Article Text

Abstract
Objective To explore medication-related burden (MRB) and patients’ lived experience with medicines (PLEM) without regard to particular medication therapies or medical conditions.
Design Systematic review and metasynthesis of qualitative studies.
Data sources MEDLINE, EMBASE, International Pharmaceutical Abstracts, PsycINFO, Global health, CINAHL and Web of Science were searched from January 2000 to August 2014 using medication burden and patients’ lived experience terms.
Synthesis methods Synthesis was undertaken following metaethnography methods and a comparative thematic analysis technique.
Results 34 articles from 12 countries with a total of 1144 participants were included. 3 major inter-related themes emerged central to PLEM: MRB, medication related beliefs and medication taking practice. The negative impact of MRB, due to its interference on patients’ daily lives and effects on well-being, its influence on patients’ beliefs and behaviours, and a potential risk for drug-related problems (DRPs) was evident. This resulted in non-adherence and poorer outcomes (unachieved therapeutic goals and damage to patients’ health). Patients who experienced MRB interference in their life over time begin to juggle their medicines. Others continue their medicines despite experiencing MRB resulting in compromised physical, social or psychological well-being.
Conclusions There is a shared commonality of PLEM among the studies. MRB plays a central role in influencing patients’ health and well-being, beliefs and behaviour towards medicines. Given the complexity of MRB and its impact evident from this review, there is a need for healthcare practitioners to have insight into PLEM in therapeutic care plans. Understanding PLEM is an opportunity for practitioners to identify particular MRBs that patients encounter, and provide individualised care through selection of therapeutic care plans that suit a patient's life. This may assist in helping to achieve patients’ medication-related needs, and improve medication therapy and health outcomes.
- GENERAL MEDICINE (see Internal Medicine)
- PRIMARY CARE
- QUALITATIVE RESEARCH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first metasynthesis to explore medication-related burden, and patients’ lived experience with medicine (PLEM), in-depth.
This metasynthesis uncovered individuals’ reality of living with medicine, the burden they encountered in their day-to-day life and its impact on beliefs and behaviours, health and well-being.
Our findings have clinical implications for practitioners to consider PLEMs in therapeutic decisions, so that individualised care maximises adherence to care plans and the success of therapy.
This review has highlighted that the medicine-lived experience area must be considered to enhance successful therapeutic decisions and outcomes, and areas that require further investigations.
The review was limited to the experiences of individuals from 12 countries; however, a comprehensive conceptual model of PLEM can be transferable across a wide range of medications and medical conditions.
Introduction
Patient experience is a concept that has been gaining attention as a key element of quality healthcare.1 In recent years, there has been growing recognition of the importance that patient-reported outcomes (PROs) have to healthcare services,2–5 clinical practice6 ,7 and outcome research.8–10 There is also increasing interest and experience of using evidence from patient-reported outcome measures (PROMs) data to improve healthcare quality.4 ,11–13 The use of patients’ experiences and reports are now valued and considered essential to improve healthcare safety and patient outcomes.4 ,12 ,14–16
Patients’ medication experience has been described as ‘the sum of all events involving drug therapy that a patient encounters in his/her life time’.17 Using a PROs concept, it is ‘…a report that comes directly from the patient, about any aspects of his/her medicines lived experiences, without interpretation of the patient's response by a clinician or anyone else’.8 ,18 The experiences that a patient has with medicine can be positive, negative or both. Positive experiences with medicines lead to improved control of patients’ symptoms or disease conditions and clinical markers, while negative experiences can manifest as adverse events (AE), poor disease control, inconvenience or inappropriate use of medicine. Patients respond to the burden of medicine/s to maintain their day-to-day life alongside their medication therapy. However, the burden may influence adherence to treatment19 ,20 and patients’ health.20 ,21 Therefore, in making therapeutic decisions, a ‘minimally disruptive medicine’22 approach together with attention to patients’ lived experiences is a strategy worth considering to minimise MRB and optimise adherence to medication and patient outcomes.
Nevertheless, although medicines represent the most common form of therapy in the management of various medical conditions, patients’ experiences with medicines has limited consideration in practice.17 ,23 Attention to patients’ difficulties with treatments is not optimal during consultations,24 ,25 and practitioners are often unaware of the challenges patients encounter with their treatments.24 ,26 Furthermore, clinicians give less attention to patients’ psychosocial information compared to biomedical factors27 in making therapeutic decisions. Additionally, beyond the brief medication history chart, there is no other simple measure of patients’ medicine lived experiences that may aid clinicians to have insight into their patients’ contexts, therapeutic decisions and care plans.
In the last few years, there has been increasing efforts to conceptualise treatment-related burden in chronic illness.20 ,21 ,24 ,28–32 However, existing studies have been primarily qualitative21 ,29 ,31 ,32 and reviews have been limited to either single20 or selected medical conditions.30 Moreover, less is known about medicines-attributed burden,20 such that further exploration of individuals’ experiences with medicine is needed.30 To date, multifaceted dimensions of MRB and patients’ experience with medicines across a broad range of medical conditions has not been examined. Hence, there is a need to comprehensively review and synthesise existing qualitative studies to conceptualise the burden attributed to use of medicines, and how MRB influences PLEM/s. This review aimed to explore MRB, and understand PLEM/s regardless of medication therapies and medical conditions.
Methods
Literature search strategy
MRB is not a standard Medical Subject Heading (MeSH), hence, there was a need to first undertake a ‘scoping search’ prior to a formal search of databases. Using our own experience and expert consultation, this was initially carried out via PubMed, Google Scholar, and preliminary searches of medical, nursing and pharmacy journals to identify key papers and familiarise ourselves with concept terms. A systematic search was then conducted in Medline, PsycINFO, Global Health, International Pharmaceutical Abstracts, PubMed, EMBASE, Web of Science and CINAHL to identify articles published between January 2000 and August 2014. A sensitivity analysis carried out after the initial database search suggested the development of a two-pronged comprehensive search approach for different databases, as neither approach on its own was specific to all databases. For the first five databases (MEDLINE, PsycINFO, Global health, International Pharmaceutical Abstracts and PubMed), the search centred around three main concepts: ‘patient’, ‘medication’ and ‘lived experiences’ (see online supplementary table S1). An additional fourth concept was added, which focused on medical conditions. The fourth search concept was used to capture medication burden, both in acute and chronic illnesses. It was also done to make our review more comprehensive and to limit the retrieved articles only to those that had explored patients’ real-life experiences. ‘Patient’-centred terms included: patient, caregiver, consumer, people and health personnel. ‘Lived experiences’-centred terms included: experience, perception, attitude, preference, expectation, satisfaction, belief, view, opinion, concern, burden, hassle, knowledge. ‘Medication’-centred terms included: medic*, drug*, and treatment*.‘Medical conditions’-centred terms included: chronic illness, acute illness. The detailed search strategy for the other three databases (EMBASE, CINAHL and Web of Science) is reported in online supplementary table S1.
Inclusion and exclusion criteria
Studies with descriptive or interpretive qualitative methods and secondary analysis of primary qualitative empirical data were included if MRB was considered as a major focus, or if they described patients’ beliefs about medicine or medication-taking behaviours with medication burden as a domain. Studies conducted in any settings (primary, secondary or tertiary care) or geographical locations independent of the number as well as types of medications and medical conditions were included. Studies were also considered for inclusion if they explored PLEM from the healthcare professional, consumer health organisation, or care givers perspectives. Articles that involved direct patient contact or observation such as in-depth or semistructured interviews, focus groups with qualitative methods to identify themes discussed by participants, or quantitative surveys with qualitative data analysis were included. Articles that involved indirect patient contacts using qualitative document analysis such as secondary analysis of primary qualitative data or analysis of patients’ diary of medication experience were also included. All inclusion and exclusion criteria can be found in online supplementary table S2.
Article screening and data extraction
The titles of all retrieved studies and abstracts of selected studies were screened. Articles including relevant information on MRB and PLEM were considered for full-text analysis. The data extracted included year of publication, study population, country, design and settings, sample size and technique, studies' core focus, themes and subthemes explored, participants’ quotes and their interpretations by primary authors. Studies were first selected and screened by one author (MAM), and then independently reviewed by RJM, TFC and then approved three authors.
Quality assessment
Currently, there is no agreement on the best method to appraise the quality of qualitative studies,33 and the value of appraisal remains controversial. Moreover, evidence is lacking on whether quality appraisal improves the reporting quality of qualitative research.34 ,35 Some authors prefer to appraise articles on the basis of their conceptual input.36 We assessed the comprehensiveness of reporting in included articles using the Critical Appraisal Skills Program (CASP) checklist.37 Since our primary aim was to understand the broad dimensions of MRB and PLEMs, studies were not excluded on the basis of their quality. Thus, the purpose of the appraisal was to assess transparency of reporting in each included study. The relevance of studies content to our objective was also assessed using a criteria described by Dixon-Woods et al.33 After the assessment, studies were categorised as key papers (providing multiple dimensions of PLEM), and satisfactory papers (providing data on at least a single aspect of lived experience with medicine such as patient beliefs about medicine).The assessment was first carried out by MAM, and then independently by the other two authors (RJM and TFC).
Data synthesis
Classic metaethnography methods38 and comparative thematic analysis (CTA) approach39 were adopted. A combination of metaethnography and other methods has been successfully used in previous reviews.40–42 Metaethnography is an interpretive approach that involves identification and synthesising of shared concepts across studies. It adds depth into the studied topic by reconceptualising and interpreting identified concepts to create new insights. Compared with other methods, it is the most explicit method in terms of its approach to data synthesis,43 ,44 and the attempt made in preserving the original meaning of the studies is one of the key strengths of this method.34 ,45 Noblit and Hare38 outlined seven steps of conducting metaethnography: (1) getting started; (2) deciding what is relevant to the initial interest; (3) reading and rereading of included studies, that is, listing and noting key themes and metaphors (concepts) within studies, (4) determining how the studies are related, that is, similarities and differences, (5) translating studies into one another: reciprocal, refutational, line of argument, (6) synthesising the translation and (7) expressing the synthesis. Although the seven steps of conducting metaethnography and types of translations are explicitly outlined, the actual process of synthesis is not clearly stated.46 The lack of clarity in how the synthesis carried out has been criticised in several studies.47 Moreover, the approach towards translating studies such as ‘first identified translated first’, or ‘the oldest paper translated first’, may not always be possible and is challenging, particularly in managing large amounts of data and studies with different perspectives.46 Practically, it is not easy to ensure whether the quality of a paper starting with the translation process is better than subsequent papers when there is no agreement on how to decide a high-quality study.48 ,49 Additionally, the paper with which the translation begins may sometimes be of a conceptually weak study affecting the subsequent translations.
To ensure transparency and facilitate manageability of the data, we modified steps 3–6 of metaethnography methods using CTA approach. In our review, major themes and subthemes of included studies were selected and summarised in tables. After looking at the relationship between categories of each theme, we then reorganised all the themes and grouped them together to build a broader coding frame of comprehensive analytical themes (third-order constructs).50 The analytical themes were constructed in a way that covered breadth of articles reviewed and also assigned nodes/subthemes to simplify the coding process. Studies were exported from EndNoteX7 to Nvivo10 (QRS International, Victoria) to manage the data, facilitate coding of participants’ quotes (first-order constructs)51 and authors’ interpretations (second-order constructs),51 and to look for additional emerging themes and further refine the coding frame of analytical themes. Using our analytical themes coding frame, participants’ quotes under the heading ‘Results’ section, and their interpretations, were coded to the relevant analytical theme. As studies were conducted in inter-related but different areas, we used the CTA approach to rigorously analyse and systematically code the data (first-order and second-order constructs) to a particular node of our analytical themes, and then thematically analyse the coded items under each theme. The data were coded under similar themes with the same name as in the original studies, or recoded under a different theme where it was conceptually appropriate. The coding framework of our analytical themes was further refined based on emerging concepts from the coded data. We carefully analysed all the coded data within each theme to relate what each study stated about the specific theme and its dimensions. We then carried out the synthesis (step 6) of the data under each theme and complemented our synthesis by citing supporting evidences from primary studies and quotes of participants, when necessary. Finally, we constructed the ‘line of argument’ to explain summaries of our synthesis and the theoretical insights generated from the synthesis. The PRISMA guideline52 was followed to report the findings (see online supplementary table S3), and the protocol prespecifying the review methods is found as online supplementary text S1.
Reflexivity
The worth of a given metasynthesis is judged on the grounds of its final output.45 The final output, in this case, the synthesis, reflects the interaction between researchers and the data. Reflexivity accounting helps readers of the final output to assess the extent to which the perspectives of researchers such as their prior views and experiences may have influenced the data. Our review was conceived with a limited prior knowledge of MRB and PLEM, and thus, we believe this has limited the bias of our own experiences influence on the data. MAM recognised the gap and the need to further research the burden attributed to medicine20 and how individuals live with their medicine.30 MAM had little prior experience of MRB and PLEM-related research. Thus, to minimise bias, all the data extraction was first carried out by MAM and then independently checked by RJM and TFC, and then approved by three authors. The generation of themes to develop the coding framework was closely supervised by TFC and then reviewed by RJM. All authors were involved in each stage of data collection and analysis. MAM drafted the manuscript and RJM and TFC reviewed the manuscript.
Results
A total of 4047 studies were identified. After a thorough review of full-text versions of 122 studies, 34 studies which met eligibility criteria were included in the review (figure 1).
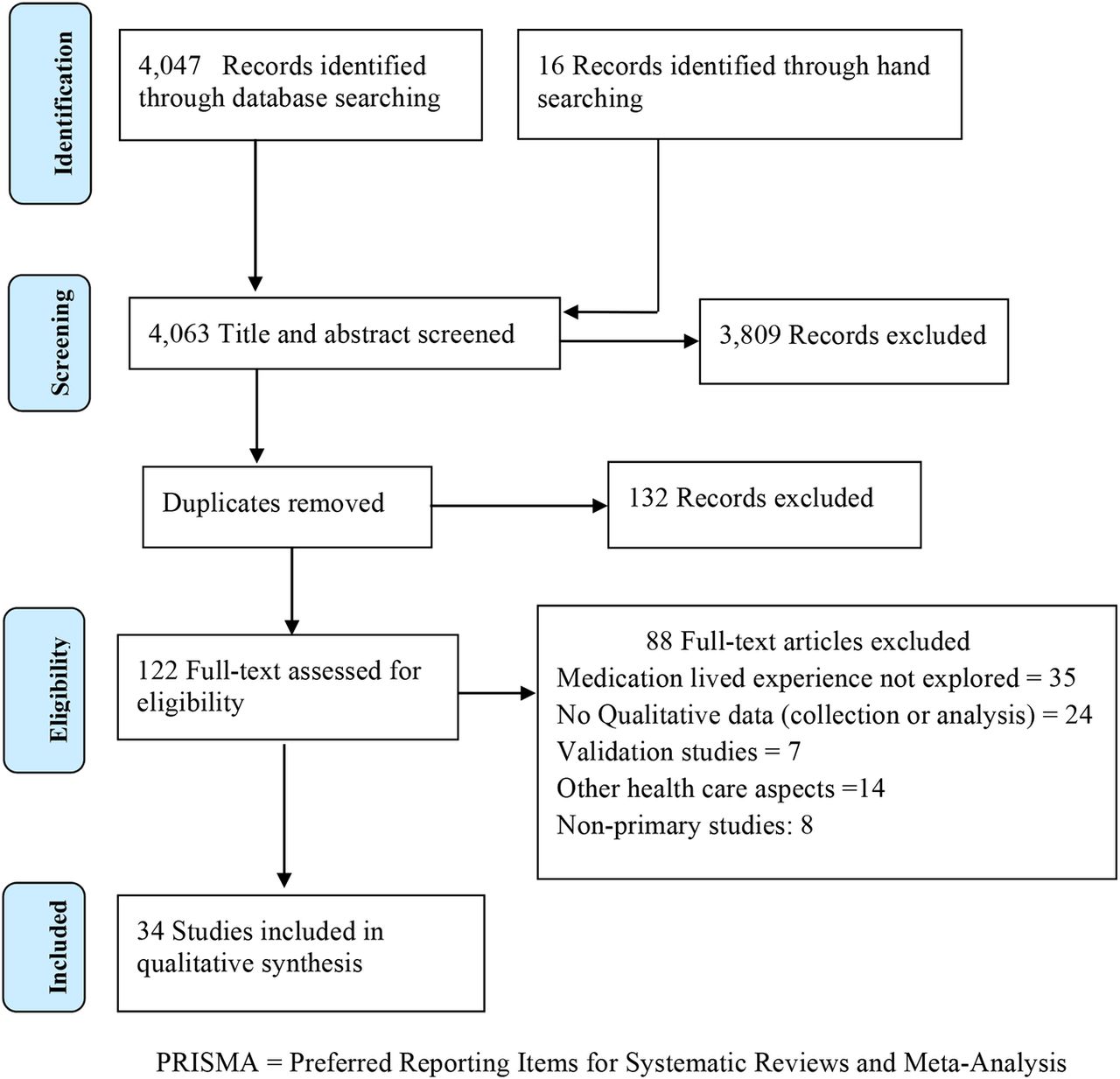
PRISMA flow chart.
Characteristics of included studies
Included studies used focus groups, in-depth, semistructured, face-to-face and telephone interviews with 1090 patients of differing ages, living with different medical conditions and taking 1 or more medicines on a regular basis. Fifty-four other participants (endocrinologist, nephrologist, general practitioners, pharmacists, consumer health organisations’ representatives and others) were also included. In one study, authors used a secondary analysis of data from prior primary qualitative study, and one study used patients’ diary of medication experiences. The studies were conducted in 11 different countries; 11 in the UK, 6 in the USA, 6 in Australia, 2 in Canada, 2 in Sweden and the remaining 8 in other countries (table 1). The study settings included: community pharmacies and participants’ homes; primary care settings including outpatient clinics or health centres; long-term care facilities; hospitals; advanced practice sites; organisational offices or research centres.
Characteristics of included studies
Quality assessment
Studies were generally found to be of a reasonable quality. In some studies, description of data analysis rigour, data collection methods and appropriateness of the research design to address aims of the study were not explicitly stated (see online supplementary table S4). The relevance of studies using Dixon-Woods et al33 assessment criteria revealed 26 articles as key papers, and the remaining eight articles as satisfactory in terms of their content relevance to our review aim (table 1).
Synthesis of findings
Three inter-related major themes and 13 subthemes that explained PLEM emerged; MRB , medication-related beliefs and medication-taking practice. For the purpose of analysis, we used the concept of the Theory of Planned Behavior (TPB)53 to explain subthemes under medication-related beliefs, in relation to MRB as an antecedent factor, and medication-taking practice as an outcome (a target behaviour). Identified themes and subthemes with selected first-order and second-order constructs are shown in online supplementary table S5. The inter-relationship between identified themes is illustrated in figure 2.

{kind=link}
{kind=link}
Conceptual model of patients’ lived experience with medicines (PLEM).
Identified themes of PLEM
We identified a gap in the literature regarding the burden attributed to medicine use.20 Data analysis also suggested that MRB was an antecedent factor that influenced other themes of PLEM. And thus, increased focus was placed on explaining themes of MRB and its impact on other themes of PLEM.
Medication-related burden
In all the included studies, participants talked about at least one category of MRB with the following five subthemes identified as dimensions of MRB: (1) burden of medication routines, (2) burden of medication characteristics, (3) burden of medication AEs, (4) healthcare and associated medication burden and (5) medication-related social burden.
Burden of medication routines
The burden of medication routines referred to adapting challenges of living with medicine; activities of managing the hassle of medicines, and strategies to solve challenges of routines.
The burden of medication routines was one of the most commonly cited21 ,29 ,31 ,32 ,54–72 burdens that patients encounter. It is a patients’ subjective experience in response to physical, psychosocial and financial impacts of medicines to maintain their daily lives, health and well-being. Participants voiced a variety of strategies to manage medicine routines, such as relying on family and others support,55 negotiating with healthcare providers,32 ,58–60 ,63 ,65 ,68 ,69 ,72–74 and using their own strategies,21 ,28 ,32 ,54–56 ,58–60 ,62–64 ,66 ,72 ,75 for example, keeping regular records, adjusting their own schedule, seeking further information, or tools to assist, such as pill organisers. Time to learn about, administer, monitor and access, and travel with medicines were described as common elements of the burden of managing medicine routines.21 ,29 ,31 ,58 ,68–70 In the process, some patients managed, controlled and adapted the routines into their daily life,21 ,32 ,55 ,56 ,58–61 ,64 while others recounted that the hassle of managing the routines negatively impacted their daily life.21 ,63 ,72 Lack of, or inadequate family76 and social support,31 ,63 ,77 complex medication regimens,58 ,61 ,71 challenges of the healthcare system,21 ,29 ,71 ,76 accessibility and cost,61 ,69 and poor communication with healthcare providers,21 ,56 ,78 exacerbated the burden. Participants reported that routines of medicines overlapped with activities of daily life,21 ,28 ,55 ,60 ,63 ,64 ,69 ,71 ,72 ,79 ,80 causing inappropriate medicine-taking behaviour which included unintentional skipping55 ,60 ,69 ,80 (see quote 1 in online supplementary table S6), and intentionally modifying medication regimens28 ,63 ,79 (see quote 2).
Burden of medication characteristics
The concept of burden of medication characteristics was noticeable across studies.21 ,31 ,54–56 ,58 ,60–62 ,65 ,68 ,69 ,71 ,74 ,76 ,79 These included: the complexity of the number of medicines;21 ,58 ,71 ,79 medicine regimen58 ,61; pill size69 and shape;62 the exchange of medication brands,31 ,65 ,68 and challenges of packaging69 or additional instructions.21 ,54 ,68 Inconvenience of dosage forms, pill size and taste appeared to negatively shape patients’ perceived control over medicines.80 Individuals expressed overwhelming feelings of the burden of dealing with the complexity of medicines. Inability to manage this burden, being sceptical about medicines’ character, and the information provided, reinforced negative emotions towards medicine.21 ,56 ,66 ,71 ,76 ,79 Some patients considered an increase in medicines dose or number, or being on multiple medicines on a daily basis, was a sign of losing control,79 whereas for others the notion of taking medicines regardless of its number was considered vital to maintain their health and well-being (see quote 3).56 ,60 ,61 Exchanging of brand for generic medicines caused feelings of insecurity, confusion of the indication, risk of mixing up medicines, and leading to poor medication-taking practice (see quote 4).31 ,63 ,65
Burden of medication AEs
One of the most challenging aspects of living with medicine was experiencing AEs.21 ,29 ,31 ,54–56 ,58–61 ,63 ,67 ,69 ,73 ,74 ,76 ,77 ,79–81 The studies detailed a range of AEs from minor and tolerable to severe and life threatening that affected an individual’s quality of life. Its impact was consistently raised in relation to emotional distress related to present or past experiences of events,21 ,29 ,31 ,56 ,59 ,61 ,63 ,67 ,69 ,71 ,73 ,76 ,77 ,81 anxiety of future occurrences,57 ,63 ,64 ,81 impact on perception of self, and the need to maintain a meaningful life.63 ,81
The disturbing negative impact of AEs on individuals’ quality of life,60 ,63 ,67 ,69 ,76 ,79 ,80 ,82 and the embarrassing public image associated with some AEs was reported by some patients.59 ,80 ,82 The physical or psychological impact of medicine AEs damaged patients’ emotions and shaped their beliefs towards medicines especially when they experienced the impact in their own life21 ,29 ,31 ,56 ,58 ,59–61 ,63 ,67 ,69 ,73 ,74 ,76 ,77 ,81 or observed it in others.79 Some expressed emotions of undesirable bodily effects (see quote 5)63 including impact on sexual well-being (see quote 6).29 ,77 ,79 Others recounted how AEs shaped their beliefs29 ,76 and behaviours towards medicine (see quote 7).76 Individuals used a range of coping strategies to either manage or avoid the AEs, including juggling the dose or stopping the medication alltogether,54 ,60 ,74 ,61 particularly when the AE was not tolerated, or worse, than the problem it was treating. For others, the AE led to inappropriate medication-taking practices, putting them at risk of potential medication-therapy problems.55
Healthcare-associated medication burden
One of the most widely cited dimensions of MRB was related to the challenges associated with being recipients of healthcare within a complex healthcare system.21 ,28 ,29 ,31 ,54–56 ,58–65 ,69 ,71–73 ,76 ,78 ,81 Systemic obstacles of healthcare delivery, provider–patient relational aspects, and financial burden associated with healthcare services and medications costs were commonly described.29 ,31 ,56 ,61 ,69 ,71 ,76 Time spent on travel, and waiting time in a facility (eg, hospitals/clinics/pharmacies) to obtain medicines, alongside transportation costs, were voiced as common burdens.21 ,29 ,31 ,63 Attending multiple facilities, travelling extended distances to facilities and financial challenges (eg, low income, unemployment) appeared to intensify the burden (see quote 8).21 ,31 ,71
The cost of medicines was a troubling financial burden (see quote 9).21 ,29 ,31 For some, its psychological impact was evident (see quote 10),21 ,29 and for others, unavailability of medicines, coupled with their financial costs, was a cause of inappropriate use of medicines (see quote 11).76 Financial burden of medicines negatively influenced some individuals’ well-being as a result of compromised family and social life. In some cases, this resulted in internal conflict and unpleasant feelings (see quote 12).29 ,31
Inadequate, conflicting, and sometimes contradicting information about medicines, were persistently highlighted as commonly encountered medicine information burden.28 ,31 ,56 ,58–63 ,65–68 ,72 ,75–78 For some patients, the cursory style of medicine information provision in the healthcare facility resulted in a challenge to fully understand their medication therapy management plan (see quote 13).65
Failure of healthcare providers to consider a patient's lived experiences, the relationship as a partnership, and some unacceptable consultation styles were voiced as common healthcare-associated burden that adversely affected patients’ trust in healthcare providers (see quote 14).21 Lack of continuity and networked care hindered patients in establishing therapeutic relationships with healthcare providers, affecting patients’ confidence in providers and therapeutic plans (see quote 15).21 ,28 ,29 ,31 ,62 ,63 ,65 ,66 ,71 ,72 Coordinated care, ease of access to the healthcare services, and patient–provider therapeutic partnership appeared to enhance patients’ confidence in the provider and satisfaction with the care plan.32 ,55 ,58 ,59 ,61–67 ,72 ,74 ,75 ,77 ,81 ,82
Medication-associated social burden
This refers to the social (eg, family, friends and public) influence on medicines use and the impact of medicines use on an individual’s social life, such as holidays, visiting family or friends. On the contrary, the influence of family, social connections, public views and comments on medicine users were noticeable across studies.21 ,31 ,32 ,54 ,55 ,56 ,61 ,63 ,64 ,67 ,76 ,77 ,79 ,80 Medicines use associated social burden, such as social isolation, often altered patients’ relationships with family and friends. Some patients recounted the encountered social stigma,56 and others shared the story of medicine-associated stigma from family and friends (see quote 16).56 The lack of public understanding had a detrimental impact on patients’ beliefs about medicine, the concept of self and self-confidence affecting their activities of social life. The fear of social stigma associated with medicine use had significant psychological burden on patients’ life that may have triggered further isolation. A sense of disruption was demonstrated by some patients (see quote 17).63 Conversely, the benefit of social support (eg, family members) in assisting self-care and proper medicines use was evident (quote 18).21 ,28 ,32 ,61 ,64 ,67 ,80
Medication-related beliefs
We described the identified subthemes under this category using an adapted TPB. The concept of TPB helped us to identify and separately analyse individuals’ normative beliefs, control beliefs and behavioural beliefs in relation to MRB and medicine-taking practices as a target behaviour. This section mainly focuses on MRB factors influencing patients’ beliefs in relation to their medication-taking behaviour.
Family, healthcare providers and public influence on patients’ beliefs (normative beliefs)
Analysis of first-order and second-order constructs revealed two concepts; healthcare providers’ behaviours influence on patients’ beliefs,56 ,58 and how family members and others influenced individuals’ beliefs and behaviours towards medicine. It was evident across studies that partners or spouses, family members, friends and other people were the common salient groups that appeared to influence patients’ beliefs about medicine.21 ,31 ,32 ,54 ,55 ,56 ,61 ,63 ,64 ,67 ,74 ,76 ,77 ,79 This influence on beliefs, in turn, seemed to impact individuals’ behaviour towards medicine. Some patients noted that the influence of family members led to unjustifiable use of medicines (see quote 19),56 while others recounted that the medicine they started using, based on another individuals’ experience, resulted in undesirable outcomes (see quote 20).55
MRB intensity and individuals’ coping skills (control beliefs)
This theme referred to how two related factors, the intensity of MRB and the coping skills of the individual, influenced the perception of the individual to control their use of medicines. The ability to cope and engage with proper use of medicines was associated with self-perception of the individuals’ coping threshold and prior experience with medicines use, healthcare system, and services. Many participants stated that medicines routines interfered with personal and social life beyond their ability to cope, and consequently, were key barrier to engage in proper medicines use (see quote 21).21 ,28 ,55 ,56 ,63 ,64 ,80 To cope with or control the interference attributed to medicines routines on daily life (eg, personal schedules, travelling), patients adjusted or changed medications regimens, often without the knowledge of their healthcare professionals. However, some patients’ perceptions and problem-solving strategies appeared to likely result in drug-related problems (DRP) and negative health outcomes (see quotes 22 and 23).28 ,63
In addition, other barriers which influenced an individual's belief about medicines included lack of transport, and inadequate information about medicines and healthcare services.28 ,32 ,56 ,58–63 ,66 ,71 ,78 ,81 Patients stated that medicines were prescribed without consideration of their personal issues.59 Some reported unmet expectations and a need for medicines information, particularly on how to manage and integrate medicine routines into daily life.60 Comprehension difficulties28 ,31 ,56 ,57 ,59 ,62 ,63 ,67 ,76 ,78 ,79 ,81 due to inadequate or conflicting information about medicines acted as a barrier to proper medicine use (see quotes 24 and 25). Healthcare providers’ inattention to patients’ lived experiences was a key barrier that made patients develop negative perceptions towards medicines and care plans (see quote 26–28),56 ,59 ,63 and resulted in medicine-taking difficulties (see quote 29).69
It was evident that patients undertake a range of activities when their expectations and needs were not met due to inadequate healthcare support.32 ,59 ,63 Conversely, some individuals objected to the idea of undertaking extra activities to seek further information, deferring the responsibility to healthcare providers (see quote 30).64 ,65 ,81
The burden of medication characteristics21 ,55 ,58 ,60 ,62 ,69 ,71 and AEs21 ,59 ,61 ,73 ,74 ,76 were other key issues that appeared to challenge patients’ ability to engage in proper medicine use. Some participants cited how AEs inhibited them to engage in proper medicine use (see quotes 31and 32),76 ,61 and others reported that inconvenience of some dosage forms were impeding reasons to engage in proper medicine use.62
Individuals’ general attitude towards medicine (behavioural beliefs)
This subtheme reflected the way individuals evaluated the favourability of medicine use and healthcare-seeking behaviour relating to them. Studies detailed individuals’ attitudes towards the use of medicines including how they balanced the burden and benefits.29 ,32 ,54–58 ,60 ,61 ,63–67 ,69–71 ,74 ,77–82 Individuals often traded medicines’ benefit for associated burden and underlining consequences of illness.
Individuals’ positive attitudes towards medicines were noticeable across studies.29 ,32 ,60 ,61 ,64 ,65 ,67 ,69 ,70 ,74 ,77 ,78 ,80 Positive attitudes were mostly linked to trust in healthcare providers, positive experiences with medicines, and achievement of desired therapeutic outcomes.29 ,32 ,56 ,58 ,60 ,61 ,64 ,67 ,69 ,77 ,78 ,80–82 Many praised the positive role of medicines in assisting their disease management and controlling their illnesses (see quote 33),56 ,60 ,61 ,63 ,64 ,77 ,78 ,82 and others got a feeling of new hope (see quotes 34 and 35).29 ,56 ,69 ,77 ,80 ,82 It appeared that individuals’ attitude towards medicines also played a key role in persisting with the use of medicines. Some individuals noted that their faith in medicines to control disease and prevent illness consequences,56 ,58 ,61 ,64 ,66 ,67 ,70 ,77 the potential for a better life,32 ,55 ,60 ,64 ,67 ,70 ,80 and the opportunity to fulfil social roles64 ,70 motivated them to be persistent in using their medicines.
However, others held negative attitudes towards medicines61 ,63 ,64 ,66 ,67 ,69 ,71 ,77 ,79 ,81 mainly linked to negative past experience with medicines56 ,63 ,64 ,69 ,71 ,73 ,76 ,77 ,79 ,81 and lack of perceived desired outcomes.29 ,63 ,67 ,71 ,82 Negative past experience influenced individuals’ attitude towards medicine (see quote 36).21 ,58 ,63 ,69 Likewise, for some individuals, lack of desired perceived outcomes was a major issue that shaped their attitudes towards medicines (see quote 37).71 ,82 Being sceptical about medicines’ benefits and concerns about potential side effects, long-term use and dependency on medicine also influenced individuals’ attitude towards medicine.58 ,59 ,63 ,64 ,74 ,81 ,82 In addition, some individuals held preconceived negative attitudes61 ,66 ,68 ,77 ,61 ,79 towards medicine, unrelated to past experiences of burden and lack of desired outcomes (see quotes 38 and 39).68 ,61
Medication-taking practices
The actual act of medicine use was well documented across studies.31 ,54–56 ,58–61 ,63 ,64 ,66 ,69 ,73 ,76 ,77 ,78 ,79 Analysis of the constructs under this theme revealed two major categories of individuals’ lived experience of medicine use; accepting medicines and their corresponding regimen, and juggling medicine such as altering the dose, and stopping or replacing medicine with alternative therapies.
Accepting medicine and following therapeutic instructions
This concept related to willingly accepting medicine use, or being forced into it by the underlining illness. Positive experiences with medicines54 ,55 ,61 including the ability to adapt to the burden of taking medicine,54 ,55 achievement of desired therapeutic outcomes,61 trust in healthcare providers54 ,55 ,60 ,64 ,65 ,69 and understanding of the medicine,54 ,55 ,65 ,61 were common reasons for accepting medicines. Yet, for some, pleasing family members was the reason behind accepting their medicine.56 ,77Confidence in medication therapy and satisfaction with the care enhanced medicine acceptance, especially when decisions were made through direct engagement with the patient.55 ,56 ,58 ,61 ,65 When patient-provider partnerships were perceived to be sincere, individuals’ acceptance of medicines and care plans was enhanced (see quote 40).55 ,66 Some individuals unconditionally accepted their medicine as a result of surrendering to the high desire of controlling the illness and living a better life (see quote 41).55–58 ,60 ,61 ,64 ,70 ,73 ,82 Surprisingly, few others accepted their medicine after disproving their own experiments of ‘what will happen if I stop my medicine’, and observing the consequence of stopping medicine without the prescriber’s knowledge (see quote 42).56
Modifying or altering medicine/therapeutic care plans
Several studies28 ,29 ,31 ,54–56 ,58 ,60 ,62 ,63 ,66 ,69 ,73 ,74 ,76 ,77 ,78 ,79 ,81 described this concept in relation to MRB and individuals’ beliefs about medicines. Intolerable MRB, such as AEs,55 ,60 ,69 ,73 ,74 ,76 ,79 medicine routines,21 ,28 ,55 ,60 ,63 ,78 ,79 medication costs29 ,31 ,61 ,69 ,71 ,74 ,76 and characteristics,54 ,61 ,62 ,69 ,79 inadequate medicine information31 ,54–56 ,58 ,74 ,76 ,79 ,81 and fragmented healthcare,31 ,58 were common reasons for modifying the medication regimen or stopping the medicine. Individuals’ beliefs55 ,74 ,76 ,79 and attitudes56 ,58 ,61 ,63 ,66 ,74 ,76 ,77 ,79 resulted in deviations from the therapeutic care plans.
Reducing or increasing doses, skipping doses or discontinuing or restarting medicines were described as individuals’ ways of evaluating the effect of their own medicines, to discover doses that suited their lifestyle. Many individuals manipulated their medication regimens, particularly when intolerable burden was experienced, or the therapy was perceived as inappropriate, or medicines-related needs were unmet.56 ,77 ,78 ,82 Lack of perceived outcome and fear of potential side effects led patients to perform self-initiated medicine dose adjustments.54 Inadequate information and poor understanding about medicines were other reasons for altering the medication regimen (see quote 43).76 Similarly, intolerable medicine AEs often forced patients to vary medicine use (see quote 44).60 ,61 ,74 ,79 The burden of medicine routines causing variation in medicine use was noticeable especially when it interfered with individuals’ daily life activities (see quote 45).28 ,55 ,71
Social norms,54 ,55 ,74 ,76 ,79 such as the influence of family members, others’ experience and culture, seemed to play a key role in affecting patients’ medicine-taking practices in a positive or negative way. Many individuals manipulated their medicines based on others’ experience and recommendations (see quote 46).54 ,55 ,74 Some held a view that herbal medicines reduce the adverse effect of prescribed medicines, and others relied on traditional medicines and never went back for their medical appointments (see quotes 47 and 48).74 ,76 The potential impact of medicine mismanagement, either due to MRB or individuals’ beliefs, was likely to result in inappropriate or dangerous medication therapy outcomes.
Line of argument synthesis
Despite the advances in medical and pharmaceutical care services in today's healthcare system, patients continued to experience MRB and medication therapy problems in their day-to-day life. Even with the differences in study contexts, our synthesis generated from 34 studies with a total sample of 1144 participants showed considerable similarity of patients’ lived experiences with medicine across different medical conditions. This reflects that there is a need to move towards a more comprehensive understanding of PLEM across medical conditions and healthcare settings. The data revealed well-established evidence of MRB effect on patients’ beliefs and behaviours towards medicine on one hand and patients’ health, well-being and therapeutic outcomes on the other. The MRB impact was reflected as potential causes of non-adherence to care plans in some patients, while in others its effect on negative therapeutic outcomes or unachieved therapeutic goals and harm to patients’ health was evident. All dimensions of MRB appeared to predispose patients to DRPs, either as an antecedent (causing non-adherence),or as a consequence (affecting therapeutic and health outcomes).
Individuals’ personal capacity in managing the burden and their beliefs towards medicine alongside environmental and medication factors determine the intensity of the burden. Individuals continue to exert efforts to manage and control MRB. Despite the sustained nature and interference of the burden in daily life, some continue their medicine at the expense of compromised physical, social, financial, or psychological well-being. Additionally, individuals who experienced the interference of MRB in daily life over time begin to juggle their medicine, ending up with potentially inappropriate medicine use practices. Despite the burden concerns, PLEMs are often forgotten, not listened to, and in some cases ignored by healthcare providers, allowing patients self-initiated inappropriate medicine management, resulting in negative therapeutic and health outcomes.
Implications for practice and research
Our review suggests that sound medication therapy decisions cannot be made without good insight and attention to PLEMs. Hence, actively exploring and engaging PLEM when making therapeutic decisions may help provide individualised care. This will occur through understanding a patient's medication-related needs, and identifying and prioritising particular medication therapy problems that a patient may experience as a result of encountered MRB. Resolving MRB may have added value in improving an individual's medication therapy outcomes, and health-related quality of life. PLEM may also serve as a foundation to generate a patient-centred measure used to assess medication-focused services or interventions impact on patients’ health outcomes or behaviour towards medicine. There appears to be a need to develop a patient-generated outcome measure of MRB for routine clinical practice. Such a measure could be integrated with a patient's medication records, facilitating comprehensive medication review.
Discussion
This work is the first metasynthesis to explore MRB and PLEM. Previous studies have only focused on particular aspects of patients’ experiences with medicine. We anticipate that this metasynthesis may improve understanding of the PLEM, the complex nature of MRB, and its impact on patients’ medication therapy and health outcomes. This metasynthesis offers a comprehensive conceptual model for PLEM, which provides medication-related areas requiring emphasis for successful medication therapy decisions and outcomes, in addition to areas that require further research. Themes included in the framework are related. For instance, adequate family support and a patient–practitioner partnership has the potential to minimise some dimensions of patients’ MRB which, in turn, has a positive influence on beliefs, behaviour towards medicine and therapeutic outcomes. From this review, we noticed that MRB is a negative experience with medicine that can occur at any stage of the medication taking. MRB could be minor and manageable, or extensive and awkward, affecting individuals’ health outcomes. The encountered burden can be specific or extensive, depending on the patient, medication, underlying illnesses and environmental factors, including healthcare system and social support.
A key message from this metasynthesis is that MRB plays a central role in influencing patients’ health and well-being, beliefs and behaviour. The impact of MRB on psychosocial, physical and financial well-being was evident. In a continuous process of living with medicines, patients attempted to control and adapt to the hassle associated with incorporating medicine use into their daily life. However, the process of medicines’ routines’ management is challenging, requiring patients’ resources such as time, money and energy. Some patients are successful in adapting to the burden imposed by medicines, while others are unable to do so, and thus, the burden of interference in their day-to-day life influences their well-being, beliefs and behaviour towards medicine and care plans. Lack of, or inadequate family, social and healthcare systems support can limit the patients’ capacity to manage, further exacerbating their burden. The adverse outcomes of treatment burden have also been highlighted in previous reviews.20 ,30 Although there is a difference in the scope, context, number and types of included studies between these reviews and ours, the resonance of results reflects the similarity of lived experiences with medicine among patients with chronic illnesses.
Systemic obstacles of healthcare, lack of established therapeutic relationship, and unacceptable consultation styles can damage patients’ trust in their provider, and confidence in prescribed medicines. Lack of continuity of care generally appeared to influence patients’ adherence to medication therapy. This may be due to diverse, and in some cases, provision of conflicting information, leading to information burden and potentially inappropriate medicine-taking practice. Although medicine costs generally appeared the key healthcare-associated financial burden, others, such as attending multiple facilities and travelling extended distance to and from the facility were also potential factors that intensified the burden and contributed to altered patient behaviour towards medicine. This was more apparent for individuals’ with low socioeconomic status and cultural influence.
Lack of an established patient–practitioner therapeutic relationship had a negative impact on patients’ beliefs about medicine and medicine-taking behaviour. When patients’ trust and confidence in the provider and therapy was negatively influenced, and their expectation and need regarding the medicine was unmet; patients were likely to develop negative attitude towards therapy. This was more common when the partnerships were perceived as unhelpful and unacceptable, when providers did not give their patients adequate time, did not pay them attention, or were unwilling to consider their lived experiences. These individuals preferred to manage their medicines their own way, and over time, they started to juggle their medicine, which may result in negative health outcomes. This resonates with Doyle et al,83 who argued that ‘clinicians should resist sidelining patient experience measures as too subjective or mood-orientated’. Poor patient–practitioner relationships negatively influenced medicine adherence,20 and hence, the success of prescribed medicines outcome.84 Healthcare providers should elicit patients’ concerns about MRB by encouraging them to share their experiences regarding the challenges of the therapy. Likewise, patients also need to make efforts to express their views and perspectives to their healthcare providers.15 Establishing such a relationship may facilitate collaborative discussions,15 ,30 help practitioners to identify the particular MRB encountered, and understand patients’ actual lived experiences so that sound therapeutic decisions can be made. The value of two-way patient–provider interactions, where patients’ experiences are discussed and decisions are shared, contributed to improved patients’ knowledge, satisfaction, therapeutic and health outcomes.15 ,85
There is social burden associated with medicine use. This can be seen as the influence of family members or others on patients’ beliefs and behaviour towards medicine. In addition, medicine use interferences in patients’ social activities is the reality that many patients experience. In routine clinical practice, treatment-related patients’ psychosocial information is often given less consideration than biomedical factors.27 Medication management review should go beyond side effects and toxicities17 ,86 to include psychosocial factors related to medicines use. This may enable practitioners to have an insight into the patients’ context when making therapeutic decisions and care plans.
While in line with a previous study that identified patients’ general dislike to take medicines,87 we found that MRB was a major factor that influenced patients’ beliefs about medicine. In only a few studies did patients hold a preconceived general negative attitude towards medicines and poor health-seeking behaviour. Patients tolerate, control and adapt all events of MRB until the cumulative effect of the burden interference in day-to-day life exceeds their coping threshold and overcomes their controlling capacity. Altering medication therapies either by varying the dose or shifting to alternative therapies appeared to be patients’ rational behaviours in response to the encountered MRB. In our review, many patients made decisions to manipulate their prescribed doses or regimen to manage intolerable MRB and its interference in daily life. Others continued their medicines despite the encountered MRB by trading-off the felt burden with illness consequences. However, this was at the expense of compromised physical, social, financial and psychological well-being. Yet some patients made decisions to continue their medicine after discovering ‘what will happen if I stop my medicine’, and observing the consequences without notifying their healthcare provider. It is known that people conceal adjustments made to medicine taking from their healthcare providers.87
Strengths and limitations
Our review incorporates PLEMs across a broad range of medical conditions. It used systematic searches of multiple databases and rigorous analysis techniques following the methods of metaethnography and a CTA approach. Sensitivity analysis of our initial search approach and the use of two different search strategies reflect the strength and comprehensiveness of our search strategy. Eligible qualitative studies conducted in different contexts of PLEM were combined to achieve a large volume of data across medical conditions. Even though we have included relatively high number of articles in this metasynthesis, the fact that studies were conducted in inter-related topics, and using a combination of metaethnography and CTA technique, made our synthesis process less complicated. This approach facilitated systematic coding of the data and rigorous analysis of concepts from studies. Combining the two methods also ensured the transparency in our data synthesis. We developed a coding framework from second-order constructs in order to code the data. This assisted detailed insight into coded items within each theme and their dimensions, and the overall link between findings across themes. Moreover, the use of a coding framework generated from the study helped us to avoid the risk of forcing the data into a predefined external framework which may have a possibility of some outlying data. To ensure transparency and trustworthiness of the findings, detailed discussions among authors about interpretation of the findings was conducted at each stage. The validity of our data was determined in three ways: critical analysis by independent authors otherwise called ‘investigator triangulation’; citing supporting evidences and quotes of participants from primary studies; and comparing our findings with others. A further strength of this work was linking the three major themes of PLEM using TPB. This helped us to explain how MRB factors influenced patients’ beliefs and medication-taking practices.
Our review included studies from 12 different countries, patients with various medical conditions and medication therapies, and different healthcare settings. Heterogeneity among the studies is inevitable in systematic reviews and there is no standard measure of heterogeneity in metasynthesis. However, a thorough analysis of concepts across studies, and combining emerging concepts to build valid themes is a common approach. The level of overlap in the themes emerging from studies provides good evidence for communality reflecting low impact of heterogeneity. Adhering to metaethnography principles, we reconceptualised the findings of included studies to create new insights beyond those attained from individual studies. Given the interpretive nature of metaethnography, including a wide range of studies helped us generate overarching themes and a conceptual model of PLEM based on a shared communality among the studies. Studies using metaethnographies in healthcare research have successfully synthesised multiple qualitative studies despite their contextual variability.36 ,88–90 Moreover, taking multimorbidity into account accurately reflects the burden experienced by patients.20 Most of the studies we have included were descriptive and used thematic analysis, while a few studies analysed the data based on prespecified theoretical assumptions. We acknowledge that despite the commonality of lived experiences, the specific types of MRB encountered and its magnitude may vary depending on the nature of medicines, medical conditions, patient and environmental factors. For some, medicines characteristic or routines aspects are more burdensome than the number of medicines or adverse effects. For others, getting attentions of healthcare providers is more important than the social burden or medicine costs. While in line with previous work in this field that highlighted positive correlation between treatment burden and number of medicines,24 our analysis of the MRB concept revealed that the burden attributed to medicine goes beyond the number of prescribed medicines. Patients on the same number of medicines may experience different levels and aspects of MRB. However, we have not done subgroup analysis to determine the common types of burden in a specific cohort, medical condition or healthcare setting. We suggest that future research is necessary to explore MRB variation across healthcare settings, medical conditions or specific cohorts in order to capture particular types of burden requiring more attention. Our review also highlighted individuals’ attitude and beliefs about pharmaceutical therapy as a class from perspectives of consumer-encountered burden. Despite the communality, individuals’ beliefs about a particular medicine or group of medicines may vary from individual to individual, across medicine types and medical conditions. We suggest future studies to further investigate, both qualitatively and quantitatively, individuals’ belief variations across medical conditions and medicine types to identify the particular medicine or group of medicines towards which individuals commonly hold negative beliefs to make informed decisions. Despite the comprehensiveness of our search concepts and the broad range of databases searched, some conceptually rich studies might have been missed. Our search was limited to English language studies published from the year 2000 onwards. Although we have included studies on patients’ beliefs about medicine and medication-taking behaviour if MRB was explored as a domain, our search strategy did not include many terms related to medication adherence or non-adherence. Hence, some potential articles on medication adherence that may have medication burden concept as a barrier to adherence might have been missed. Despite these limitations, our study explored the burden attributed to medicines use and highlighted the importance of understanding PLEM during therapeutic decisions. Although the findings are limited to the experiences of individuals involved in the included studies, the comprehensive conceptual model of PLEM can be transferable across a wide range of medications and medical conditions.
Conclusion
This metasynthesis uncovered the shared communality of PLEM among the studies. MRB plays a central role in influencing patients’ health and well-being, beliefs and behaviour towards medicine. Given the complexity of MRB and its impact evident from this review, there is a need for healthcare practitioners to have insight into PLEMs in therapeutic care plans. Understanding PLEM is an opportunity for practitioners to identify particular MRB that patients encounter, and provide individualised care through selection of therapeutic care plans that suit a patient's life. This may assist in helping to achieve patients’ medication-related needs, and improve medication therapy and health outcomes.
Acknowledgments
The authors wish to thank The University of Sydney medical library and librarian, Mrs Loraine Evison, for her assistance during searches of the databases.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
- Data supplement 4 - Online table 3
- Data supplement 5 - Online table 4
- Data supplement 6 - Online table 5
Footnotes
Contributors MAM developed the review protocol and designed the review questions, carried out database search, articles evaluation and screening, data coding and synthesis, and manuscript write up. RJM participated in protocol development, database search, articles evaluation and screening, data coding, synthesis and interpretation and reviewed the manuscript. TFC participated in protocol development, conceptualising the review, designing review questions and database search, articles evaluation and screening, data coding and synthesis and interpretation and manuscript review.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.