Article Text

Abstract
Objective We aimed to compare patient’s and physician’s ratings of inhaled medication adherence and to identify predictors of patient-physician discordance.
Design Baseline data from two prospective multicentre observational studies.
Setting 29 allergy, pulmonology and paediatric secondary care outpatient clinics in Portugal.
Participants 395 patients (≥13 years old) with persistent asthma.
Measures Data on demographics, patient-physician relationship, upper airway control, asthma control, asthma treatment, forced expiratory volume in one second (FEV1) and healthcare use were collected. Patients and physicians independently assessed adherence to inhaled controller medication during the previous week using a 100 mm Visual Analogue Scale (VAS). Discordance was defined as classification in distinct VAS categories (low 0–50; medium 51–80; high 81–100) or as an absolute difference in VAS scores ≥10 mm. Correlation between patients’ and physicians’ VAS scores/categories was explored. A multinomial logistic regression identified the predictors of physician overestimation and underestimation.
Results High inhaler adherence was reported both by patients (median (percentile 25 to percentile 75) 85 (65–95) mm; 53% VAS>80) and by physicians (84 (68–95) mm; 53% VAS>80). Correlation between patient and physician VAS scores was moderate (rs=0.580; p<0.001). Discordance occurred in 56% of cases: in 28% physicians overestimated adherence and in 27% underestimated. Low adherence as assessed by the physician (OR=27.35 (9.85 to 75.95)), FEV1 ≥80% (OR=2.59 (1.08 to 6.20)) and a first appointment (OR=5.63 (1.24 to 25.56)) were predictors of underestimation. An uncontrolled asthma (OR=2.33 (1.25 to 4.34)), uncontrolled upper airway disease (OR=2.86 (1.35 to 6.04)) and prescription of short-acting beta-agonists alone (OR=3.05 (1.15 to 8.08)) were associated with overestimation. Medium adherence as assessed by the physician was significantly associated with higher risk of discordance, both for overestimation and underestimation of adherence (OR=14.50 (6.04 to 34.81); OR=2.21 (1.07 to 4.58)), while having a written action plan decreased the likelihood of discordance (OR=0.25 (0.12 to 0.52); OR=0.41 (0.22 to 0.78)) (R2=44%).
Conclusion Although both patients and physicians report high inhaler adherence, discordance occurred in half of cases. Implementation of objective adherence measures and effective communication are needed to improve patient-physician agreement.
- asthma
- medication adherence
- discordance
- logistic models
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Data from two multicentre studies with a similar design conducted at 29 secondary care outpatient clinics.
Estimates of inhaled medication adherence were only based on Visual Analogue Scales, but these simple measures could be easily implemented during medical visits.
Patient and physician estimates of adherence were not compared with objective data and were assessed only at one time-point.
Predictors of discordance were identified in a multinomial model, but results may not be generalisable as patients were recruited by convenience sampling.
Background
Inhaled controller medications are the cornerstone of effective asthma treatment,1 with established benefits in decreasing severity and frequency of symptoms as well as exacerbations.2 3 However, to achieve these benefits, daily adherence to the prescribed inhaled medications is of critical importance.
Adherence rates in patients with asthma are known to be low, both in paediatric and adult studies.4 5 Suboptimal adherence to inhaled medication is associated with poor health outcomes, including lack of symptom control, exacerbations, emergency department visits and hospitalisations, leading to disease progression, additional social burden and health costs.6 To improve these health outcomes, it is crucial to promptly identify poorly adherent patients during medical visits,7 enabling physicians to address adherence barriers early and avoiding unnecessary additional diagnostic procedures and adjustments in medication. However, this is quite challenging as there is no commonly accepted approach to assess adherence.
Distinct methods have been used, such as evaluation of medical/dispensing records, use of electronic monitoring devices and reliance on self-reports.8–10 The first two methods have limited feasibility for routine use in clinical practice and resource-constrained settings. Self-reports, although subjective, are still considered one of the preferred methods to continuously monitor adherence as they are simple, cheap and minimally intrusive.11 12 One example is the use of a single item Visual Analogue Scale (VAS), which has shown to provide estimates of adherence comparable with pill counts and dispensing records11 13 and is easily applied during medical visits.14 However, reliance on VAS also has its limitations. Patients tend to overestimate their level of adherence.11 13 Additionally, physicians have been found to be inaccurate in estimating patients’ adherence when using VAS.15 16 These limitations may generate patient-physician discordance and impair the identification of patients with poor adherence. In turn, this might influence patient satisfaction and compromise shared decision making and therapeutic adjustments.17
Evidence is lacking on the degree and characteristics of discordance between patients and physicians in relation to the assessment of inhaled medication adherence. In other chronic diseases, patients’ clinical status, disease severity and age are known predictors of patient-physician discordance regarding medication adherence.18 19 The identification of the level of discordance as well as characteristics associated with patient-physician discordance are essential to delineate effective strategies to maximise patient-physician agreement and improve clinical decisions. Therefore, we aimed to (1) compare patient’s and physician’s ratings of inhaled medication adherence using VAS and (2) to identify predictors of patient-physician discordance.
Methods
Study design
Initial face-to-face visit and 1-week telephone interview data from two prospective observational studies of the Inspirers project were analysed (view online supplementary table 1).20 This project addresses the topic of adherence to asthma inhalers among adolescents and adults with persistent asthma. A convenience sample was recruited between November 2017 and June 2018 at 29 allergy, pulmonology and paediatric secondary care outpatient clinics in Portugal. The studies were approved by the ethics committees of all participating centers. The study is reported according to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.21 Eligible patients were approached by physicians during medical visits. Adult patients signed a consent form. Adolescents signed an assent form, and a parental consent form was also obtained.
Supplemental material
Patients
Patients were included if they had a previous medical diagnosis of persistent asthma, were at least 13 years old (13–17 years adolescents; ≥18 years adults) and had an active prescription for an inhaled controller medication for asthma. All inhaled controller treatments were allowed, and there was no change in any prescribed medication in relation to the participation in these studies. Patients were excluded if they had a diagnosis of a chronic lung disease other than asthma or a diagnosis of another significant chronic condition with possible interference with the study aims.
Patient and public involvement
Patients were not involved in this study.
Data collection
During the initial face-to-face visit, data were collected from both patients and physicians. Physicians answered a questionnaire including: assessment of patients’ asthma control according to the Global Initiative for Asthma (GINA)1; last known value of percent predicted forced expiratory volume in one second (FEV1) and respective date; number of exacerbations, defined as episodes of progressive increase in shortness of breath, cough, wheezing and/or chest tightness, requiring change in maintenance therapy22; use of healthcare resources namely, number of unscheduled medical visits (primary care, secondary care or emergency department) and number of hospital admissions; and length of physician-patient relationship. Physicians also reported on the patients’ current asthma treatment, including inhaled and oral medication, allergen immunotherapy and biological therapy. Medication was grouped by active substance in classes: inhaled corticosteroids (ICS), long-acting beta-agonists (LABA), ICS and LABA (ICS/LABA), long-acting muscarinic receptor antagonists (LAMA), short-acting beta-agonists (SABA), short-acting muscarinic-antagonists (SAMA), anti-leukotrienes, xanthines and oral corticosteroids. Reliever therapy with beta-agonist was classified based on the prescription of SABA and/or LABA and accounting for the type of prescribed LABA, considering that maintenance and reliever therapy (MART) is only recommended with formoterol.1 We stratified reliever therapy into three groups: without prescribed SABA or fast-acting LABA recommended for MART (includes patients prescribed a LABA other than formoterol); with SABA alone (also includes patients prescribed a LABA other than formoterol) and with LABA that allows MART (with or without concomitant SABA). In addition, we classified asthma severity in accordance with GINA treatment steps.1 Patients and physicians independently assessed patient global adherence to inhaled controller medication for asthma during the previous week using a VAS, ranging from 0 (worst) to 100 (best) mm.23 Both filled in their respective VAS in distinct case report forms, without any specific instructions, and at distinct moments, being kept blind to each other’s response.
Demographic data—age, gender, smoking habits—were also collected from patients during the face-to-face visit. Upper airway control was assessed using the Control of Allergic Rhinitis and Asthma Test upper airway (CARAT-UA) subscore.24 The CARAT-UA subscore ranges from 0 to 12 points, with >8 points being indicative of good control.25
Approximately 1 week later, through a telephone interview, patients were asked to characterise the patient-physician relationship, namely if patient’s preferences were considered at the time of inhaler prescription, if they had their inhaler technique reviewed during the last 12 months and if they had a written asthma action plan.
Statistical analysis
Descriptive statistics were used to characterise the sample. Normality of each variable was investigated with Kolmogorov-Smirnov tests and visual analysis of histograms. Inhaler adherence VAS scores were compared by pairing patients and physicians using Wilcoxon signed-rank tests and between adolescents and adults, using Mann-Whitney U tests, both considering patients and physicians scores. Intraclass correlation coefficient (ICC) and Bland-Altman plots were used to assess relative and absolute reliability of inhaler adherence VAS scores from patients and physicians. ICC was interpreted as excellent (ICC >0.9), good (ICC=0.75–0.9), moderate (ICC=0.5–0.75) or poor (ICC <0.5).26 27 Correlations with Spearman’s rho were also used to explore the relationship between patients and physicians VAS scores. Spearman’s rho was interpreted as negligible (0–0.30), low (0.3–0.5), moderate (0.5–0.7), high (0.7–0.9) and very high (0.9–1).28
VAS scores were further categorised using cut-offs of 50% and 80%, generating three VAS categories: low (0–50 mm), medium (51–80 mm) and high (81–100 mm) adherence. These cut-offs are frequently used for differentiation of adherence groups.29–33 To determine the agreement on VAS categories between patients and physicians, the percentage of agreement and weighted Cohen’s kappa were used.34 Cohen’s kappa values were interpreted as follows: <0, no agreement; 0–0.20, slight; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial and 0.81–1.0, almost perfect agreement.34
Discordance was defined as (1) category discordance, classification in distinct VAS categories or (2) value discordance, as an absolute difference in VAS scores ≥10 mm. A difference of 10 mm has been widely accepted as a minimum threshold for clinical relevance.35–37 The direction of the discordance was characterised as physician overestimation of patient’s adherence (higher VAS scores by at least 10 mm or higher VAS category) or, inversely, as physician underestimation (lower VAS scores by at least 10 mm or lower VAS category than the patients’ perspective). Univariate multinomial logistic regressions were used to identify possible patient, disease or treatment characteristics predicting the discordance outcome (0=concordance, used as reference; 1=physician underestimation; 2=physician overestimation). Variables with p<0.25 at univariate analysis and informative variables linked to these variables (eg, last percent predicted FEV1 and respective date) were used in a multivariate multinomial logistic regression.38 When two candidate variables (predictors) were highly correlated, such as patient and physician adherence ratings, only one was included in the model.39 The final model was obtained using a backward stepwise method of variable selection. Adjusted OR and 95% CI (OR (95% CI)) are presented. The overall model was evaluated using the goodness-of-fit tests and the Nagelkerke’s R-square.
Statistical analyses were performed using IBM SPSS Statistics V.25.0 (IBM Corporation, Armonk, New York, USA) and plots were created using GraphPad Prism V.6.0 (GraphPad Software, La Jolla, California, USA). The level of significance was set at 0.05.
Results
Participants
From the 413 patients included in both studies, 395 (96%) had complete data on inhaled medication adherence and were considered in this work. Patients had a median age (percentile 25 to percentile 75) of 28 (16–46) years and were mainly female (61%). Most were on ICS/LABA combination therapy (n=330; 84%) and used only one inhaler (n=265; 67%). According to the GINA classification, nearly half of participants had their asthma not well-controlled (n=184; 47%) and had at least one exacerbation during the previous year (n=195; 49%). Characteristics of the participants are summarised in table 1.
Participants’ characteristics (n=395)
Inhaler adherence—patient reported and physician assessment
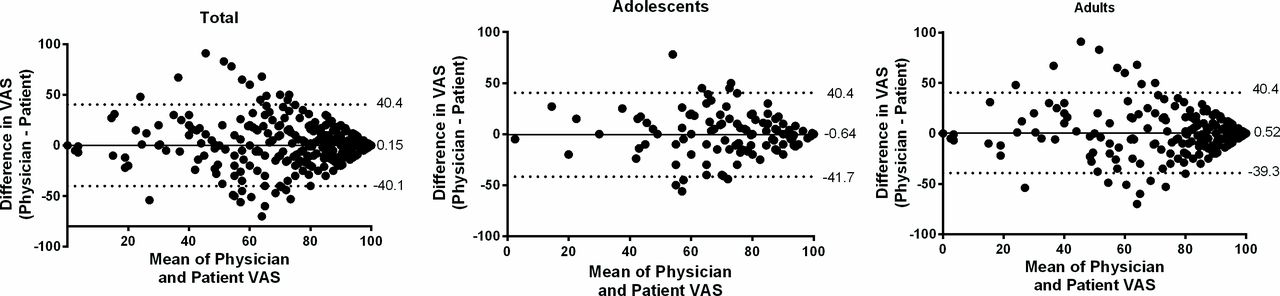
Inhaler adherence was considered high both by patients (median 85 (65–95) mm, VAS>80 53%) and by physicians (84 (68–95) mm, VAS>80 53%). VAS scores were significantly lower in adolescents when compared with adults, in the perspective of both patients (median 80 vs 88, p<0.001) and physicians (median 79 vs 88, p<0.001). The median difference between patients and physicians VAS scores was significantly higher for adolescents than adults (median 11 (5–20) vs 9 (3–20); p=0.025). Correlation between patient and physician VAS scores was moderate (rs=0.580; p<0.001) (figure 1). A lower correlation was found for adolescents (rs=0.462 vs adults rs=0.572). The relative reliability between patients and physicians scores was moderate, with an ICC of 0.63 (95% CI 0.57 to 0.69). Reliability in adolescents was 0.52 (0.38 to 0.64) and in adults 0.66 (0.59 to 0.73). Bland and Altman plots are shown in figure 2. There was reasonable agreement, with bias close to zero and quite large limits of agreement (LoA) (bias 0.15, SD 20.5; 95% LoA −40.1–40.4). Considering the two age groups, a slightly better agreement for adults (bias 0.52, SD 20.3; 95% LoA −39.3–40.4) in comparison with adolescents (bias −0.64, SD 20.9; 95% LoA −41.7–40.4) was found.
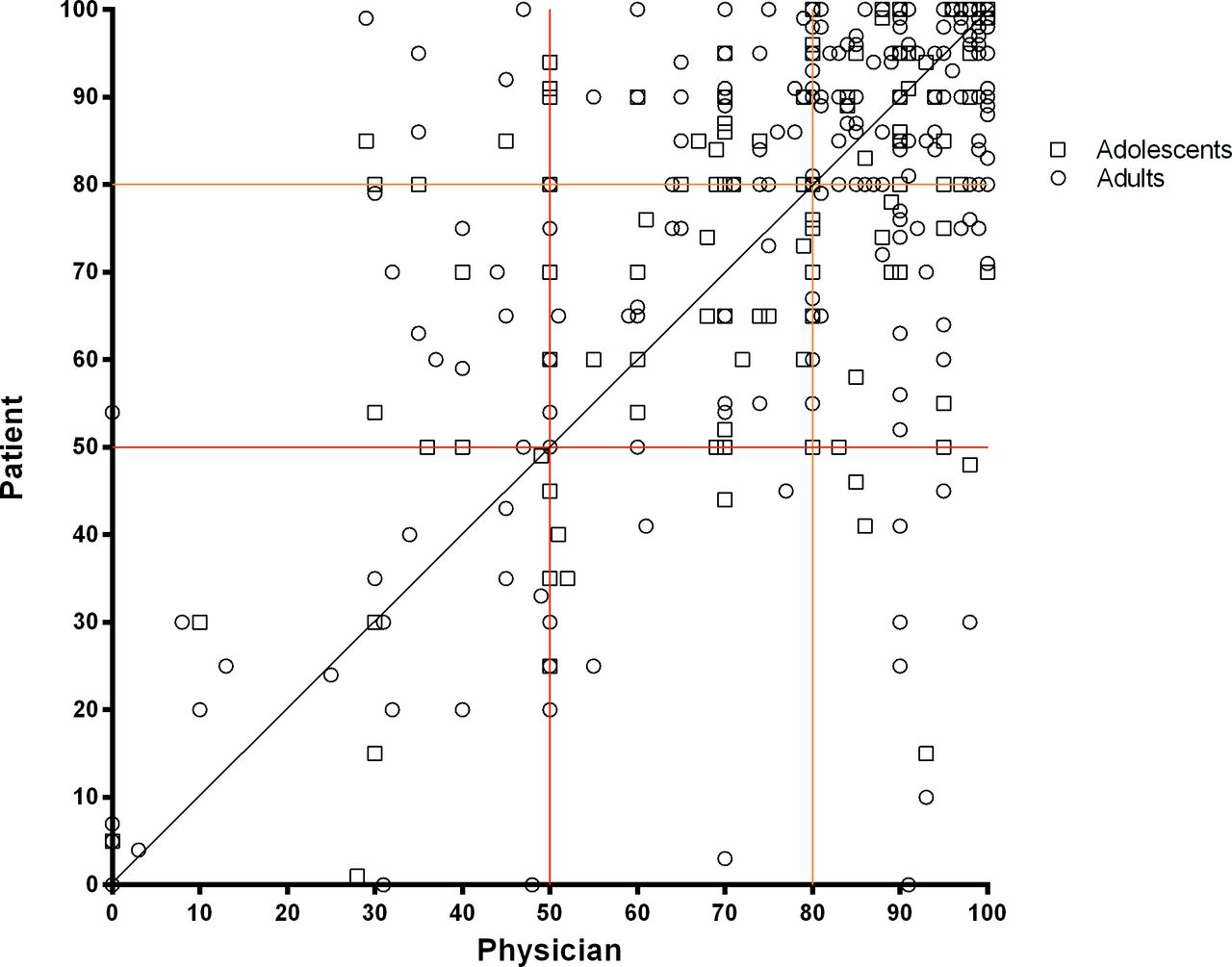
Scatter plot showing the relationship between patients and physicians estimates of inhaler adherence (n=395), with the black line representing perfect agreement; the red and orange lines representing the cut-offs of 50 and 80—in 40% cases both patients and physicians classified adherence to inhaler treatments in previous week higher than 80%, in 15% cases between 51% and 80% and in 9% cases below 50%. Physicians underestimated adherence in 19% and overestimated adherence in 17% of the participants.

{kind=link}
{kind=link}
Bland-Altman plots of inhaler adherence Visual Analogue Scale (VAS) scores between patients and physicians in the total sample (n=395), in adolescents (n=126) and in adults (n=269). The solid lines represent the bias, and the dashed lines show the 95% limits of agreement.
Value discordance was high (n=211; 53%), with physicians overestimating adherence in 26% (n=102) of cases and underestimating it in 27% (n=109). Category discordance occurred in 36% (n=142) of cases, with physicians overestimating adherence in 17% (n=66) of cases and underestimating in 19% (n=76) (table 2). Based on category discordance, a weighted Cohen’s kappa of 0.46 (0.38 to 0.54) (p<0.001) was found, reflecting moderate agreement. The category discordance between patients and physicians was higher in adolescents (41%) than in adults (34%). Weighted kappa was 0.36 (0.22 to 0.50) for adolescents and 0.48 (0.39 to 0.58) for adults, demonstrating a fair and moderate agreement, respectively.
Agreement on VAS categories between patients and physicians (n=395)—64% were in the same category, 30% differed one category and 6% differed two categories
Total discordance occurred in 56% of cases: 78 (20%) based on value discordance only, 9 (2%) based on category discordance only and 133 (34%) classified as discordant using both methods. In 28% of the cases, physicians overestimated adherence and in 27% underestimated it. Unadjusted ORs estimating the association between each variable and direction of physician discordance are presented in online supplementary table 2. Adjusted ORs of the multivariate multinomial model are summarised in table 3. Uncontrolled asthma (OR 2.33 (1.25 to 4.34)), uncontrolled upper airway disease (OR 2.86 (1.35 to 6.04)) and prescription of SABA alone (OR 3.05 (1.15 to 8.08)) were predictors of overestimation. Low adherence rated by the physician (OR 27.35 (9.85 to 75.95)), FEV1 ≥80% (OR 2.59 (1.08 to 6.20)) and a first appointment (OR 5.63 (1.24 to 25.56)) predicted underestimation. Medium adherence as assessed by the physician was significantly associated with higher risk of both physician overestimation and underestimation (OR 14.50 (6.04 to 34.81) and OR 2.21 (1.07 to 4.58), respectively), while having a written action plan decreased the likelihood of discordance (OR 0.25 (0.12 to 0.52) and OR 0.41 (0.22 to 0.78), respectively). Pearson χ2 (p=0.431) and deviance (p=0.721) showed that the multinomial logistic regression model adequately fitted the data. This model explained 44% of the variance in patient-physician discordance and correctly classified 63% of cases.
Multivariate multinomial model to explain physician overestimation or underestimation of patient’s adherence (patient-physician concordance used as reference, n=142, 45%)
Discussion
To the authors’ knowledge, this is the first study investigating patient and physician agreement on adherence to asthma inhalers. We found that although both patients and physicians reported high inhaler adherence, their degree of adherence was discordant in half of the cases. We have also identified in a multinomial model the predictors of this discordance. Uncontrolled asthma, uncontrolled upper airway disease and prescription of SABA alone were predictors of physician’s overestimation of adherence, while low adherence as assessed by the physician (VAS≤50 mm), FEV1 ≥80% and being on a first appointment were predictors of underestimation. Medium inhaler adherence rated by the physician (VAS 51–80 mm) and absence of a written action plan were predictors of both physician overestimation and underestimation.
Self-reported adherence to inhaled medications was found to be high (median 85), which is in line with findings from previous studies on adherence to inhaled medication (mean 90)32 33 and to oral medications (mean or median values between 84 and 100).11 13 19 40–44 Physicians’ perception of the extent of adherence to inhaled medication was also high (median 84 mm), in agreement with prior reports.14 18 42–44 Adherence self-reported by adolescents and assessed by their physicians was lower in comparison with adults. This was somewhat expected as previous research showed that adolescents tend to be less adherent to inhaled asthma therapy when compared with younger children or adults.45 46 Irrespective of the patients’ age, it is possible that both patients’ and physicians’ adherence estimates were overestimating real adherence, as previous research showed lower adherence levels to inhaled medications for asthma when using objective assessment methods4 and overestimation of subjective measures of adherence when compared with objective measures.15 18 47–49 However, in the present study, we did not collect objective data on inhaler adherence to support this assumption.47 This was mainly due to the fact that currently available objective methods (eg, medical/dispensing records, electronic monitoring devices) required laborious analysis by physicians and were costly to implement in clinical practice. There is an urgent need to develop and validate low-cost, ubiquitous and easy-to-disseminate tools to objectively measure inhaler adherence. Mobile applications that allow patients to record their inhaler adherence and share it with their physician may be promising solutions. Some apps with these features are already available, such as AsthmaMD (https://www.asthmamd.org/), Asthma Coach (http://myhealthapps.net/app/details/317/asthma-coach) and InspirerMundi (https://play.google.com/store/apps/details?id=com.bloomidea.inspirers&hl=pt_PT). InspirerMundi app, besides traditional daily self-report of medication intake, has an additional inhaled medication adherence detection tool, using the smartphone camera and advanced image processing, which validates inhaler use through dose tracking.50 The Inspirers research project, in which the present work is included, is developing the InspirerMundi app and plans to assess its feasibility and validity in real-life studies.
Discordance was found in 36% (VAS categories) and 53% of cases (VAS difference ≥10 mm) and fair-to-moderate agreement was found between patient and physician reports. In other conditions requiring daily therapy, such as HIV, similar discordance rates have been found.18 51 This discordant perspective regarding medication adherence is of particular concern as it may limit evaluation and discussion of treatment decisions between patients and their physicians (shared decision making),17 which is likely to have a negative impact on diagnostic and therapeutic decisions such as unnecessary additional procedures and adjustments to medication regimen. In future, implementation of more effective patient-physician communication together with the use of objective adherence measures at the time of the medical encounter may improve agreement.
Irrespective of the method used to define discordance, we found a balance between physicians overestimation and underestimation of inhaler adherence compared with patient self-reported adherence. In studies conducted in other chronic diseases, such as hypertension, osteoporosis or HIV, physicians tended to overestimate adherence.15 18 47 One can speculate that this compared overestimation and underestimation may be related to a higher awareness of the barriers to inhaled medication adherence of physicians treating patients with asthma. However, studies with objective adherence measures evaluating the predictors for physicians underestimation and overestimation of adherence are needed.
The discordance in the perceptions of inhaler adherence may have several reasons. In this study, having a written asthma action plan was associated with a reduction in the likelihood of discordance. If patients and physicians at a certain point of their relationship have agreed on an action plan, they will be more likely to implement effective communication, partnership working and shared decision making during medical visits, which is also reflected in closer estimates of inhaler adherence. Indeed, effective communication was one of the main themes identified by patients as helping the promotion and/or use of action plans.52 In the patients’ view, good communication meant being listened to, feeling respected and having their own knowledge and experience of asthma recognised by physicians during clinical encounters.52 The same argument may also explain why absence of previous patient-physician relationship was associated with underestimation of adherence. Implementation of effective communication in the first visit is challenging, as it is a critical time for a systematic collection of diverse information.53 First visits were also previously linked to greater discordance between patients and physicians.18 53
Other predictors of overestimation were prescription of SABA alone, uncontrolled asthma and uncontrolled upper airway disease. Although in this study we have not quantified the use of reliever therapy, the inclusion of SABA alone in the physician-reported therapeutic plan can be regarded as a proxy of SABA use. These associations suggest that physicians consider patients with poor outcomes or using SABA as being more likely to adhere to the prescribed control inhaler. However, this is contrary to the available evidence showing that SABA can adversely affect adherence to anti-inflammatory treatment and contribute to high levels of poorly controlled asthma.54 Thus, we cannot exclude a possible reverse causality with overestimation itself being a marker of underlying lack of effective patient-physician communication, which might lead to impaired physician perception of the need for control medication adjustments and contribute to worse patient outcomes, including poor disease control and need for SABA. Nevertheless, the estimation of adherence in light of disease control might be highly misleading, as patients could have their disease controlled even with dosages much lower than prescribed, whereas others who take their prescribed medication may not.19 Indeed, some studies demonstrate that asthma control is not directly associated with adherence behaviours.55 56 The same argument may also explain why an FEV1 ≥80%, also related to good asthma control,57 58 was associated with physician underestimation of adherence, suggesting that physicians believe that patients who have better lung function are more prone to forget or reduce medication intake. It is known that, in the absence of objective adherence data, physicians commonly rely on patients’ health status to estimate adherence. This is not exclusive of physicians managing patients with asthma and occurs also in other diseases.15 19 Nevertheless, this is a dangerous assumption that may lead to unnecessary and inadequate changes in the medication regimen.
Our study has some limitations. Although data come from two multicentre studies involving 29 secondary care outpatient clinics, patients were recruited by convenience sampling. Therefore, the findings may not be generalisable to all patients with persistent asthma. Future studies can confirm or negate these results, preferably recruiting patients from different healthcare settings, including primary care, and using consecutive or random sampling. Patient and physician estimates were assessed only at one time-point and based on a single type of measure (VAS). Future long-term studies could use VAS together with other adherence subjective measures, such as the Eight-Item Morisky Medication Adherence Scale,59 and with complementary questionnaires on adherence issues such as medication beliefs60 or knowledge.61 Also, future research could compare subjective estimates with objective adherence measures, ideally simple to use during clinical encounters. When interpreting the agreement between patients and physicians, we need to be aware that kappa is highly sensitive to the distribution of the marginal totals and could produce unreliable results. Also, we need to take into account that each physician rated several patients and a possible physician-cluster effect might have occurred. In addition, as there is no standardised way to define discordance, we used two approaches to define discordance, both based on previously used and generally accepted cut-offs,29–31 35–37 which we believe make our results more robust. Nevertheless, more research is needed on how to define discordance. Regarding discordance prediction, some outcomes of interest occurred frequently (>10%) and this may lead to overestimation of the relative risk. This problem has been identified in cohort studies of common outcomes,62 and thus our results need to be interpreted with caution.
In conclusion, although both patients and physicians report high inhaler adherence, discordance occurs in half of cases. This study has identified some predictors that can help to improve the understanding on this discordance. Implementation of objective adherence measures and effective communication are needed to improve the patient-physician agreement and therapeutic decisions.
Acknowledgments
We thank the participants and centers involved in the project Inspirers. We thank Adelaide Alves, Ana Castro Neves, Anabela Lopes, Andreia Oliveira, Ângelo Afonso, Catarina Parra, Cátia Alves, David Trincão, Diana Pinto, Elena Finelli, Elisa Pedro, Fernanda Carvalho, Filipa Lopes, Joana Borges, Joana Branco, José Ferraz de Oliveira, Liliana Ribeiro, Margarida Valério, Mariana Conde, Marta Pereira, Sara Cabral, Sara Prates and Teresa Almeida for their support in data collection. We thank Rita Amaral for her support in the statistical analyses.
References
Footnotes
Collaborators Inspirers group.
Contributors CJ, AMP, RA, MF-M, MACorreia, CCL, AM, AMA, ATB, JA, PLP, JGM, AGC, LT-B, MFT, RF, JAlberto Ferreira, AC and JAlmeida Fonseca helped design the study. CJ and AMP contributed to statistical analysis. CJ drafted the manuscript. CJ, AMP, RA, MF-M, MC, LA, MP, MACorreia, CCL, MJoana Catarata, LMS, JP, BR, CLopes, AMendes, JCCR, GO, APA, IA, JCarvalho, AMA, JCC, JD, ATB, JA, CR, MA, PLP, NN, AP, JGM, NP, PM, FTB, MAS, AGC, ASN, MS, CLozoya, NS, DS, MJV, LT-B, CC, MFT, RRA, ASM, CSP, PMS, CA, RCâmara, DC, DB, RMF, RF, FM, RGomes, MJosé Calix, AMarques, JCardoso, ME, RGerardo, CN, RCâmara, JAlberto Ferreira, AC, PF, RCorreia and JAlmeida Fonseca contributed to data collection, interpretation and discussion of the results and approval of the final version of the manuscript.
Funding CJ is a post-doc fellow (SFRH/BPD/115169/2016) funded by Fundação para a Ciência e Tecnologia (FCT), reimbursed by Fundo Social Europeu and by national funds of MCTES. This work was funded by ERDF (European Regional Development Fund) through the operations: POCI-01-0145-FEDER-029130 ('mINSPIRERS—mHealth to measure and improve adherence to medication in chronic obstructive respiratory diseases—generalisation and evaluation of gamification, peer support and advanced image processing technologies') cofunded by the COMPETE2020 (Programa Operacional Competitividade e Internacionalização), Portugal 2020 and by Portuguese Funds through FCT (Fundação para a Ciência e a Tecnologia).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The studies were approved by distinct ethics committees (CUF Porto Instituto & Hospital, Centro Hospitalar e Universitário de Coimbra, Unidade Local de Saúde de Matosinhos, Centro Hospitalar Lisboa Norte, Centro Hospitalar Universitário de Lisboa Central, Hospital Beatriz Ângelo, Hospital da Senhora da Oliveira, Unidade Local de Saúde de Castelo Branco, Centro Hospitalar Universitário do Algarve, Centro Hospitalar de São João, Centro Hospitalar Universitário Cova da Beira, Centro Hospitalar Universitário do Porto, Centro Hospitalar de Trás-os-Montes e Alto Douro, Centro Hospitalar Barreiro Montijo, Centro Hospitalar do Médio Ave, Hospital Garcia de Orta, Centro Hospitalar Tondela–Viseu, Serviço de Saúde da Região Autónoma da Madeira, Centro Hospitalar Vila Nova de Gaia/Espinho, Hospital Privado de Alfena) and by the National Data Protection Committee (no 8825/ 2017 and no 11060/ 2017).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data sets generated during and/or analysed during the current study are not publicly available.