Access). On seeing the value of a protocol for COPD management, clinical leadership initiated a project to develop protocols and EHR templates for a variety of common conditions, including diabetes, hypertension, asthma, epilepsy, acid peptic disorder and vaginal discharge with plans to fully integrate these protocols into the patient care workflow (Leadership and Governance).
Lessons and limitations
The overall goals of this initiative were to: (1) improve the quality of COPD management, (2) model the use of an EHR for QI and (3) build local QI capacity. Here, we discuss our progress with these goals and the multiple healthcare systems-related lessons embedded throughout our experience.
Improvement in the rate of oral corticosteroid prescriptions for AECOPD, as documented in figure 2, was indicative of an increase in adherence to a guideline-based protocol for COPD management. This constituted a concrete improvement in quality of care and shows that QI initiatives can be successfully conducted in rural, resource-constrained areas of low/middle-income countries. However, a key finding was that despite this evidence of improved protocol adherence, COPD EHR template completion remained relatively low. Thus, the first lesson is that changes in institutional culture and behaviour are multifactorial and that the combination of building local consensus, educational sessions, reminders, as well as audits and feedback likely produced our results. Of note, the use of EHR template completion as a process measure for protocol adherence was complicated by the fact that many patient encounters were ‘proxy visits.’ For patients with limited mobility, family members would present for medication refills (prescriptions capped at 30 days) and the event would be logged as an outpatient encounter, but the template would not be used. Additionally, when patients with COPD presented for alternate acute complaints, or for management of a comorbid disease, the EHR template was infrequently used, which underestimated the number of COPD outpatients. Finally, patients with AECOPD could only be identified when the COPD EHR template was used.
In light of this experience, we can conclude EHR template completion may not be an effective proxy for provider protocol adherence. We had not fully appreciated the barriers to EHR template uptake during project design and would have made other considerations in hindsight. Specifically, high staff turnover, English language formatting and low prior exposure to EHRs were likely key drivers of low EHR template uptake. New providers were continuously learning how to use the EHR and would often leave prior to or just after mastery. As documented elsewhere in Nepal, our mid-level providers reported that the template helped with diagnostic accuracy, but it did not address the nuances of patient presentations and was often time consuming.24 Limited EHR team capacity prohibited dynamic, real-time EHR modifications to meet these provider needs, which led to informal workarounds, rather than systematic EHR changes, which in turn limited the scope of this EHR-based QI initiative. Thus, the second lesson is that the use of technology requires commensurate investments around functionality and system integration. To this end, we will make additional investments in EHR orientation, language formatting, usability and continuous improvement to promote uptake among clinicians. Specifically, we aim to undertake a human-centred design approach25 with future EHR templates and workflows and to invest more heavily in onboarding and staff retention while designing for high turnover.
Building local QI capacity was challenging as most clinicians were unfamiliar with QI concepts, such as PDSA cycles, run charts or root cause analyses. Despite this, one of the initiative’s notable strengths was local ownership, and adaptability in the face of resource constraints. An initial investment was required to orient a local clinician, the QI champion, around QI concepts. In retrospect, the QI champion proved to be crucial for the success of the initiative, with essential roles in brainstorming, generating content, communicating and directing changes, and garnering local consensus. Both the investment in the QI champion and the QI champion’s commitment to the initiative resulted in a cascade of system-wide changes including enhanced service delivery, a better capacitated healthcare workforce and attention to (and consequent investment in) broad healthcare system barriers to quality. For example, medication availability was noted by the QI champion as a barrier through the course of the initiative. Specifically, COPD medications including inhaled long-acting beta antagonists and inhaled corticosteroids were unavailable as they were absent from Nepal’s National List of Essential Medicines (online supplementary file E) but were present on the WHO’s Essential Medicine List.26 The QI champion also noted the need to broaden our scope from patients with AECOPD to patients with stable COPD as well and adjusted the protocol and template to accommodate for either situation. Therefore, the third key lesson is that cultivating local leadership is a critical investment for the success of low/middle-income country QI initiatives and healthcare systems strengthening.
Supplementary file E
There were significant barriers to QI and quality, more broadly, that were specific to our rural setting. Among our patient population, inhaled medications are often not a familiar concept, which resulted in oral rather than inhaled salbutamol being expected by patients and prior to the initiative, often prescribed by clinicians. The context is that >50% of the Achhami population is below the poverty line27 and only 53% is literate,28 thus limiting patient health knowledge and expectations, and informing future considerations for QI. Other limitations flagged for future consideration, included the lack of depth and breadth of process and outcome measures. For example, while provider behaviour changes were reported, these were collected anecdotally rather than systematically. Given limited data collection capability and QI team bandwidth, there were notable gaps in capturing key process measures (eg, inhaled medications), patient experiences (eg, extent to which goals and needs were met over time), long-term health outcomes (eg, hospitalisations, exacerbations, disability) and costs (eg, marginal investments, potential cost savings and cost-effectiveness). Therefore, the limitations illustrated above highlight the unique challenges to QI in low/middle-income countries.
In retrospect, a significant change to project design would have been integrating Bayalpata Hospital’s community healthcare worker programme with facility-based COPD care. Each community healthcare worker is equipped with a mobile phone application with an integrated clinical decision support tool29 30 to provide home-based care (online supplementary file F). Comm unity healthcare workers currently follow-up with each patient with COPD at home every 30 days (or more often if needed), based on a monthly list of COPD outpatients. They assess a patient’s self-reported level of symptom control and screen for alarm symptoms (with facility referral if positive), counsel on COPD risk factors and medication adherence, and coordinate care longitudinally. To date, from the inception of community-based COPD follow-up in mid-2016, 72% of Bayalpata Hospital’s catchment-area COPD outpatients were linked to Bayalpata Hospital via a community healthcare worker, with an aggregate of 2857 follow-up visits completed for those patients, resulting in a median of 8 visits per patient (mean 9.2). We aim to leverage this asset in future QI design.
Finally, the unplanned, broader changes in systems and behaviour, triggered by this intervention support the view of healthcare systems as complex, adaptive and responsive to feedback. QI initiatives can strengthen healthcare systems independent of intended outcomes. They are important tools to uncover previously unknown or underestimated gaps and provide the impetus for foundational changes, which in turn support future initiatives, create robust healthcare systems and improve patient care.
Conclusions
We describe the implementation of a QI initiative at a healthcare facility in rural Nepal. The initiative’s goals were to: (1) improve the quality of COPD management, with specific attention to outpatient AECOPD, (2) model the use of an EHR for QI and (3) cultivate local QI capacity. Importantly, we demonstrate the feasibility of implementing a QI initiative in a rural, low/middle-income country setting. It also highlights the importance of systems thinking, elucidates the healthcare systems components which enable or impair sustainable QI and demonstrates how QI initiatives can catalyse broad systems-level improvements, which create a stronger foundation for continuous QI and healthcare systems strengthening. Moving forward, we aim to initiate additional QI initiatives, covering a range of patient-centred outcomes. When conducted thoughtfully and with long-term goals in mind, the QI process can be as valuable as its outcomes.
Supplementary file F
Acknowledgments
We express our appreciation to the Nepal Ministry of Health and Population for their continued efforts to improve the public sector healthcare system in rural Nepal. We give our thanks to Margaret Kruk and colleagues at the Lancet Global Health Commission on High Quality Health Systems as well as Amit Aryal and colleagues at the Nepal National Commission for their encouragement of our work, and to our EHR technology partner ThoughtWorks. Lastly, we are indebted to the hospital staff whose commitment to serving our patients and dedication to improving the quality of healthcare in rural Nepal continues to inspire us.
References
Footnotes
SM and DJ contributed equally.
DM and DS contributed equally.
Contributors SM, DJ, BD, GD, SKD, BG, TKG, SK, RS, AT, RT, LW, DM and DS conceived and designed the study. NC, RM, SP and AR performed the relevant data quality and extraction processes. SM, DJ, GD, RT and LW analysed the data. SM, AK and DM wrote the first draft of the manuscript. AK, SH, SM, LW and DS edited and revised the manuscript draft. All authors contributed to programme implementation and iteration, contributed to the writing of the manuscript, and reviewed and approved the final manuscript draft.
Funding DM received support for this work from the Office of the Director, National Institutes of Health under an Early Independence Award, number DP5OD019894. The Eunice Kennedy Shriver National Institute of Child Health and Human Development and the National Institute of Dental and Craniofacial Research provided support for this award.
Disclaimer The funders played no role in research design, data collection, data analysis, manuscript write-up or decision to publish. Any opinions, findings, conclusions or recommendations expressed in this article are those of the authors alone and do not necessarily reflect the views of the US National Institutes of Health.
Competing interests SM, AK, GD, RS, LW, DM and DS work in partnership with and DJ, NC, BD, SKD, BG, TKG, SH, SK, RM, SP, AR and AT are employed by a non-profit healthcare company (Possible) that delivers free healthcare in rural Nepal using funds from the Government of Nepal and other public, philanthropic and private foundation sources. At the time of initiative implementation, RT was employed by Possible. SM, GD, BG and LW are academic fellows affiliated to a bidirectional fellowship programme (Health, Equity, Action, Leadership Initiative Fellows) that is affiliated with a public medical school (University of California San Francisco). DJ and DRS are employed by the Government of Nepal. AK is an academic fellow at and DM is a faculty member at a private medical school (Icahn School of Medicine at Mount Sinai). GD is employed part time at a public medical centre (Natividad Medical Center). SH is employed part time at a public university (University of Washington). SK is a graduate student at a private university (Eastern University). RS and DS are faculty members at an academic medical centre (Brigham and Women’s Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. RS and DS are faculty members at a private university (Harvard Medical School). RS is employed at an academic medical centre (Massachusetts General Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. LW is employed by a medical centre (Tuba City Regional Health Care) that is managed using public sector funding through the Indian Health Services. DM is a non-voting member on Possible’s board of directors but receives no compensation. DS is employed at an academic medical centre (Beth Israel Deaconess Medical Center) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. DS is employed at an academic research centre (Ariadne Labs) that is jointly supported by an academic medical centre (Brigham and Women’s Hospital) and a private university (Harvard TH Chan School of Public Health) via public sector research funding and private philanthropy. All authors have read and understood BMJ Open Quality’s policy on competing interests and declare that we have no competing financial interests. The authors do, however, believe strongly that healthcare is a public good, not a private commodity.
Ethics approval This study protocol was approved by the Nepal Health Research Council, registration number 472/2017.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Deidentified data will be made available at the Healthcare System Design Group’s, Possible’s Implementation Research Team website (http://hsdg.partners.org/). Data may also be requested by emailing: research@possiblehealth.org.
Patient consent for publication Not required.