Article Text

Abstract
Objective The aim of this study was to evaluate the diagnostic accuracy of bedside lung ultrasound and chest radiography (CXR) in patients with suspected pneumonia compared with CT scan and final diagnosis at discharge.
Design A prospective clinical study.
Methods Lung ultrasound and CXR were performed in sequence in adult patients admitted to the emergency department (ED) for suspected pneumonia. A chest CT scan was performed during hospital stay when clinically indicated.
Results 120 patients entered the study. A discharge diagnosis of pneumonia was confirmed in 81 (67.5%). The first CXR was positive in 54/81 patients (sensitivity 67%; 95% CI 56.4% to 76.9%) and negative in 33/39 (specificity 85%; 95% CI 73.3% to 95.9%), whereas lung ultrasound was positive in 80/81 (sensitivity 98%; 95% CI 93.3% to 99.9%) and negative in 37/39 (specificity 95%; 95% CI 82.7% to 99.4%). A CT scan was performed in 30 patients (26 of which were positive for pneumonia); in this subgroup the first CXR was diagnostic for pneumonia in 18/26 cases (sensitivity 69%), whereas ultrasound was positive in 25/26 (sensitivity 96%). The feasibility of ultrasound was 100% and the examination was always performed in less than 5 min.
Conclusions Bedside chest ultrasound is a reliable tool for the diagnosis of pneumonia in the ED, probably being superior to CXR in this setting. It is likely that its wider use will allow a faster diagnosis, conducive to a more appropriate and timely therapy.
- Cardiac care
- diagnosis
- emergency department management
- imaging
- lung ultrasound
- management
- pneumonia/infections
- respiratory
- ultrasound
Statistics from Altmetric.com
- Cardiac care
- diagnosis
- emergency department management
- imaging
- lung ultrasound
- management
- pneumonia/infections
- respiratory
- ultrasound
Community-acquired pneumonia (CAP) is a major health problem. In the United States CAP is responsible for 1.7 million hospital admissions per year and is the seventh leading cause of death, with an age-adjusted mortality rate up to 22%.1 Core measures that constitute emergency department (ED) care of CAP patients include blood culture collection before first antibiotic administration, administration of initial antibiotics within 6 h of ED arrival and appropriate antibiotic selection.2
An adequate treatment is thus reliant on an early diagnosis of pneumonia, yet the diagnosis is not always clear at presentation to the ED. In a retrospective chart review of patients admitted with pneumonia, 22% of patients presented some reason for diagnostic uncertainty that could result in delayed antibiotics delivery.3
The accuracy of chest radiography (CXR), which remains the daily reference for lung imaging and a cornerstone for the diagnosis of pneumonia according to the American Thoracic Society criteria, is 65% when compared with CT scan.4
Thoracic CT scan is the diagnostic gold standard,5 but may not always be available and is charged with a high radiation dose and high cost that preclude its use in the routine diagnostic process of patients with suspected pneumonia.6
Ultrasound examination is increasingly being used as a valuable bedside method in the diagnosis of various thoracic conditions including pleural or pericardial effusion, empyema, pneumothorax, pulmonary embolism and pneumonia.7
To date only a few studies have investigated the use of lung ultrasound in the diagnosis of pneumonia in the ED or intensive care unit.8–10
The aim of our study was to compare the accuracy of bedside lung ultrasound and CXR in confirming a clinical suspicion of pneumonia in the ED. Although diagnosis at hospital discharge was used as the reference standard, CT scan results were also available for a consistent number of patients.
Methods
Setting
The study was performed at a 90 000 patient/year metropolitan ED (Niguarda Ca' Granda Hospital, Milan, Italy), between September 2008 and October 2009.
Patients
We studied a consecutive sample of adult patients with suspected CAP admitted to the ED during the duties of an emergency physician with experience in lung ultrasound. Signs and symptoms considered as suggestive of CAP were: cough; pleuritic pain; sputum production; fever; dyspnoea; in accordance with American Thoracic Society guidelines.2 All patients were older than 18 years, and were not pregnant. Walking patients with normal vital signs were seen in the fast track area of our ED and were not included in the study; all patients were admitted to a general or emergency medicine ward and were followed till discharge (14±5 days).
Study design
Lung ultrasound was performed by a single expert operator (FC) in patients with suspected CAP as soon as possible after their arrival at the ED and before CXR. CXR was read by a senior radiologist on duty. Further CXR or CT scans were obtained when considered clinically indicated by the senior physician in charge of the patient. Only for study purposes, a second expert radiologist later reviewed CXR that were discordant from lung ultrasound results. Physicians who followed patients and discharged them, and all radiologists, were always blind to ultrasound results.
As ultrasound and CXR are routine examinations, informed consent was obtained only from patients undergoing a CT scan.
We prospectively evaluated all patients until discharge, comparing the ultrasound results with final the diagnosis made by physicians in charge of the patients, on the basis of radiological examinations, clinical evolution, markers of inflammation and microbiology.
Instrumental examination
Anterolateral and posterior scans of the thorax were performed with a convex 3.5–5 MHz probe (Esaote Medical Systems, Firenze, Italy).
All ultrasounds were performed at the bedside by a single expert physician, with longitudinal and oblique (intercostal) scans. The posterior areas were studied in the lateral decubitus or sitting position according to clinical status. The ultrasound execution time cut-off was 5 min.
In agreement with the literature,8 11 12 each hemithorax was divided into five areas: two anterior, two lateral, one posterior, for a total of 10 areas bilaterally. The anterior chest wall was marked off from the parasternal line to the anterior axillary line. This zone was split into an upper region (from the collar bone to the second–third intercostal space) and a lower region (from the third intercostal space to the diaphragm). The lateral area (anterior to posterior axillary line) was split into upper and lower halves. Finally, the posterior area was identified from the posterior axillary line to the paravertebral line.
In normal cases lung ultrasound shows the echoic pleural line, between two rib shadows, and its sliding with breathing; the air-filled lung prevents any visualisation beyond this line.
The wide acoustic impedance between the pleura and underlying areated parenchima creates typical horizontal artifacts defined as ‘A lines’.13
In the presence of variations in the relationship between the aerated and tissue–fluid parts of the lung, vertical artifacts moving with lung sliding arise from the pleural line, reach the edge of the screen and erase A lines.14 These vertical artifacts are called ‘B lines’ and are defined as an interstitial syndrome when exceeding three per longitudinal scan area. B lines correlate with extravascular lung water15 and with tomographic images of interstitial or alveolar–interstitial oedema.16 Interstitial syndrome may be focal (pneumonia, lung contusion) or diffuse (cardiogenic pulmonary oedema, acute lung injury (ALI)/acute respiratory distress syndrome (ARDS), pulmonary fibrosis); history and clinical data, as well as the ultrasound pattern, can help in the differential diagnosis.12 17
In our study an echographic diagnosis of pneumonia was made in the presence of subpleural lung consolidation, presenting a tissular pattern.18
These consolidations may contain dynamic air bronchograms (branching echogenic structures with centrifuge movement with breathing) or multiple hyperechogenic spots (air trapped in the small airway).19 The presence of dynamic bronchogram helps to rule out obstructive atelectasia.20
We also considered as indicative of pneumonia a focal interstitial syndrome. Depending on the ability of patients to stay upright, CXR was obtained in the supine or seated anterior–posterior view only, or in the upright posterior–anterior and lateral views (Siemens Rohere/Tube Optitop 150/40/80 HC 2007). In emergency cases CXR was obtained with a mobile device (Siemens Mobilett XP Hybrid, 083 94 004 Ed. 02; Siemens, Spain). CT scans (Siemens Somatom Definition, 64×2 slices; Siemens, Germany) were always contrast enhanced.
Statistics
Sensitivity, specificity and likelihood ratios of lung ultrasound and CXR were calculated. Student's t test was used for continuous variables while the χ2 test or McNemar test were used for dicothomic variables when appropriate.21
Results
One hundred and twenty patients, of which 77 (64%) were men, with a mean age of 69±18 years, were enrolled in the study. Clinical baseline data, signs and symptoms of patients with and without pneumonia did not differ significantly. A diagnosis of pneumonia at discharge was confirmed in 81 of 120 patients (67%). The final diagnoses of patients without pneumonia are shown in table 1.
Diagnosis at discharge of the 39 patients without pneumonia
Ultrasound and CXR compared with diagnosis at discharge
Considering discharge diagnosis as the reference standard, ultrasound showed a sensitivity of 99% (80/81 patients; 95% CI 93.3% to 99.9%) and a specificity of 95% (37/39 patients; 95% CI 82.7% to 99.4%). The positive likelihood ratio was 19.3 (95% CI 4.99% to 74.2%), the negative likelihood ratio was 0.01 (95% CI 0.002 to 0.09).
The only false negative was a patient with both initial pulmonary oedema and pneumonia, for whom lung ultrasound showed only an alveolar interstitial syndrome. The patient was treated with diuretics, vasodilators and antibiotics with an excellent outcome.
One of the two false-positive patients had a subphrenic abscess with atelectasia of the right lung just above the diaphragm and a small pleural effusion, whereas the other had cardiac failure with pleural effusion and atelectasia.
CXR fared much worse, with a sensitivity of 67% (54/81; 95% CI 56.4% to 76.9%) and a specificity of 85% (33/39; 95% CI 73.3% to 95.9%).
The positive likelihood ratio was 4.3 (95% CI 2.04 to 37.7), the negative likelihood ratio was 0.39 (95% CI 0.20 to 0.76).
Among the 27 patients with a first non-diagnostic radiogram, a second CXR was performed within 72 h in 17 cases and was diagnostic for pneumonia in 10 (total positive CXR in patients with pneumonia at discharge: 64/81). In seven patients with a repeatedly non-diagnostic CXR, pneumonia was diagnosed with a CT scan.
Among the 10 patients who did not undergo further imaging, the discharge diagnosis of pneumonia was based on clinical and laboratory grounds only. Three of these patients had positive but not diagnostic findings at first CXR (pleural effusion in two cases and atelectasia in one). Ultrasound showed consolidations with dynamic air bronchograms in all three cases.
In the remaining seven patients with non-diagnostic findings at first CXR ultrasound was positive for a retrocardiac consolidation.
The first CXR was obtained only in the anteroposterior view in 75% of patients because they were not able to stand upright in the ED. These constituted 92% of the negative results in patients with a discharge diagnosis of pneumonia. In only one case the second radiologist modified the initial result of CXR.
The results of CXR and lung ultrasound compared with the diagnosis at discharge are summarised in table 2.
Results of CXR and lung ultrasound compared with the diagnosis at discharge
The difference in the sensitivities was estimated and tested considering the matched pairs design (table 3). The result (sensitivity (ultrasound)—sensitivity (CXR)=32.1%, 95% CI 21.4% to 42.8%; Mc Nemar test p=2.2×10−7) shows that ultrasound is preferable to CXR.
Significance test of the difference of sensitivity for matched pairs (CXR and lung ultrasound)
Utrasound and CXR compared with CT
A chest CT scan was performed in 30 of the 120 enrolled patients and was diagnostic for pneumonia in 26 cases.
Ultrasound was positive in 25 of 26 patients with CT-confirmed pneumonia (sensitivity 96%, 95% CI 0.89% to 0.99%) and negative in three of four patients without pneumonia.
CXR was positive in 18 of 26 patients with CT-confirmed pneumonia (sensitivity 69%, 95% CI 51.5% to 87.0%) and negative in three of four patients without pneumonia at CT (table 4).
Results of thoracic CXR and ultrasound compared with CT
Ultrasound characteristics and feasibility
The feasibility of ultrasound was 100% and the ultrasound execution was less than 5 min in all patients. The echographic findings of the 80 patients with pneumonia are summarised in table 5.
Lung ultrasound findings
Pneumonia (figure 1) appeared with a pattern of consolidation in 73 cases. Dynamic air bronchograms were almost always present within the consolidation. An interstitial pattern surrounded the consolidation in 42 cases as an expression of perilesional inflammatory oedema. In all cases of consolidation lung sliding was reduced.
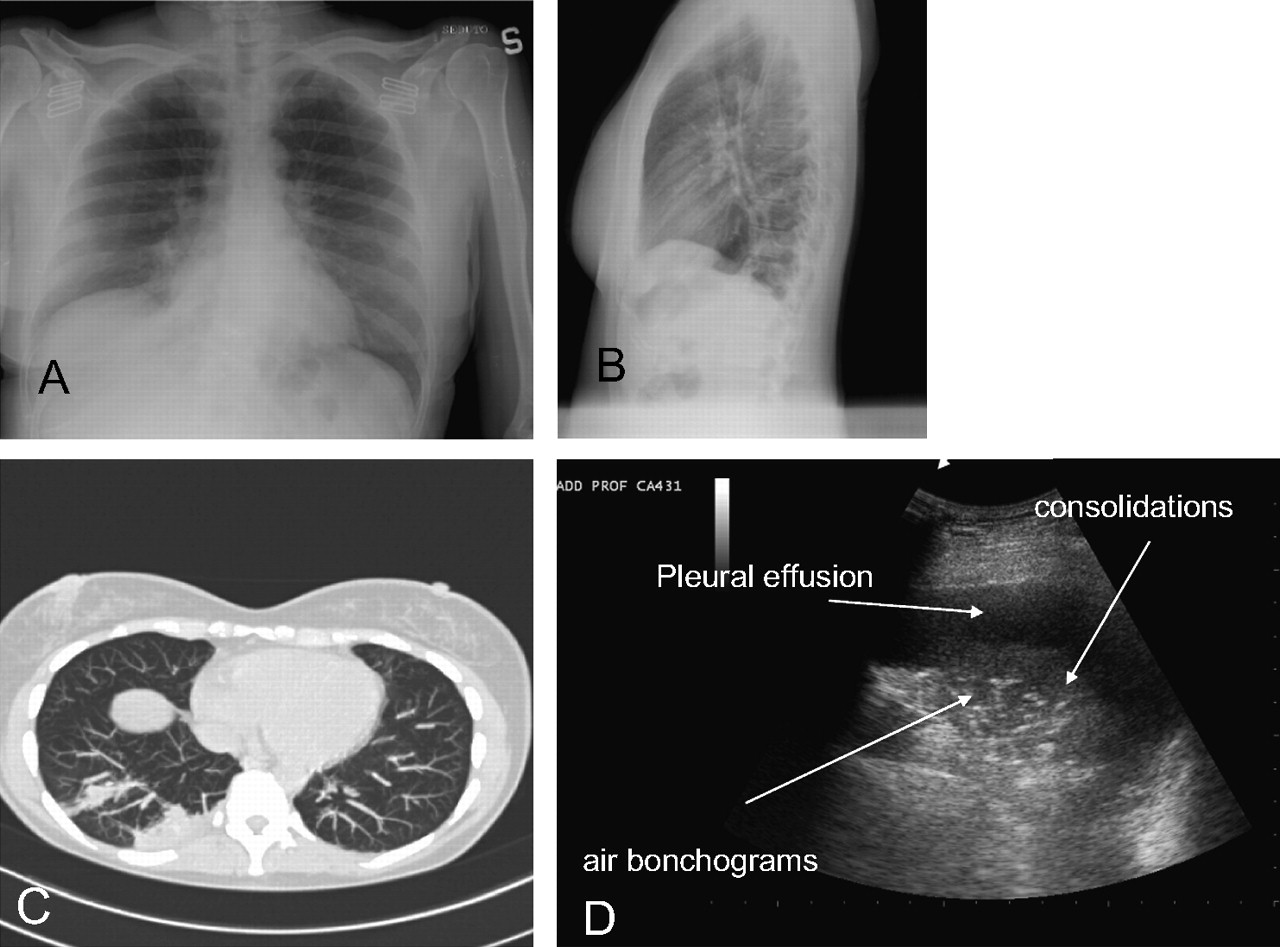
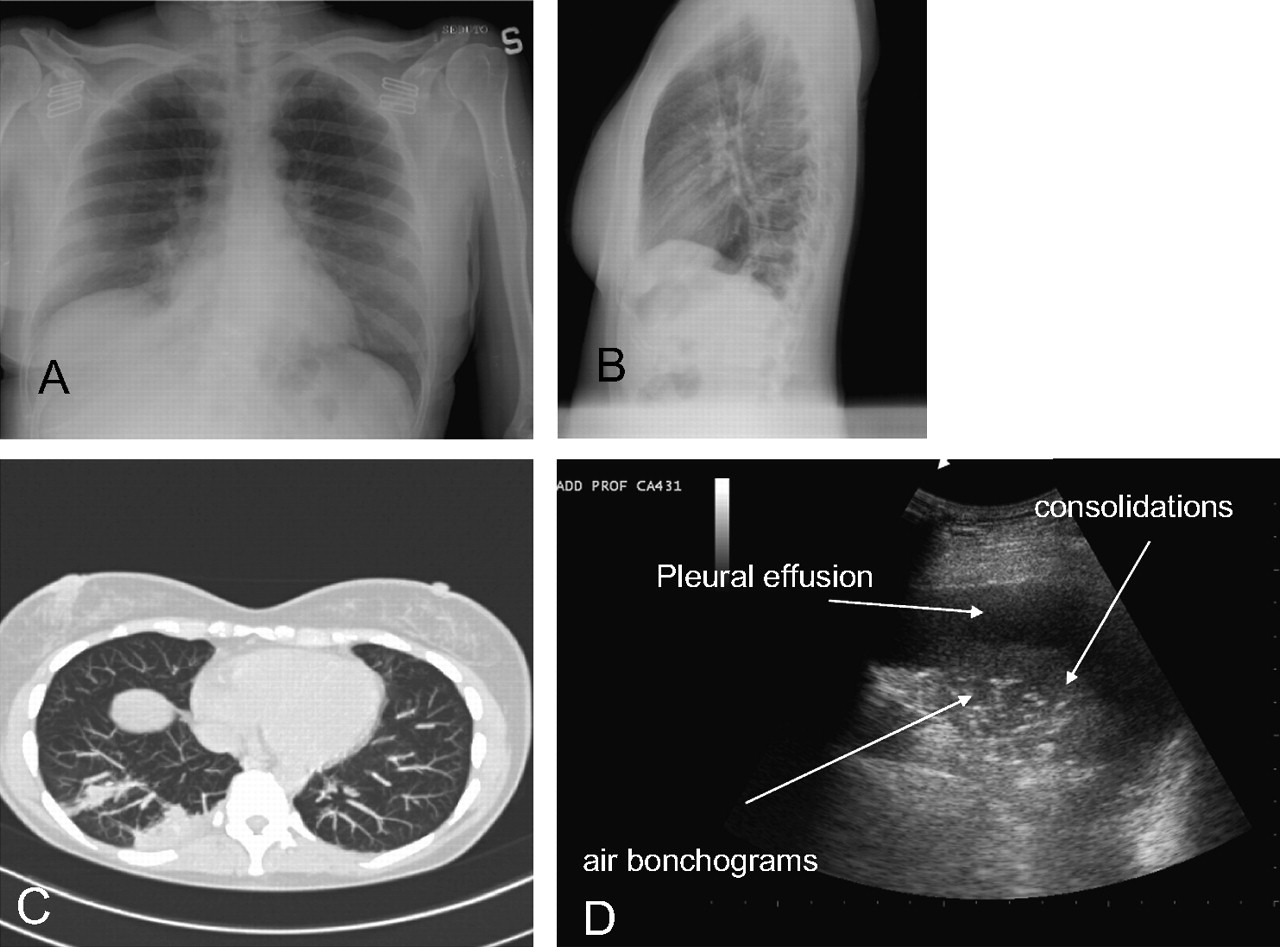{kind=link}
A 45-year-old patient presenting in the emergency department with cough, pleuritic pain and dyspnoea. Double-view chest x-ray showed no sign of pneumonia (A, B). A CT scan (C) confirmed the presence of a right basal consolidation shown by lung ultrasound (D).
An interstitial syndrome was the prevailing pattern in the remaining seven patients (focal and monolateral in three and bilateral in four cases). In all these cases the ultrasound pattern showed irregular and thickened pleura, with reduction of sliding and small subpleural consolidations. In particular the four cases with bilateral involvement had ultrasound findings similar to those decribed by Copetti et al17 in ALI/ARDS. These echographic findings permitted pulmonary oedema to be ruled out.17 The arterial oxygen tension/fractional inspired oxygen of these patients in the ED was between 250 and 300, microbiological data confirmed a primitive pulmonary infection as the cause of the ALI (Klebsiella pneumoniae, H1N1 influenza virus and two cases of Pneumocystis carinii).
Discussion
Lung ultrasound has only recently been appreciated by the greater medical community,22 because for a long time respected sources considered ultrasound to be unfit for assessing the pulmonary parenchyma.23 On the contrary, during the past decade, lung ultrasound has been shown to be a very useful tool in the hands of intensivists and emergency physicians for the diagnosis of pneumothorax, pleural effusions and other thoracic conditions. Its use in the diagnosis of pneumonia has also been investigated in consideration of the great limitations of CXR. This is of particular importance when CXR is performed in the ED, where many patients are critically ill and can be examined only in the supine position, often with bedside equipment.5
The comparative accuracy of ultrasonography and chest radiology has been investigated in one study on patients with ARDS24 and in a few small studies on patients with pneumonia.9 10 25
In their CT controlled study on 32 patients admitted to the intensive care unit for ARDS of different causes and 10 healthy volunteers, Lichtenstein et al24 showed that bedside CXR had a diagnostic accuracy of 47% for pleural effusion, 75% for alveolar consolidation and 72% for alveolar–interstitial syndrome. In the same patients lung ultrasound had a diagnostic accuracy of 93% for pleural effusion, 97% for alveolar consolidation and 95% for alveolar–interstitial syndrome.
Parlamento et al10 came to similar results investigating a series of 49 patients with suspected CAP at first clinical evaluation in the ED. In the group of 32 patients with a confirmed diagnosis of pneumonia, ultrasound was positive in 96.9% of patients, whereas CXR was diagnostic in only 75%. The eight patients with a positive ultrasound but a non-diagnostic CXR were further studied with a CT scan, which confirmed the presence of pneumonia in all cases. In our study CT scans were not routinely performed in all cases in which ultrasound and CXR results conflicted, but were required by senior physicians in charge of patients (blind to ultrasound results) when considered clinically necessary. In this way it was possible to compare the performance of ultrasound and CXR with CT scan in 30 patients. Once again, chest ultrasound comes out as a more accurate diagnostic tool than CXR, with a sensitivity of 96% in CT controlled patients against 69% of CXR. Similar results are obtained when ultrasound and x-ray imaging results are compared with the discharge diagnosis.
The fact that a high number of CXR (75% of all patients and 92% of the negative CRX with diagnosis of pneumonia at discharge) have been taken in the supine position with a single anteroposterior view might partly explain the bad performance of x-rays in the ED setting. Nevertheless, seven out of 10 of the repeated x-rays who became positive for pneumonia at 72 h were also taken in the supine position.
Ultrasound has a clear advantage over CXR–anteroposterior views in the diagnosis of retrocardiac consolidations. It may also be speculated that an earlier diagnosis is possible with ultrasound due to its higher sensitivity to lung extravascular water, as demonstrated for ARDS and lung contusions.24 26 The diagnostic performance of CXR was in accordance with previous results.4 5 Ultrasound lung consolidation is a non-specific sign of pneumonia because it is also present in lung atelectasia, and differential diagnosis could be difficult. The ultrasound sign that differentiates pneumonia from obstructive atelectasia is the presence of a dynamic air bronchogram in the former case (specificity 94% and positive predictive value 97%).20 The possibility of a dynamic evaluation gives ultrasound an advantage over CXR, and possibily also over CT scan, which cannot always clearly differentiate between the two conditions.25 We found dynamic air bronchograms in 71 of 73 patients. Static air bronchograms can also be present in consolidation. When this is the prevalent pattern within a large pneumonic consolidation, in association with the presence of the ‘lung pulse’ sign, we are facing a major obstruction to air flow and urgent bronchoscopic examination should be considered.27
A minority of patients with pneumonia has a prevalent ultrasound pattern of interstitial syndrome. While a focal interstitial pattern is suggestive of pneumonia, the finding of a bilateral interstitial syndrome of acute onset poses a differential diagnosis with pulmonary oedema or other causes of ALI/ARDS.17 In our series we found four such cases and we used the presence of small subpleural consolidations, the absence or reduction of gliding, the irregularity and thickening of the pleural line, to rule out pulmonary oedema. The ultrasound findings in these four patients were similar to those described by Copetti et al17 in ALI/ARDS; microbiological results supported the final diagnosis of lung infection as the cause of primary ALI.
A pleural effusion was present in 31 of 80 (39%) patients with a final diagnosis of pneumonia and in six of 39 (15%) patients without pneumonia, confirming it to be a non-specific sign.
Limitations
In our study chest CT was performed in a limited number of non-randomised patients. The advantage of ultrasound over CXR was thus not confirmed with reference to the imaging gold standard. In agreement with other authors10 we felt that performing CT in all patients would not be ethically justified, therefore we decided to use hospital discharge diagnosis as a surrogate for CT diagnosis in the wider number of patients that had no clear clinical indication for further imaging. We think that our results are consistent with clinical practice and are unlikely to have been biased by this design.
All ultrasounds have been performed by a single, experienced operator. Although ultrasound diagnosis was established on the basis of objective signs, there are no studies documenting what level of proficiency is necessary for a reliable ultrasound diagnosis of pneumonia. Interobserver agreement among physicians with different levels of experience and proficiency should thus be investigated further. On their sample series of ARDS patients, Liechtenstein et al24 documented 0.74, 0.77 and 0.73 concordance (k) for the detection of alveolar–interstitial syndrome, alveolar consolidation and pleural effusion between two physicians of similar experience.
The ultrasound operator was not blind to the clinical presentation of the patients, which herself was diagnosing as possibly having pneumonia. On the contrary, the radiologist did not see the patients but only a very synthetic report of the their clinical conditions. We cannot exclude that this might have been an advantage for the physician performing ultrasound, but we think at the same time that this fact underscores the usefulness of an imaging procedure that can be performed at the bedside during the very first moments of the evaluation of an acute patient.
Ambulant patients were excluded from our study, we cannot therefore affirm the superiority of chest ultrasound over two views standing chest x-rays in this group of patients.
Conclusions
Bedside chest ultrasound is a reliable tool for diagnosing pneumonia in the ED, probably being superior to CXR in this setting. It is likely that its wider use will allow a faster diagnosis of this disease, conducive to a more appropriate and timely therapy.
Although it is unclear what level of proficiency is required to perform adequate lung ultrasound in the emergency room, the use of this technique by emergency physicians in the differential diagnosis of patients with acute respiratory and cardiovascular symptoms is rapidly expanding. This will probably contribute to a diffuse increase of skills and competence and to the routine use of lung ultrasound in the evaluation of patients with suspected pneumonia in the ED.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Primary survey